

Abstract
BACKGROUND: Mid-frequency ventilation, a strategy of using conventional ventilators at high frequencies, may reduce lung injury but has had limited evaluation in neonates. Hence, a randomized crossover study was designed to assess the feasibility of using mid-frequency ventilation in preterm infants with respiratory distress syndrome.
METHODS: Twelve preterm infants (≥500 g and ≥24 weeks gestational age) who were receiving pressure-limited conventional ventilation with frequencies ≤60 breaths/min for respiratory distress syndrome were randomized to periods of mid-frequency ventilation (conventional ventilation with the fastest frequency up to 150 breaths/min that gave complete inspiration and expiration) or conventional ventilation (frequency ≤60 breaths/min), each lasting 2 h using a crossover design. Ventilator parameters were adjusted to maintain the O2 saturation and transcutaneous CO2 at baseline.
RESULTS: Mean peak inspiratory pressure (15 ± 4 cm H2O vs 18 ± 4 cm H2O, P < .001), Δ pressure (9.8 ± 3.3 cm H2O vs 13.5 ± 3.9 cm H2O, P < .001), and tidal volume (2.6 ± 0.4 mL/kg vs 4.6 ± 0.8 mL/kg, P < .001) were lower, but mean airway pressure (8.9 ± 1.9 cm H2O vs 8.4 ± 1.6 cm H2O, P = .02) and measured PEEP (5.1 ± 0.5 cm H2O vs 4.4 ± 0.5 cm H2O, P < .001) were higher with mid-frequency compared with conventional ventilation. FIO2, gas exchange, and hemodynamic parameters were not affected.
CONCLUSIONS: Based on this small study, mid-frequency ventilation among preterm infants with respiratory distress syndrome is feasible. Further larger and longer duration trials are necessary to validate our findings. (ClinicalTrials.gov registration NCT01242462)
Introduction
Antenatal corticosteroids,1,2 exogenous surfactant therapy,3 and early nasal CPAP4,5 reduce death and death or bronchopulmonary dysplasia in preterm infants with respiratory distress syndrome (RDS). However, the incidence of bronchopulmonary dysplasia among surviving preterm infants is increasing,6–8 in part because of increased survival of at-risk infants. Although nasal CPAP is a better choice for the initial respiratory support for RDS,5 many preterm infants with severe respiratory failure require mechanical ventilation as a rescue therapy.9–11 However, mechanical ventilation may lead to ventilator-induced lung injury and contribute to the development of bronchopulmonary dysplasia.12–14
Reducing volutrauma and achieving patient-ventilator synchrony during mechanical ventilation are lung-protective strategies. One of the ways to reduce volutrauma and improve patient-ventilator synchrony is to increase the ventilator frequency.15 A meta-analysis of the 3 randomized, controlled trials16–18 that compared ventilation strategies with a ventilator rate of 60 breaths/min with strategies at a lower ventilator rate (usually 30–40 breaths/min) showed a reduction in air leaks and a trend toward a decrease in mortality when faster rates were used.15 Preterm infants with RDS often breathe faster than 60 breaths/min.19 Hence, conventional ventilators may achieve lower tidal volumes and better synchrony at ventilator rates >60 breaths/min. Use of ventilators at rates >60 breaths/min (sometimes called high-frequency positive-pressure ventilation) has been reported in neonates20–22 but has not been evaluated in randomized controlled trials.
Mid-frequency ventilation is an alternative mode of ventilatory support aimed at providing the needed minute ventilation at lower tidal volumes and lower peak inspiratory pressures by operating conventional ventilators at higher than normally used ventilator rates.23,24 In the present paper, we classify mid-frequency ventilation (in its present non-commercial form) as PC-IMVs,s (this classification is very common and has many unique names).25 The mode is a form of intermittent mandatory ventilation (IMV) because spontaneous breathing is allowed, although it may not occur at high levels of ventilatory support (eg, the mode in this study was synchronized IMV pressure control on a Puritan Bennett 840 ventilator [Covidien, Mansfield, Massachusetts]). We give it the name “mid-frequency” to distinguish it from the many other forms of PC-IMVs,s and to highlight the fact that it uniquely fits in the range of ventilating frequencies between conventional rates and those used by specialized high-frequency ventilators. Although the principles of mid-frequency ventilation are similar to those of the high-frequency positive-pressure ventilation strategy, several differences suggest that mid-frequency ventilation may be a better lung-protective ventilation strategy. Mid-frequency ventilation allows operation of conventional ventilators at faster rates than used by conventional ventilation (which enables better ventilator-patient synchrony), minimizes auto-PEEP development (reducing adverse hemodynamic consequences), and decreases tidal volume and inspiratory time (gentle ventilation strategy) yet maintains alveolar minute ventilation at low delivered tidal volume (reducing adverse gas exchange consequences). Mid-frequency ventilation has been studied only using adult lung simulators and animal models of ARDS.23,24 Randomized crossover studies using conventional ventilators with a mid-frequency ventilation strategy have not been reported. Therefore, we conducted a trial to study the feasibility of using mid-frequency ventilation to reduce surrogate measures of lung injury in preterm infants with RDS receiving mechanical ventilation. We hypothesized that relative to a conventional ventilation strategy, a mid-frequency ventilation strategy achieves comparable gas exchange at lower Δ pressure, peak inspiratory pressure (PIP), and tidal volume.
QUICK LOOK
Current knowledge
Mid-frequency ventilation is a mode of ventilation characterized by high ventilator rates and low tidal volumes aimed at reducing ventilator-induced lung injury. This is the first trial to apply the concept of mid-frequency ventilation to neonates.
What this paper contributes to our knowledge
Mid-frequency ventilation was feasible in infants with respiratory distress syndrome. Mid-frequency ventilation reduced surrogate measures of volutrauma and barotrauma without compromising gas exchange.
Methods
Study Design
This was a single-center, randomized crossover, trial carried out in the neonatal ICU at the University of Alabama Hospital. Infants were randomly assigned to either conventional ventilation followed by mid-frequency ventilation (CV-MFV group) or to mid-frequency ventilation followed by conventional ventilation (MFV-CV group) based on a random sequence by using serially numbered sealed envelopes, which were opened after the informed consent. Time-cycled, demand flow (variable flow), PC-IMVs,s was provided with Puritan Bennett 840 ventilators with neonatal mode software.
Subjects
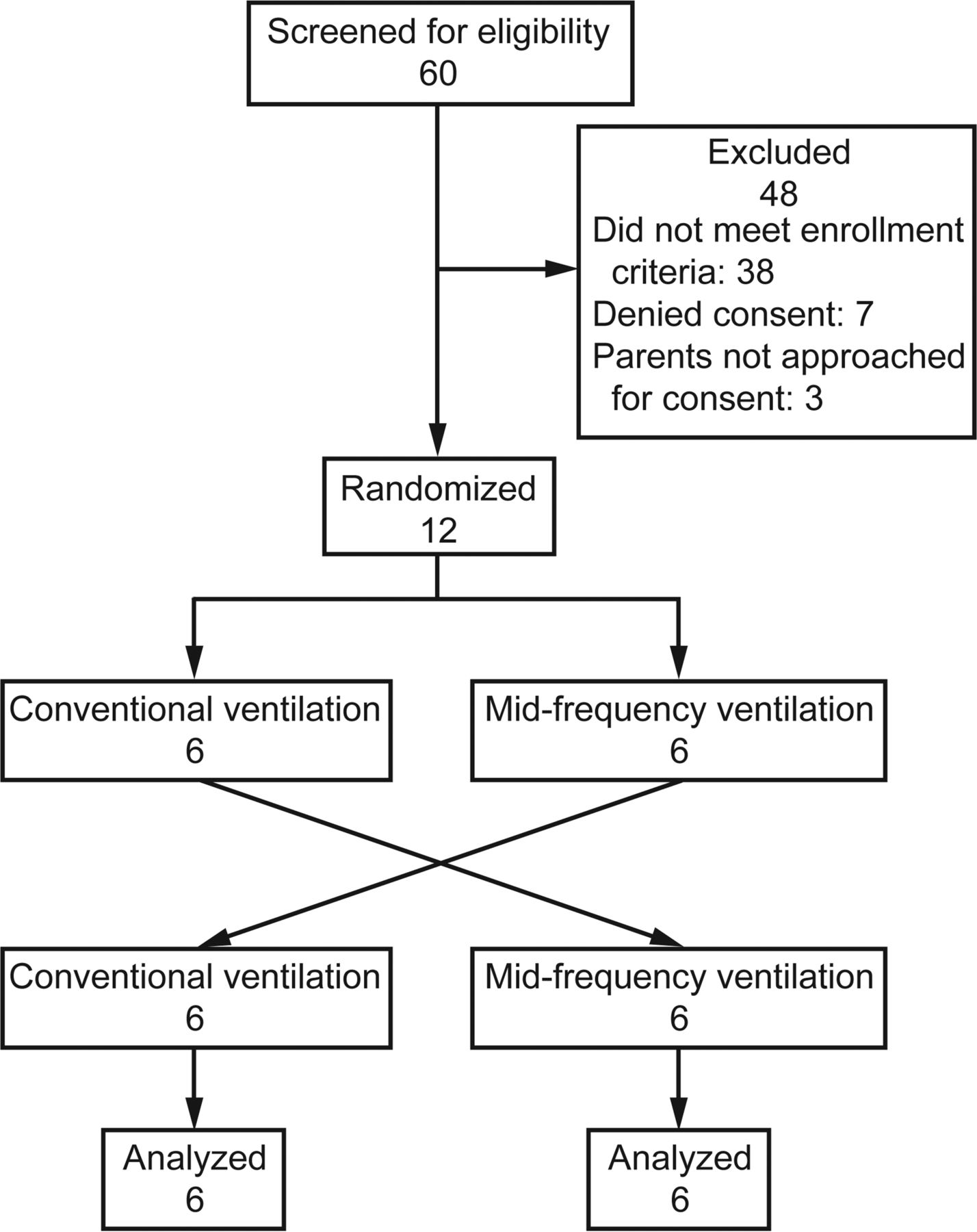
Preterm infants with birthweight of ≥500 g born at or after 24 weeks completed gestation with a postnatal age ≤7 d, had a clinical-radiological diagnosis of RDS, and who were receiving mechanical ventilation after surfactant treatment were eligible (Fig. 1). Infants who were already managed on conventional pressure controlled synchronized IMV with frequencies >60 breaths/min and/or receiving FIO2 <0.3 were excluded from the study. Other exclusion criteria were blood culture-positive sepsis, life-threatening congenital anomalies, cyanotic congenital heart disease, hydrops fetalis, outborn status, and non-viability, as determined by the neonatologist, and those considered too unstable for study enrollment by the attending physician. The institutional review board of the University of Alabama at Birmingham approved the study protocol. The study was registered at ClinicalTrials.gov (NCT01242462). Informed consent was obtained from the mother or legal guardian once an infant was eligible.
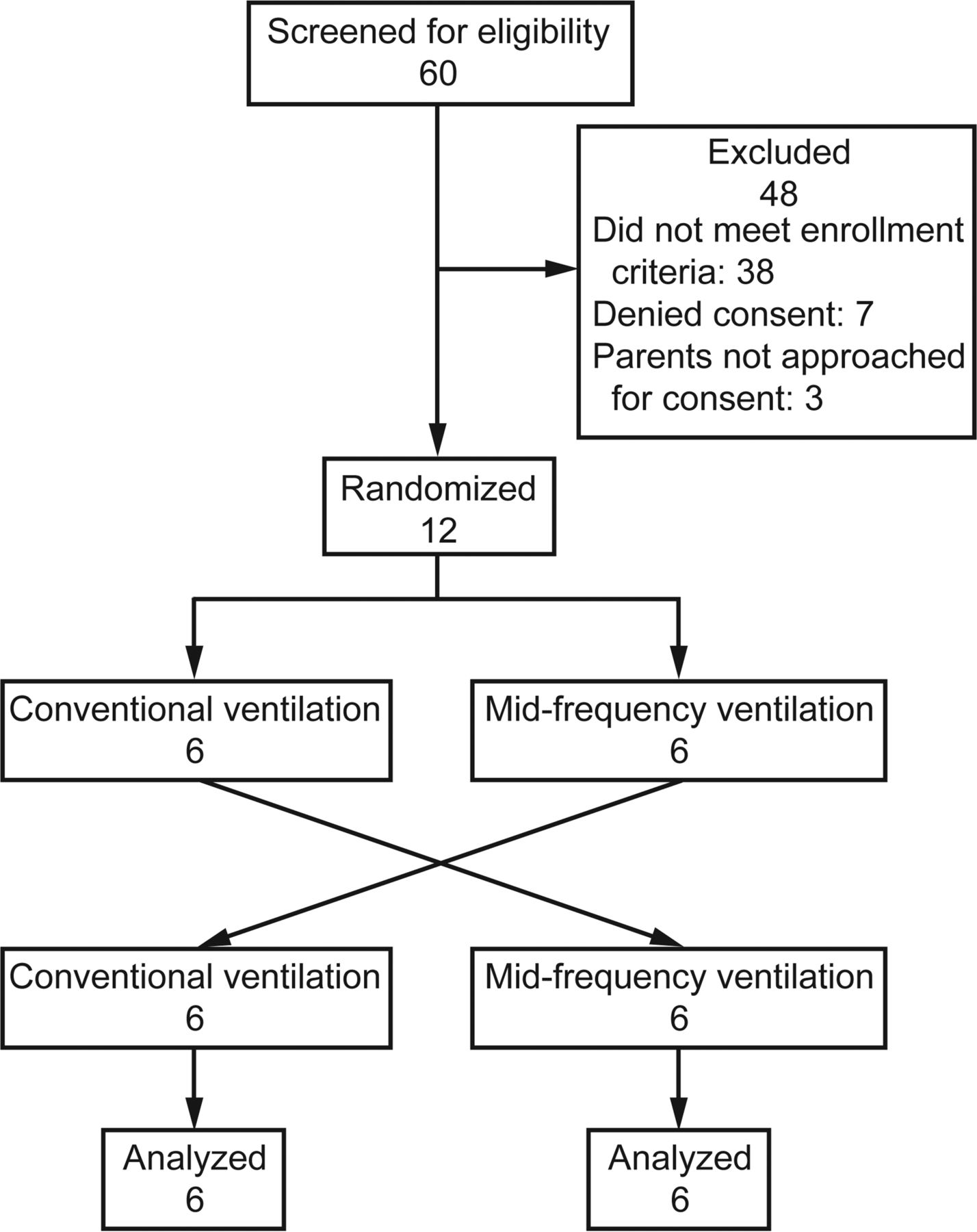
Flow chart.
Before beginning enrollment, ventilator management and other aspects of the care were as per the attending physicians' discretion. SpO2 and transcutaneously measured partial pressure of carbon dioxide (PtcCO2) monitoring (Sentec noninvasive transcutaneous monitor) was used in all infants. SpO2 and PtcCO2 targets were set at 88–95% and 45–55 mm Hg, respectively, during the period of the study. The initial SpO2 and PtcCO2 values during the initial 30-min pretrial stabilization period were considered as baseline values for individual infants.
Interventions
Each infant was in the trial for a total of 4 h after random assignment to either group CV-MFV or group MFV-CV with 2 h in each mode of ventilation (Fig. 2). A time period at the time of crossover, wherein ventilator settings were changed from one mode to the other mode and adjusted to maintain SpO2 and PtcCO2 at baseline, was considered to be the wash-out period. Synchronized IMV pressure control was the primary mode of ventilation during both conventional ventilation and mid-frequency ventilation periods. A constant pressure support of 4 cm H2O was provided throughout the study period. For Puritan Bennett 840 ventilators, inspiratory rise time is measured as percentage of flow acceleration. During conventional ventilation, we used the manufacturer's recommendation of 50% inspiratory rise time, but during mid-frequency ventilation, we used 90% (near maximum) inspiratory rise time to preserve a square pressure waveform and thus maintain tidal volume delivery for short inspiratory times.23 Rise time was kept constant throughout the study periods.

Study algorithm. RDS = respiratory distress syndrome, PC-SIMV = pressure controlled synchronized intermittent mandatory ventilation.
During the period of conventional ventilation, adjustments of ventilator settings were performed to maintain PtcCO2 and SpO2 approximately at their baseline values. If PtcCO2 had increased from baseline, the frequency was increased to not higher than 60 breaths/min initially. If PtcCO2 increased, PIP was increased by 1 cm of H2O to maintain PtcCO2 approximating its baseline value. If the PtcCO2 had decreased from the baseline and FIO2 requirement was <0.4, then PIP was decreased by 1 cm of H2O so as to maintain PtcCO2 at baseline, but if the FIO2 requirement was >0.4, then the frequency was decreased to no less than 40 breaths/min. Thereafter, PIP was decreased to maintain PtcCO2 at its baseline value. For decreasing SpO2 from baseline, FIO2 was increased by 0.05 to a maximum of 0.7; thereafter, PIP was increased in a stepwise manner by 1 cm H2O so as to maintain SpO2 between 88 and 95%. Because moderate baseline PEEP (4–5 cm H2O) was already used, further increase in PEEP was avoided to prevent a negative impact on lung compliance.26 If SpO2 was >95%, FIO2 was decreased by 0.03–0.05 in a stepwise manner to a minimum of 0.4 to maintain target SpO2 of 88–95%. If hyperoxia persisted, the mean airway pressure was reduced by decreasing PIP in a stepwise manner by 1 cm H2O.
During the study period of the mid-frequency ventilation strategy, the optimal frequency for each individual infant was achieved by increasing frequency to the maximum possible, between 61 and 150 breaths/min, with the shortest possible inspiratory time and expiratory time (both with a minimum of 0.2 s) while achieving complete inspiratory and expiratory flows on displayed pulmonary graphics without using an inversed inspiratory-expiratory ratio. Then PIP was adjusted to maintain PtcCO2 at the baseline value by keeping ventilator rate constant. If SpO2 decreased to <88%, FIO2 was increased initially in a stepwise manner by 0.05 each time up to a maximum of 0.7. If SpO2 persisted below 88%, mean airway pressure was increased by stepwise increases in PIP to maintain target level saturation. For SpO2 > 95%, FIO2 was decreased in a stepwise manner to a minimum of 0.4. If SpO2 remained >95%, PIP was decreased by 1 cm H2O to maintain SpO2 between 88 and 95%.
Outcome Variables, Data Collection, and Statistical Analyses
The primary outcome variables in this study were the Δ pressures and tidal volumes. Secondary outcome variables for comparing the 2 modes of ventilation included set PIP, FIO2, mean airway pressures, frequencies, inspiratory times, measured PEEP (recorded from ventilator display), set PEEP, hemodynamic parameters (mean arterial pressure and heart rate), and gas exchange parameters (SpO2 and PtcCO2). Δ pressure was calculated by subtracting measured PEEP from set PIP. A proximal airway flow sensor was not used. Exhaled tidal volumes (corrected to body temperature and pressure saturated) were recorded from ventilator screen display as estimated by the ventilator's internal flow measurement system, taking into account both ventilator circuit compliance and temperature effects. Inadvertent PEEP (at the airway opening) was estimated by deducting the set PEEP from the measured PEEP. Auto-PEEP (in the lungs) was not measured because of potential interference from spontaneous breathing efforts (subjects were not paralyzed). Data on ventilator parameters, hemodynamic parameters, and gas exchange parameters were recorded every 15 min during both mid-frequency ventilation and conventional ventilation periods, and average values for individual infants during each study period were calculated. The average Δ pressure was calculated for individual infants for each study period once baseline blood gas parameters were achieved.
The sample size was based on the following assumption. During the surfactant-treated acute stage of RDS, the usual PIP requirement for a pressure-preset, time-cycled conventional ventilator operating in synchronized IMV is ∼10–20 cm H2O, and the PEEP requirement is 4–5 cm H2O.27 Hence, the Δ pressure requirement will be ∼6–16 cm H2O. Assuming the average Δ pressure to be 12 cm H2O and the SD to be 3–4 cm H2O, 12 neonates were required to detect a 20% change in the Δ pressure when mid-frequency ventilation is used (mean difference of 2.5–3 cm H2O) by paired t test with the power of the study being 80% and α error being .05. The data safety monitoring board reviewed the data after the enrollment of 5 infants.
Descriptive statistics were used to compare the baseline characteristics of the study groups. Unpaired t test or Mann-Whitney test was used to compare the baseline characteristics between the 2 groups. Ventilator parameters and hemodynamic and gas exchange variables between 2 modes of ventilation were compared by using either the paired t test or Wilcoxon test based on the type of distribution. Period and carry-over effects of the first ventilation strategy over the subsequently applied ventilation strategy were evaluated by comparing sums and differences of ventilator, gas exchange, and hemodynamic parameters between the CV-MFV group and the MFV-CV group by using an unpaired t test. Both primary and secondary outcomes were analyzed by 2-tailed statistical tests. Statistical significance was defined as P < .05.
Results
Twelve preterm infants (26 weeks, interquartile range 24–27 weeks; birthweight 792 g, interquartile range 580−1,060 g) with clinical and radiographical evidence of RDS receiving mechanical ventilation were randomized 1:1 into the study. The mothers of all infants received at least one dose of antenatal corticosteroids. Infants were enrolled at a median postnatal age of 2 d (interquartile range 1–2 d). Indwelling arterial lines in place in 8 infants were used to monitor the blood pressures continuously, whereas intermittent cuff blood pressure measurements were used in the other 4 infants. All of the enrolled infants successfully completed the study period of 4 h without adverse events.
Baseline ventilation settings, including ventilation rate, PIP, inspiratory time, tidal volume, and Δ pressure as well as mean PtcCO2 and FIO2, did not differ between the groups (Table 1). Δ pressure decreased during mid-frequency ventilation compared with conventional ventilation (9.8 ± 3.3 cm H2O vs 13.5 ± 3.9 cm H2O, P < .001). Similarly, infants required lower tidal volume during mid-frequency ventilation compared with conventional ventilation (2.6 ± 0.4 mL/kg vs 4.6 ± 0.8 mL/kg, P < .001), whereas FIO2, gas exchange parameters (PtcCO2 and SpO2), and hemodynamic parameters (blood pressure and heart rate) did not change (Table 2). As expected, the frequency achieved during mid-frequency ventilation was faster than the frequency during conventional ventilation (134 ± 7 breaths/min vs 56 ± 8 breaths/min, P < .001). Set PIP during mid-frequency ventilation was lower than during conventional ventilation (15 ± 4 cm H2O vs 18 ± 4 cm H2O, P < .001) (Table 2). The inadvertent PEEP at the airway opening generated during the mid-frequency ventilation period was 0.7 ± 0.1 cm H2O, and measured PEEP during mid-frequency ventilation was higher than during conventional ventilation (5.1 ± 0.5 cm H2O vs 4.4 ± 0.5 cm H2O, P < .001). Mean airway pressure was also higher during the mid-frequency ventilation when compared with conventional ventilation (8.9 ± 1.9 cm H2O vs 8.4 ± 1.6 cm H2O, P = .02). The mean difference was only 0.5 cm H2O, which might not have any clinical importance. Carryover effects in these measures were not observed. Heart rate and mean arterial pressure did not differ between mid-frequency ventilation and conventional ventilation periods. None of the infants required sedatives during the period of mid-frequency ventilation. Chest radiographs were not part of the study protocol. However, subsequently obtained routine radiographs were reviewed, and none of the infants enrolled in the study developed air leaks.
Baseline Ventilator and Hemodynamic Parameters of Enrolled Infants
Comparison of Ventilator, Gas Exchange, and Hemodynamic Parameters Between Mid-Frequency Ventilation and Conventional Ventilation Strategies
Discussion
The results of this trial show that, in comparison with conventional ventilation, mid-frequency ventilation allowed the use of lower Δ pressures and tidal volumes while maintaining adequate gas exchange. PIP and tidal volume, the surrogate indicators of volutrauma and barotrauma, were lower during mid-frequency ventilation. Our results suggest that when fast frequencies are used, lower tidal volumes can provide adequate gas exchange in infants with RDS without hemodynamic impairment.
The application of the mid-frequency ventilation strategy has been tested in mathematical models,23 a high-fidelity adult lung simulator,23 and acute lung injury animal models.24 The feasibility and efficacy of the mid-frequency ventilation strategy using an algorithm to adjust the ventilator parameters to achieve optimal frequency were evaluated in an acute lung injury piglet model.24 Although we incorporated the basic principles of mid-frequency ventilation, our study did not use this algorithm to achieve optimal ventilator frequency. We utilized flow-time graphics displayed on the ventilator monitor and the concept of time constant to reach the ventilator frequency. Hence, optimal frequency in this context was the frequency that minimized the tidal volume while still allowing zero flow crossing during inspiratory and expiratory times. We did not use a constant duty cycle but instead used set constant minimum inspiratory and expiratory times to achieve completed flows. In contrast to the previous study,24 wherein decreased tidal volume was due to extremely short inspiratory time and decreased Δ pressure (partially from generated auto-PEEP), tidal volume was decreased in our study by adjusting PIP, targeting the same baseline level of gas exchange.
Conventional neonatal ventilators can operate at frequencies up to 150 breaths/min. However, a frequency of <60 breaths/min is usually used in clinical practice.28 The reasons for not operating conventional ventilators at higher than conventional frequencies may include progressive decrease in alveolar minute ventilation,20,21 auto-PEEP generation from gas trapping with subsequent overdistention of lungs,29,30 and decrease in the mean airway pressure if adequate bias flow is not maintained.21 Modern ventilators can achieve faster pressurization of the system as long as optimum inspiratory rise time is provided.31 The current study did not show impairment of gas exchange or hemodynamics even at faster frequencies and very low tidal volumes, consistent with clinical,32 animal,24 and experimental laboratory33 studies. We speculate that, although tidal volume was only slightly larger than the anatomical dead space, fast frequencies maintained adequate alveolar minute ventilation.
Improved short-term neonatal outcomes have been reported with the use of conventional ventilators operated at faster frequencies. Randomized control studies comparing rapid (60 breaths/min) versus slow (usually 30–40 breaths/min) frequencies have reported reductions in air leaks (pneumothoraces and/or pulmonary interstitial emphysema) in preterm infants with RDS receiving positive-pressure ventilation with rapid frequencies.16,17 A meta-analysis of the 3 randomized studies showed a significant reduction in pulmonary air leaks and trend toward decrease in mortality with the use of positive-pressure ventilation with a faster rate.15
Algorithm-based adjustments of ventilator settings, continuous monitoring of PtcCO2, and randomized crossover study designs are the main strengths of this feasibility study. The primary outcome variable, Δ pressure, which was determined by deducting measured PEEP from set PIP, serves as a reasonable surrogate for average tidal volume for all types of pressure ventilation modes. The small sample size and short duration are the main limitations of this study. Because this study was performed without using sedation and/or paralysis, an expiratory pause was not used to estimate the auto-PEEP because spontaneous breathing would have interfered with accurate estimation. Hence, total PEEP was not measured in this study; instead, measured PEEP was used as a surrogate for total PEEP. In the absence of esophageal pressure probes, measured PEEP estimation based on ventilator display might have underestimated the total PEEP generated during mid-frequency ventilation. Because the pneumotachograph was not located at the patient end, poor correlation of expiratory tidal volume displayed on the ventilator with the actual expiratory tidal volume is another limitation of the study.34,35 The endotracheal clamping maneuver was not used to estimate the volume lost in the ventilator circuit, which might have overestimated the tidal volume measurement. The generalizability of the study may be limited because infants who were considered too unstable were excluded, and we included only infants with RDS who had a short time constant of the respiratory system and were thus likely to tolerate fast frequencies. Future trials of mid-frequency ventilation could include critically ill infants with RDS or other pulmonary conditions, and a longer intervention period should be tested, now that feasibility has been observed.
Several concerns need to be considered while using a mid-frequency ventilation strategy for neonatal ventilation for a longer duration. Since a short inspiratory time and very low tidal volume are being used, alveolar de-recruitment over the course of ventilation is a concern.36,37 Lower tidal volumes may not result in better neonatal respiratory outcomes because many randomized, controlled trials of high-frequency ventilation (which operates at smaller tidal volumes) have not shown consistent benefits over conventional ventilation.38 Applicability of a mid-frequency ventilation strategy to neonates with varying pulmonary mechanics and varying time constants is another concern because the present study evaluated feasibility only in preterm infants with surfactant-treated RDS. We speculate that optimal frequencies needed to ventilate infants with different lung mechanics would change based on the time constants. With increasing time constants, the proportionate increase in the inspiratory and expiratory times would require relatively lower ventilator rates to enable completed inspiratory flow and to avoid air trapping. Doubling the frequency from baseline has been reported to be associated with increased lung injury in rabbits while being ventilated with conventional ventilators with tidal volumes >10 mL/kg.39 However, mid-frequency ventilation works on a completely different principle, whereby delivered tidal volumes are decreased at higher ventilator rates, and thus, as shown by a lung simulator study,23 overventilation and overdistention are possibly minimized. The potential suppression of spontaneous breathing efforts of neonates at higher ventilator frequency is another possible disadvantage of using mid-frequency ventilation. We believe that the primary advantage of the mid-frequency strategy over high-frequency ventilation is that special devices (such as high-frequency oscillators or jet ventilators) and special operating experiences (as needed while operating oscillators or jet ventilators) are not needed. Thus, a mid-frequency ventilation strategy has the potential to improve cost and convenience but needs to be tested in larger clinical trials before generalization. Whether mid-frequency ventilation is better as primary ventilation or as rescue ventilation has not been determined, but mid-frequency may be superior to conventional ventilation, as suggested by the meta-analysis of the trials using a frequency of 60 breaths/min. Although the mid-frequency ventilation strategy appears safe and promising in this small feasibility trial, routine clinical application of this strategy for neonatal ventilation should not be considered until the efficacy and safety data are available from adequately powered, larger clinical trials.
Conclusion
This crossover randomized trial demonstrated the feasibility of mid-frequency ventilation in preterm infants by using conventional ventilators (Puritan Bennett 840 ventilators). The tidal volume, Δ pressure, and PIP requirements during the mid-frequency ventilation period were lower, whereas the same level of gas exchange as with conventional ventilation was achieved. Because the present study was a small feasibility trial with surrogate outcomes, a meaningful conclusion regarding the clinical importance of the results cannot be stated. Hence, mid-frequency ventilation is a potential lung-protective ventilation strategy, but before considering this strategy for routine clinical application, it should be tested for a longer duration and in varied patient populations to determine effectiveness, safety, and generalizability.
Footnotes
- Correspondence: Waldemar A Carlo MD, Division of Neonatology, 176F Suite 9380, Women and Infants Center, University of Alabama at Birmingham, 619 20th Street South, Birmingham, AL 35233. E-mail: wcarlo{at}peds.uab.edu.
This work was supported by the Perinatal Health and Human Development Research Program of the University of Alabama at Birmingham, and Children's of Alabama Centennial Scholar Fund. Mr Chatburn and Dr Mireles-Cabodevila are the inventors named on the patent for mid-frequency ventilation that is assigned to the Cleveland Clinic. Mr Chatburn has disclosed relationships with CareFusion, Covidien, Dräger, Hamilton, IngMar, Inogen, Invacare, Philips, ResMed, Neotech, and Breathe Technologies. Mr Chatburn also holds US patent 4,589,409. Mr Chatburn received royalties from Amazon.com for books on research and mechanical ventilation. Dr Carlo is on the board of directors of Mednax. The other authors have disclosed no conflicts of interest.
Dr Kelleher presented a version of this paper at the Pediatric Academic Societies 2014 annual meeting, held May 3–6, 2014, in Vancouver, Canada.
- Copyright © 2017 by Daedalus Enterprises









{kind=link}
{kind=link}