

Abstract
BACKGROUND: Endotracheal suctioning is required for mechanically ventilated patients to maintain a patent airway. Studies show that open endotracheal suctioning affects respiratory mechanics and gas exchange. The aim of this study was to compare the effectiveness of hyperoxygenation with FIO2 + 0.20 above baseline and hyperoxygenation with FIO2 1.0 in preventing hypoxemia, and to determine the impact of open endotracheal suctioning on the pulmonary ventilation of critical subjects receiving mechanical ventilatory support.
METHODS: This prospective randomized crossover study was conducted in the ICU. Sixty-eight mechanically ventilated subjects with FIO2 ≤ 0.6 and requiring endotracheal suctioning were included in this study. Open endotracheal suctioning was performed using 2 different intervention sequences: hyperoxygenation of 0.20 above baseline FIO2 (FIO2 + 0.20) and 1.0 hyperoxygenation (FIO2 1.0). Oxygenation was assessed via oxygen saturation as measured by pulse oximetry (SpO2), and changes in lung ventilation were measured via alveolar gas volume (V̇A), alveolar minute volume (V̇A min), carbon dioxide (CO2) production (V̇CO2), mixed exhaled partial pressure of CO2 (P̄ECO2), exhaled tidal CO2 volume (VTCO2), end-tidal CO2 (PETCO2), anatomical dead space to tidal volume ratio (VD/VT), and anatomical dead space volume of each breath (VD) using volumetric capnography, and breathing frequency (f), heart rate, and mean arterial pressure using a multiparameter monitor.
RESULTS: SpO2 levels were significantly higher within interventions (FIO2 + 0.20 and 1.0) 1 min before and after suction. Also, there was a significant increase in PETCO2, P̄ECO2, heart rate, and mean arterial pressure immediately after the procedure compared with baseline, and in VTCO2, only for FIO2 + 0.20. Baseline values were not found to be significantly different between the groups in case of any dependent variable.
CONCLUSIONS: In mechanically ventilated adult subjects, hyperoxygenation with FIO2 + 0.20 above baseline prevents hypoxemia. Also, transient changes in pulmonary ventilation with open circuit suctioning were confirmed by volumetric capnography analysis. (Trial registration: ClinicalTrials.gov NCT02440919).
Introduction
Mechanically ventilated patients in the ICU need maintenance of airway secretion clearance for the preservation of airway patency and the prevention of respiratory tract infection. The presence of the endotracheal tube (ETT) reduces mucociliary clearance and the cough reflex, leading to greater production and accumulation of secretions. These patients are unable to remove their secretions and require endotracheal suctioning1–3 that may result in various complications,1 such as discomfort,4 bronchoconstriction,5 infection,6 injury to the tracheal mucosa and hemorrhage,2 atelectasis,6,7 cardiac arrhythmias and hemodynamic changes2,8,9 among others. Reduced oxygenation2,6,10–13 and pulmonary de-recruitment14 are the complications most frequently reported.
Open endotracheal suction is a classic method for the removal of tracheal secretions that is performed by disconnecting the patient from the mechanical ventilator and then inserting a catheter into the trachea under negative pressure.15 Studies have demonstrated that, in addition to the presence of negative suction pressure, disconnecting the patient from the mechanical ventilator causes a greater fall in oxygen saturation as measured by pulse oximetry (SpO2)11,16–20 and impairs ventilation due to pulmonary de-recruitment,6,11,12,14,18,21–23 these being the major complications related to open endotracheal suctioning.
Disconnection causes the loss of functional residual capacity, impairs pulmonary ventilation, decreases oxygenation, and may induce alveolar collapse and result in the generation of shear forces. Studies have shown that lung volume losses during open endotracheal suctioning are transitory, with different times of lung volume recovery.14,21,23
Changes in oxygenation may be easily evaluated by SpO2, effectively and noninvasively obtained by pulse oximetry. And changes in pulmonary volume can be estimated with a rapid and reliable view of ventilation using volumetric capnography, a safe technique that analyzes the pattern of CO2 elimination as a function of expired volume during each breath. Considered a safe technique, with continuous noninvasive monitoring of alveolar gas,24–26 it has been used in various studies involving physiological information about ventilation, perfusion, and metabolism, and also regarding the diagnosis, prognosis, and effects of therapeutic interventions in mechanically ventilated critical subjects.24,27–31
Hyperoxygenation and hyperinflation methods have been proposed for the prevention of hypoxemia and of impaired ventilation induced by endotracheal suctioning.32–36 Hyperoxygenation is a method used to increase FIO2 above baseline levels, and 100% hyperoxygenation has been the most widely used method.1,4,9,20,37 Exposure to FIO2 of 1.0 in experimental animal models and in humans has revealed potential toxic effects related to the release of large numbers of pro-inflammatory cytokines and to marked microvascular and muscular changes.38,39 In humans, toxic effects can occur by reabsorption atelectasis, hyperoxic hypercapnia, bronchial and epithelial damage, decreased effectiveness of the ciliary epithelium, and bactericidal bronchial function.40 Valença et al39 detected increased numbers of macrophages and neutrophils and oxidative damage in the lungs of rats exposed to FIO2 of 1.0 for 10 min, and Phillips et al41 reported respiratory markers of oxidative stress in healthy volunteers while FIO2 of 0.28 was delivered for 30 min. Although delivery of 100% oxygen for only 30–60 s before the suctioning event is suggested in preparation for endotracheal suctioning,1 these findings reinforce the importance of studying methods of < 100% hyperoxygenation.
The latest guidelines of the American Association for Respiratory Care1 recommend the provision of 100% oxygen, especially in cases of hypoxemia occurring before endotracheal suctioning. However, the real necessity of delivery of 100% oxygen should still be investigated, because lower concentrations of 20–50% or even no supplementation prevented hypoxemia during endotracheal suctioning.1,2,6,10,42
We hypothesized that hyperoxygenation with + 0.20 above baseline FIO2 is as effective in avoiding the loss of oxygenation as FIO2 1.0 hyperoxygenation and that open endotracheal suctioning causes changes in pulmonary ventilation at CO2 elimination regardless of the oxygen level offered. The aim of this study was to compare the effectiveness of hyperoxygenation with + 0.20 above baseline FIO2 and hyperoxygenation with FIO2 1.0 in preventing hypoxemia and to determine the impact of open endotracheal suctioning on the pulmonary ventilation of critical subjects receiving mechanical ventilatory support.
QUICK LOOK
Current knowledge
Open endotracheal suction results in greater impairment of oxygenation with a significant, though transitory, loss of pulmonary volume. Hyperoxygenation strategies prevent hypoxemia, although little is known about the impact of delivery of < 100% oxygen or about ventilatory variable changes after open endotracheal suctioning by VCap.
What this paper contributes to our knowledge
Hyperoxygenation with an FIO2 of + 0.20 above baseline prevents the fall of SpO2, and the variables of VCap can show the transitory nature of pulmonary ventilation changes with open endotracheal suctioning.
Methods
Study Location and Subject Population
The study was approved by the Human Research Ethics Committee of our institution and by the National Unified Research Registry involving human beings (Brasil Platform - CEP/Conep System- CAAE: 11354813.1.0000.5504). Written informed consent was obtained from the legal representatives of the subjects according to resolution 466/12 of the National Health Council and approved by ClinicalTrials.gov-ID:11354813.1.0000.5504-NCT02440919. The study was conducted in the tertiary adult ICU at Santa Casa de Misericórdia, Batatais, São Paulo, Brazil. All consecutive patients needing mechanical ventilation and ≥18 y of age were included during the period from June 2013 to May 2015. Seventy-eight subjects of both sexes with various clinical and surgical conditions were selected. However, 10 were excluded and 68 completed the study and were analyzed. Figure 1 provides a Consolidated Standards of Reporting Trials (CONSORT) flow chart of subject flow through the study.

Flow chart.
Inclusion and Exclusion Criteria
Inclusion criteria were as follows: patients undergoing orotracheal intubation and on mechanical ventilation for >12 h, hemodynamically stable, sedated or not, and requiring endotracheal suctioning according to American Association for Respiratory Care criteria.1 Written informed consent was provided by the closest relative of each patient. Exclusion criteria were: individuals using high doses of vasopressor amines and/or having severe cardiac arrhythmias; with hemoglobin <7 g/dL, impossibility of appropriate monitoring of SpO2, baseline FIO2 ≥0.60, requirement of PEEP of >10 cm H2O, rib fractures, presence of a chest drain, severe bronchospasm, intracranial hypertension (intracranial pressure >10 mm Hg), hemorrhagic disorders, marked degree of gastroesophageal reflux, bullous lung disease, unilateral lung disease, use of a tracheostomy, closed suction system, peak pressure >35 cm H2O, hemodynamic instability with mean arterial pressure <60 mm Hg, central venous pressure (CVP) <6 mm Hg, and no criteria indicating the need for endotracheal suctioning.
Study Design and Data Collection
This was a prospective, randomized, single-blind, crossover study with randomization by drawing lots using opaque envelopes containing sequential interventions: hyperoxygenation with 20% above baseline FIO2 (FIO2 + 0.20) and 100% hyperoxygenation (FIO2 1.0) during the open endotracheal suctioning procedure. To eliminate the carryover effect of the previous treatment, a washout period43 of 5 h was allowed between interventions (Fig. 1). After the subject was placed in the dorsal decubitus position for 20 min with the headrest at 40 degrees, the ETT cuff was insufflated with 24 cm H2O with a cuff pressure monitor (Ambu, Madrid, Spain) and the following variables were determined: tube size, level of consciousness, levels of sedation with the vasoactive drug, indications for the open endotracheal suctioning procedure, ventilatory mode, ventilatory parameters, and hemoglobin and hematocrit in the baseline condition before open endotracheal suctioning in both interventions. The interventions were performed by the senior author and by a physiotherapist, and the occurrence of complications during or after the procedure, such as vomiting, trauma and bronchospasms, was recorded.
The oxygen saturation as measured by pulse oximetry (Dixtal TECME S. A., Córdoba, Argentina) or ear lobe sensor oximetry (Dixtal TECME S. A., Córdoba, Argentina) with the multiparameter monitor DX-2021 or DX-2023 (Dixtal TECME S. A.), was also used as an index of hypoxia. The volumetric capnography variables were obtained with the Dixtal 3012 mechanical ventilator with a monitor and Capnostat 5-Respironics Inc-Novametrix, Murrysville, PA and sensor equipped with a mainstream flow sensor. The following variables were determined: alveolar gas volume (V̇A), alveolar minute volume (V̇A min), carbon dioxide (CO2) production per corrected min under standard temperature and pressure conditions, dry (VCO2-STPD), mixed exhaled partial pressure of CO2 (P̄ECO2), exhaled tidal CO2 volume (VTCO2), end-tidal CO2 (PETCO2), anatomical dead space to tidal volume ratio (VD/VT), and anatomical dead space volume of each breath (VD), and exhaled tidal volume (exhaled VT) was obtained by calculating VD/VT and VD. Heart rate, breathing frequency (f), systolic arterial pressure, diastolic arterial pressure, and mean arterial pressure were obtained with the multiparameter monitor DX-2021 or DX-2023 (Capnostat 5-Respironics Inc. Novametrix, Murrysville, PA). All variables were measured at baseline (immediately before each of the cleaning maneuvers), immediately after and 30 min after the cleaning episodes performed. SpO2 was also measured during each of the cleaning episodes performed in both interventions (1 min before oxygenation, 1 min after each of the 5 procedures for open endotracheal suctioning, and 1 min after oxygenation). At the end of data collection, subjects received the physiotherapy, medical, and nursing care routinely performed in the ICU.
Procedures
All participants were ventilated with a Dixtal 3012 ventilator in the following ventilatory modes: volume control ventilation, assist/control (VCV A/C), volume control synchronized intermittent mandatory ventilation (VC-SIMV) and spontaneous breath with volume guarantee pressure-support ventilation (PSV-VTG). After all inclusion criteria were checked, the subjects were randomly allocated to one of the two sequences. The subjects were placed in the supine position with elevation of the head of the bed to 40 degrees for 20 min, before the baseline measurements and the open endotracheal suctioning procedure.
Open Endotracheal Suction.
The suction procedure was performed using an atoxic, sterile, siliconized polyvinyl chloride size 12 French catheter with a lateral orifice and a bottom orifice, and with a suction control valve (Embramed) for ETT of 7.0–8.5 mm.18,44 The catheter was introduced until it met with resistance and was then withdrawn 2–3 cm with a negative pressure of approximately 150 mm Hg14,45 applied for 15 s with circular movements and with a 60-s interval between 5 insertions performed, according to the recommendations of the latest endotracheal suctioning directives of the American Association for Respiratory Care.1
Hyperoxygenation Technique.
Hyperoxygenation was performed mainly using a Dixtal 3012 ventilator. FIO2 + 0.20 was increased to a value 20% above the baseline value of the subject, and FIO2 was increased to 1.0, 1 min before each of the 5 procedures and 1 min after the open endotracheal suctioning procedure.
Data Analysis
A sample of 23 subjects was necessary for an 80% power considering α = 0.05 (2-tailed), as determined by calculating the sample size in a pilot study with 25 subjects. Data were first analyzed using the Kolmogorov-Smirnov test, with approximation to the normal distribution being accepted, thus validating a parametric procedure. To determine the presence or absence of a significant difference between ventilation modes, the modes were characterized as independent populations, and one-way analysis of variance was used to determine variables that could be grouped. To determine the presence or absence of statistical significance, we used the paired Student t test for comparisons between and within the groups, where the baseline was compared with time immediately after and 30 min after open endotracheal suctioning. Repeated measures analysis of variance followed by the Bonferroni post hoc test was used for the 4 SpO2 measurements during the 5 endotracheal suctioning procedures. For the baseline conditions with non-normal distribution, we used the paired Wilcoxon test. Data are reported as mean ± SD and median, with the level of significance set at P < .05 for all analyses, which were carried out with the aid of SPSS 17.0 for Windows (SPSS, Chicago, Illinois).
Results
The mean age of the 68 adult subjects was 68.0 ± 15.6 y, all fulfilled the inclusion criteria, and none experienced bronchospasm or arrhythmias during open endotracheal suctioning. The characteristics and baseline conditions of the study sample are listed in Tables 1 and 2. The indication for mechanical ventilation was predominantly respiratory, mainly due to COPD and acute respiratory failure caused by pneumonia. Mean duration of mechanical ventilation was 12.0 ± 11.7 d, and mean duration of hospitalization was 15.9 ± 13.2 d. The Acute Physiologic and Chronic Health Evaluation II score was 23.0 ± 8.4 at admission and 23.9 ± 8.1 48 h later, indicating an estimated risk of death of 41–49.7%, and observed mortality was 54%,37 with a rate of discharge from the ICU of 46%.31
Characteristics of the Subjects and Baseline Conditions in the Two Interventions (N = 68)
Comparison of Baseline Conditions of Subjects in the Two Interventions (n = 68)
After the first statistical analysis, the SpO2, heart rate, and mean arterial pressure variables were grouped according to ventilatory mode and analyzed for the total population (N = 68), and the f and VT variables, which could not be grouped, were analyzed in subjects studied in the VCV A/C mode (n = 45).
Changes in Cardiorespiratory Variables
There was significant increase within the groups (FIO2 + 0.20 and 1.0) in heart rate (P < .001 and P = .002), mean arterial pressure (P < .001 and P = .001) and maintenance of f, immediately after the open endotracheal suctioning. Also, there were no significant differences between groups (Table 3).
Changes in HR, Mean Arterial Pressure, SpO2 and Breathing Frequency in the Open Endotracheal Suctioning2 Procedure at Different Time Points
Changes in SpO2
There was a significant increase in SpO2 within groups (FIO2 + 0.20 and 1.0) immediately after the procedure compared with baseline (P < .001 and P < .001) (Table 3). Figure 2 shows the continuous analysis, with maintenance of the values during the 5 suction procedures. Comparison with baseline in both groups showed significant differences at times 1 min of hyperoxygenation and 1 min after the end of the procedure (P < .001 and P < .001). A significant difference between baseline and the 2-min time point was observed only for intervention FIO2 + 0.20 (P < .001). A significant difference was detected between the groups, after hyperoxygenation (P < .001) and at all time points measured between the 5 suction procedures (P = .001, P = .001, P < .001, P < .001), immediately after the procedure (P = .02) and 1 min after it (P < .001). No difference was observed in baseline values or in the values at 2 and 30 min after the procedure.

Changes in SpO2 before and after open endotracheal suctioning at different time points with FIO2 + 0.20 above the baseline value and FIO2 1.0. *P < .001; †P = .02.
Changes in Pulmonary Ventilation
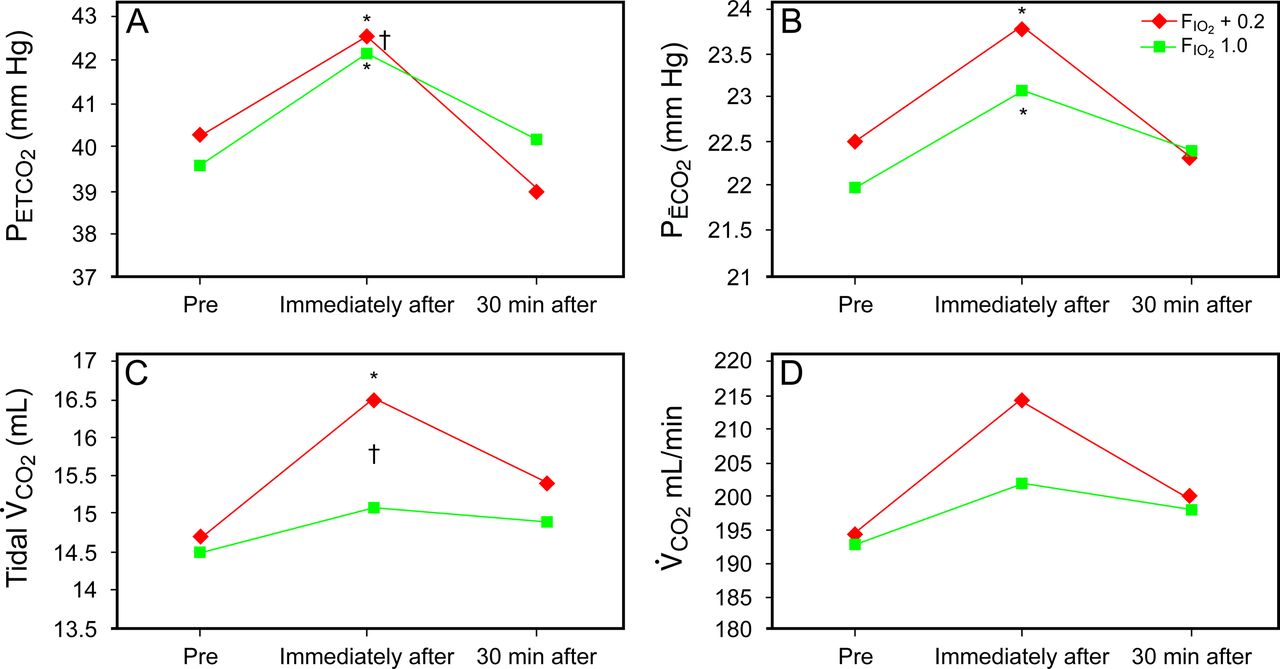
The 45 subjects analyzed for this outcome were in VC-CMV mode, sedated with fentanyl and midazolam with Ramsey of 5 ± 1.15. Immediately after the procedure, there was a significant increase in PETCO2 (P < .001 and P < .001) and in P̄ECO2 (P = .02 and P = .005) in interventions FIO2 + 0.20 and 1.0, and a significant increase in VTCO2 only in FIO2 + 0.20 (P < .001). V̇CO2 increased immediately after interventions FIO2 + 0.20 and 1.0, although without statistical significance (P = .064 and P = .45). V̇A min and exhaled VT were reduced immediately after, although without statistical significance (P = .41 and P = .88), (P = .68 and P = .88), (P = .17 and P = .30), respectively. At 30 min after open endotracheal suctioning, none of the variables studied differed significantly from the preintervention values. Significant differences were found between the groups in PETCO2 and P̄ECO2 immediately after the procedure. Furthermore, there were also no significant changes in VD or VD/VT, between and within the groups (Table 4 and Fig. 3).
Changes of Volumetric Capnography Variables in the Open Endotracheal Suctioning Procedure at Different Time Points3

Changes in PETCO2, P̄ECO2, PECO2, tidal V̇CO2 and V̇CO2 before and after open endotracheal suctioning at different time points with FIO2 of + 0.20 above the baseline value and FIO2 1.0. *Comparison within the groups (pre and immediately after) and †comparison between groups. *P = .001; †P = .038 in A; *P = .02 in B; *P = .001; †P = .038 in C; †P = .033 in D.
Discussion
In the present study, we investigated the effectiveness of hyperoxygenation with FIO2 + 0.20 and 1.0 and the impact of open endotracheal suctioning on pulmonary ventilation. The results indicated that the method of hyperoxygenation with FIO2 of 0.2 above the baseline value in subjects with a previous FIO2 ≤ 0.60 was as effective in maintaining oxygen saturation via pulse oximetry (SpO2) as 100% FIO2 hyperoxygenation, routinely used in clinical practice. We also confirmed the transitory impairment of ventilation reported in previous open endotracheal suctioning studies.6,14,16,18,21,22,23
Using a similar study design, Diniz et al46 also verified the effectiveness of FIO2 0.50 above baseline in preventing hypoxemia in ICU subjects. Similar results have been reported by Rogge et al47 using hyperoxygenation with + 0.20 above baseline FIO2 versus 1.0 FIO2 associated with manual lung hyperinflation in 11 subjects with COPD. More recently Souza et al48 also compared FIO2 of + 0.20 versus baseline FIO2, combined with thoracic physiotherapy and manual lung hyperinflation in 30 critical subjects. Fernandez et al14 reported a similar effect on SpO2 using hyperoxygenation with FIO2 1.0 or without preoxygenation in subjects with mild-to-moderate lung disease, regardless of the type of suction system used, ie, closed, quasi-closed, or open. Moreover, Mohammadpour et al11 detected that SpO2 with preoxygenation of FIO2 1.0 was slightly higher in the closed suction system compared with that in the open endotracheal suctioning, although there were no statistically or clinically important changes with either system.
In the current study, hyperoxygenation with 20% above baseline FIO2 was effective in maintaining oxygen saturation > 95% as determined by pulse oximetry (SpO2) and in preventing unnecessary SpO2 values > 98% using pure oxygen. Jubran et al49–51 considered SpO2 > 92% to correspond to a satisfactory level of oxygenation in mechanically ventilated subjects and limits between 92 and 94% to be targets to avoid SaO2 < 90%, which corresponds to mild hypoxemia, in agreement with the findings of Carruthers and Harrison52 that ruled out respiratory failure with SpO2 > 92% in subjects with severe acute asthma. However, Seguim et al53 detected the absence of hypoxemia only with SpO2 values ≥ 96% in critically ill subjects receiving mechanical ventilation. Torsani et al54 reported that 88 to 92% SpO2 is typically accepted as ideal in clinical practice for critical subjects. However, Ghayumi et al55 recently reported that SpO2 ≥ 94% can be a reliable substitute for arterial blood gas for the assessment of hypoxemia and that arterial blood gas should be limited to subjects with SpO2 < 94%. Based on the present findings, we may state that hyperoxygenation with FIO2 + 0.20 above the baseline value avoids hypoxemia during the open endotracheal suctioning procedure.
In the present study, the ventilation loss expected with open endotracheal suctioning was estimated by the increase in PETCO2 and P̄ECO2 immediately after open endotracheal suctioning, measured by volumetric capnography. Volumetric capnography is especially sensitive to problems affecting the efficiency of ventilation for gas exchange.27 Briassoulis et al56 reported that compact metabolic monitors were reliable for the spirometry records and the metabolic indexes before and after endotracheal suctioning, with no significant changes detected in the pulmonary mechanics of children undergoing endotracheal suctioning. Additionally, volumetric capnography measurements of VD/VT in mechanically ventilated subjects with ARDS are as accurate as those obtained by the metabolic monitor technique.26 In this study, there was no significant difference in VD and VD/VT, measured by volumetric capnography during open endotracheal suctioning.
Regarding changes of pulmonary ventilation during open endotracheal suctioning, studies6,14,16 have shown that closed suction is protective against substantial losses of lung volume. Fernandez et al,14 using inductance plethysmography in subjects with severe lung disease, showed that closed suction and quasi-closed systems reduced the substantial losses of lung volume observed with open endotracheal suctioning and that changes in lung volume are transitory and rapidly reversible, with a similar rate of recovery in both methods. Corley et al18 in a study of mechanically ventilated adult subjects after cardiac surgery using electric impedance tomography, reported that closed suction minimized the loss of lung volume during endotracheal suctioning, but with slower recovery of end-expiratory lung volume (EELV) compared with open endotracheal suctioning. Therefore, an in situ valve between the airway and catheter cleaning chamber should be considered essential in preserving lung volumes and uninterrupted ventilation in mechanically ventilated subjects.22 Mohammadpour et al11 detected a discreet increase in PaCO2, but more significant in open endotracheal suctioning compared with closed suction, both with 100% hyperoxygenation. In our study, there was an increase in PETCO2 and P̄ECO2 regardless of the method. There was also a significant increase in VTCO2 only with hyperoxygenation with FIO2 + 0.20, while a nonsignificant increase in V̇CO2 was observed with both types of hyperoxygenation. This increase may have been related to de-recruitment during open endotracheal suctioning and patient awakening during the procedure.
The present study also confirmed the transience of the ventilatory changes and detected the reversibility of these changes within 30 min, regardless of method of hyperoxygenation with FIO2 + 0.20 or FIO2 1.0. Several previous studies have detected the re-establishment of respiratory mechanics and gas exchange within periods of time of 3–30 min.11,12,32–34,44,46,57
Savian et al32 observed an increase in V̇CO2 with the application of manual lung hyperinflation in subjects under the VC-SIMV mode and in spontaneous modes, which may be explained mainly by disconnection from the ventilator, causing agitation and discomfort. Corley et al22 also detected a significant increase in pulmonary volume and disorders of normal ventilation in subjects under synchronized intermittent mandatory ventilation (SIMV) during pulmonary de-recruitment in manual lung hyperinflation. Liu et al44 demonstrated that open endotracheal suctioning of subjects with acute respiratory failure receiving mechanical ventilation may impair gas exchange and decrease lung compliance under both the pressure control ventilation, assist/control (PCV A/C) and VCV A/C modes, but the effects of endotracheal suctioning on gas exchange were more severe and longer-lasting in the PCV A/C than in the VCV A/C mode. In the present study, we did not compare ventilatory modes; all subjects were in the VCV A/C mode and manual lung hyperinflation was not used, but there was a reduction of V̇A min and exhaled VT, although without statistical significance in both interventions.
Open endotracheal suctioning can also represent a potential factor of psychological stress and irritability in many subjects, caused by anxiety and fear about mechanical ventilator disconnection. Our results also showed a significant increase in heart rate and mean arterial pressure immediately after open endotracheal suctioning as reported in other studies.8,11,19,32 Although significant, the results were discrete and had no risk or clinical impact, which could be attributed to the fact that the protocol followed the guidelines for endotracheal suctioning.1,2,4,45 It should be pointed out that the present results should not be extrapolated to subjects with ARDS and that, in order to minimize the harmful effects of open endotracheal suctioning, in addition to providing hyperoxygenation, the other recommendations of the directives for endotracheal suctioning should be followed, such as precise indication, appropriate catheter, time between suctions, suction pressure, number of procedures, and a strategy of protection against de-recruitment, thus rendering the technique viable and safe.
In a crossover study like this, the issue of how long the period of time between interventions should be is a matter of convenience and a risky decision, even though no significant differences in the interventions were observed at baseline. The decision about washout is always risky, involving the choice between recovering baseline conditions and reducing the chance of changes in the clinical condition of the patient between interventions. The type of sample was also a limitation, because a patient population with more homogeneous clinical characteristics would have permitted a better interpretation of the results. Also limiting was the fact that the influence of the diameter of the suction catheter in relation to the volume of losses of the ETT was not considered.
Additional investigations are needed to compare different ventilatory modes and strategies for the protection of pulmonary volume during and after open circuit suctioning and to determine the impact of the relationship between the diameter of the suction catheter and ETT volume losses during open endotracheal suctioning.
Conclusions
So far, this is the first study demonstrating the effectiveness of the use of hyperoxygenation with FIO2 + 0.20 above the baseline value without association with other techniques in mechanically ventilated adult subjects. Also, VCap variables easily obtained confirmed the effects of pulmonary de-recruitment due to open endotracheal suctioning, based on ventilatory variable changes. Nevertheless, pulmonary ventilation changes were transient and reversible within 30 min, suggesting that the open system may be a safe procedure for subjects without severe lung disease. The effects of hyperoxygenation with FIO2 + 0.20 before suctioning were similar to those observed with hyperoxygenation with FIO2 1.0 in terms of oxygen saturation as measured by pulse oximetry and changes in pulmonary ventilation.
Acknowledgments
The authors acknowledge the entire ICU team from Santa Casa de Batatais and their families. Thanks are also due to Érica Moreira Oliveira for her contribution to the pilot project.
Footnotes
- Correspondence: Jacqueline Rodrigues de Freitas Vianna PT PhD, Av Comandante Salgado, 428 B, Castelo, Batatais, São Paulo, Brazil. E-mail: jacrfvianna{at}uol.com.br.
The authors have disclosed no conflicts of interest.
- Copyright © 2017 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}