

Abstract
Asthma exacerbation is a common reason for children to present to the emergency department. If primary therapies fail to halt the progression of an asthma flare, status asthmaticus often leads to hospital, and potentially ICU, admission. Following the initial administration of inhaled β agonists and systemic corticosteroids, a wide array of adjunct medical therapies may be used to treat status asthmaticus. Unfortunately, the data supporting the use of these adjunct therapies are often unclear, conflicting, or absent. This review will present the physiologic basis and summarize the supporting data for a host of adjunct therapies, including ipratropium, intravenous β agonists, methylxanthines, intravenous and inhaled magnesium, heliox (helium-oxygen mixture), ketamine, antibiotics, noninvasive ventilation, inhaled anesthetics, and extracorporeal membrane oxygenation. Finally, we present a suggested care map for escalating to these therapies in children with refractory status asthmaticus.
Introduction
Asthma is an immune-mediated process in which an environmental or infectious agent triggers a hypersensitivity immunoglobulin E-mediated allergic response, causing mast cell degranulation, histamine release, and activation of pro-inflammatory cytokines.1 The classic triad of asthma is the clinical manifestation of this cascade and involves airway reactivity and bronchospasm, mucosal swelling, and mucus production. The combination of concentric airway swelling and smooth-muscle constriction dramatically increases resistance in the lower airways, resulting in an obstructive process (Fig. 1). Mucus production in the airways adds to the obstructive process, both from potential narrowing of airways with mucus clinging to airway walls and from worsening of air trapping through blockage of airways in a ball-valve mechanism.

Schematic demonstrating asthma pathophysiology. Note the change in the cross-sectional airway from a normal airway (A) to an asthma bronchiole (B), with smooth muscle bronchoconstriction, mucosal edema, and mucus clinging to airway walls.
The mainstays of acute asthma therapy are inhaled β2 agonists and systemic steroids, and often this combination is adequate to break the asthma flare. The β2 agonist (typically inhaled albuterol, but it may also include levalbuterol or salbutamol) is the primary acute treatment, causing an immediate reduction in small airways resistance through bronchial smooth-muscle relaxation and resultant bronchodilation. Corticosteroids, most commonly oral prednisone or prednisolone or intravenous methylprednisone, have 2 distinct mechanisms of action. In the first few hours after administration, glucocorticoids cause upregulation of β-receptors on bronchial smooth-muscle cells, allowing for increased efficacy of β-agonist therapy to reduce bronchoconstriction.2 Following this early effect, the glucocorticoid anti-inflammatory actions lead to decreases in inflammatory cytokines and cause reduced swelling of the airways. In many ways, the anti-inflammatory effect of the steroid reverses the underlying asthma process, whereas other therapies, including β agonists, simply treat symptoms and “buy time” for the steroids to work.
Unfortunately, some patients continue have severe bronchospasm and respiratory distress despite initial treatment with β agonists and steroids. Status asthmaticus and acute severe asthma are common terms used for severe or life-threatening asthma exacerbations in which bronchospasm and respiratory distress persist despite treatment with steroids and multiple doses of a β agonist. Status asthmaticus occurs in approximately 20% of asthma hospitalizations, but the number of children requiring pediatric ICU admission appears to be increasing over time.3–5
Expert guidelines from the National Institutes of Health (NIH) recommend inhaled β-agonist systemic corticosteroid therapy for all asthma flares requiring emergent treatment, with the addition of inhaled ipratropium for severe exacerbations.1 For patients who fail to demonstrate improvement with initial management of β agonists and steroids, a host of other adjunct therapies may be utilized.6 This paper will review many of these adjunct therapies, including the basic mechanisms of action and the evidence supporting their use.
Dosing of Standard Therapies
If patients with status asthmaticus fail to respond to initial treatments, many providers will first escalate the dosage of these first-line therapies above the recommended dosage prescribed in the NIH asthma guidelines. Continuous delivery of a β agonist has become common in the treatment of severe asthma flares. In children, this continuous delivery appears to be more effective than intermittent delivery7,8 and also provides a more efficient use of respiratory therapist and nursing resources.9 The NIH asthma guidelines1 recommend a continuous inhaled albuterol dosage of 0.5 mg/kg/h up to a maximum 15 mg/h; however, 20 mg/h of continuous albuterol is commonly utilized by providers for children of all ages. A few studies have evaluated the use of high-dose continuous albuterol, with doses as high as 75–150 mg/h,10–12 with no clear evidence of benefit over standard dosing. The limiting factor in continuing to increase the dose of albuterol is typically dose-dependent tachycardia. Diastolic hypotension and mild hypokalemia may be seen with increasing doses of continuous inhaled albuterol12,13; however, the clinical importance of these findings is undetermined.
The dosing equivalent of 1–2 mg/kg/d of prednisone (maximum 60 mg) is the recommended steroid dosing regimen for asthma exacerbation in the NIH asthma guidelines1; however, it is also common for many providers to exceed this dose during a severe exacerbation.14 Although some evidence in adults may suggest benefit from early high-dose steroid in the emergency department setting,1 data on systemic steroids remain inconclusive. A 2016 Cochrane review examined 18 pediatric and adult studies using a variety of dosing regimens for systemic steroids and found no clear advantage to any specific regimen.15 It has, however, been demonstrated that early administration of systemic steroids in the emergency department is associated with decreased hospital admission rate.16
Despite the common practice of escalating the dosing of standard therapies in the setting of status asthmaticus, limited data support inhaled continuous albuterol dosing > 15–20 mg/h or steroid dosing > 2 mg/kg/d of prednisone equivalent. Providers should carefully consider and monitor adverse effects of these medicines if they choose to exceed standard dosing regimens.
Anticholinergics
Ipratropium is an anticholinergic agent that causes bronchodilation through its action as an acetylcholine receptor antagonist.17 A 2005 systematic review of 32 randomized studies of ipratropium provided in the initial management of status asthmaticus in the emergency department demonstrated a clear benefit in both children and adults for improving pulmonary function parameters and preventing hospital admissions18; this was confirmed in a 2013 Cochrane review.19 However, once a child is admitted to the hospital, the potential benefit of continued ipratropium therapy is less clear. A randomized trial of 210 children (ipratropium vs control) found an advantage in the ipratropium group for symptom improvement and reduced length of hospital stay; however, this difference was lost once the groups were corrected for confounders.20 A 2014 Cochrane review of 7 randomized studies in children admitted to the hospital for asthma exacerbation also found no benefit for shortened stay to support continuing ipratropium after hospital admission; however, none of these studies evaluated those patients admitted to the ICU.21 At this point, the addition of ipratropium should be considered standard of care for children presenting to the emergency department in status asthmaticus; however, there are not sufficient data supporting their continued use after admission to the hospital, and there are no data evaluating their use in the ICU.
Intravenous β Agonists
A postulated utility of intravenous β agonists in addition to or in place of inhaled β agonists stems from the concept that during a severe asthma exacerbation, severe bronchial constriction may prevent delivery of inhaled β agonists to the distal airways.22 An intravenous β agonist, most commonly terbutaline or salbutamol, may reach β2 receptors in the distal airways via the bloodstream and cause more effective bronchodilation. Because these β agonists are delivered systemically, they are also more likely than inhaled albuterol to produce adverse effects related to interaction with non-airway β1 receptors, primarily tachycardia and jitteriness. This will be even more exaggerated with other, less-specific α and β agonists, such as epinephrine. In addition, if the airway β receptors are already saturated from inhaled albuterol, the addition of an intravenous β agonist may provide minimal supplementary benefit.
A 1997 randomized trial by Browne et al23 of intravenous salbutamol versus saline given to children in the emergency department exhibiting poor response to inhaled salbutamol and steroids demonstrated earlier time to weaning of nebulized therapy and emergency department discharge in the intravenous salbutamol group. Browne repeated the trial in 2002 with earlier randomization and similar results.24 An additional 2007 randomized trial of intravenous terbutaline versus saline added to nebulized albuterol for children presenting to the emergency department with status asthmaticus demonstrated a statistically nonsignificant improvement in clinical asthma scores, time to weaning of nebulized therapy, and time to ICU discharge.25 However, 4 subjects demonstrated some cardiac toxicity of terbutaline, with one displaying cardiac dysrhythmias and 3 cases of elevated troponin levels. Despite the marginal success of these early trials, Cochrane reviews in 2001 and 2012 including children and adults found no significant benefit with the addition of intravenous β agonists to inhaled β agonists.22
More recently, the increased use of long-acting β agonists in the out-patient setting as asthma control agents may affect patients' response to short-acting, rescue β agonists in the acute setting. Chronic exposure to β agonists probably down-regulates the β-receptors in airway smooth muscle, making these receptors less responsive to β-agonist therapy during status asthmaticus episodes. This is one theory explaining the increased rate of death observed in patients receiving daily long-acting β-agonist therapy26; however, there remains some controversy about the cause of increased witnessed mortality in these patients.27,28
β agonists are a mainstay of therapy for acute asthma flares, but the preferred route of delivery remains inhaled β2 agonists. If a patient is unable to receive inhaled therapies, intravenous β-agonist therapy is warranted. However, there remains insufficient evidence regarding the effectiveness of adding intravenous β agonists to inhaled β agonists for acute status asthmaticus. When intravenous β-agonist therapy is coupled with inhaled β agonists, clinicians should monitor closely for adverse effects, including excessive tachycardia and dysrhythmias.
Methylxanthines
Methylxanthines, a drug class including caffeine, theophylline, and aminophylline, are nonspecific phosphodiesterase inhibitors that cause bronchial smooth-muscle relaxation through increases of intracellular cyclic adenosine monophosphate.17 Use of enteral theophylline has waxed and waned in popularity as an adjunct therapy for out-patient asthma management, largely due to narrow therapeutic range requiring monitoring of serum drug levels and other drug interactions due to its metabolism via the cytochrome P450 pathway. However, intravenous aminophylline remains a common therapy in the setting of status asthmaticus. Common adverse effects include tachycardia and nausea, whereas a more significant adverse effect involves lowering of the seizure threshold in patients at risk for seizures.
One theoretical advantage of a methylxanthine as an adjunct to an inhaled or intravenous β agonists is the mechanism of action on a unique receptor. Conceptually, targeting a site other than the β-receptor may provide an additive benefit for bronchial smooth-muscle relaxation. Other proposed mechanisms include improved diaphragm contractility and airway clearance, inhibition of the inflammatory response, and diuretic properties reducing pulmonary edema.6 Unfortunately, the adverse effect profile of methylxanthines has significant overlap with β agonists, and tachycardia in particular often limits the utility of this drug class.
Intravenous aminophylline has been used for status asthmaticus in children for more than 70 years,29,30 with some evidence that the addition of aminophylline improved lung function in these patients. However, randomized trials of intravenous aminophylline or theophylline as an adjunct to albuterol and steroids for status asthmaticus completed in the early 1990s repeatedly failed to show a benefit of this therapy, for both measures of pulmonary function and secondary outcomes, such as length of hospital stay.31–36 Several of these studies also reported increased adverse effects, most commonly nausea and restlessness (including insomnia and tremor). In a 2001 randomized trial, Ream et al37 demonstrated an advantage in the aminophylline cohort for improvement of clinical asthma scores in children admitted to the pediatric ICU who were also receiving corticosteroids, inhaled albuterol, and ipratropium but failed to show a difference in ICU stay compared with those therapies without aminophylline; these findings were later supported by a 2005 Cochrane review.38
Wheeler et al39 compared the efficacy of aminophylline, terbutaline, and combined aminophylline/terbutaline as adjuncts to inhaled albuterol and found equal efficacy between all 3 groups. A cost analysis included in this study demonstrated that aminophylline without terbutaline was the most cost-effective of these adjunct therapies. A subsequent Cochrane review comparing aminophylline and terbutaline for pediatric and adult patients with status asthmaticus found insufficient evidence to support one over the other.40 Finally, a more recent retrospective review demonstrated increased length of pediatric ICU stay for children receiving aminophylline when compared with matched case controls, but there remains a high potential for selection bias in this study.41
Overall, the data supporting the use of methylxanthines as an adjunct for the treatment of status asthmaticus are weak, and methylxanthines are the only adjunct therapy discussed in this review that are specifically “not recommended” in the NIH expert guidelines.1 Despite this, intravenous methylxanthines remain a therapeutic option in many ICUs. The ability to closely monitor theophylline levels in the ICU may help to mitigate some of the potential adverse effects of methylxanthines, but these adverse effects, particularly tachycardia and nausea, will often limit their use. Enoximone is a selective phosphodiesterase III inhibitor that was demonstrated to have bronchodilatory effects in adults with asthma, with the potential for fewer adverse effects than the nonselective methylxanthines.42 However, the clinical utility of this new drug in children remains unknown.
Magnesium
Magnesium causes smooth-muscle relaxation by altering the flow of calcium into the muscle sarcoplasmic reticulum and therefore reducing the muscle's ability to contract.6 Because of this property, magnesium is also commonly used in the setting of premature labor to reduce uterine smooth-muscle contractions. By the same process, magnesium reduces bronchoconstriction in the airways. The presence of magnesium also inhibits mast cell degranulation,43 which may block histamine release and mitigate further inflammation. Adverse effects are typically mild and may include generalized weakness, malaise, and hypotension (although the latter has not been reported in studies where magnesium is given as treatment for asthma).
Ciarallo et al44 demonstrated that an intravenous bolus of 25 mg/kg magnesium sulfate over 20 min versus placebo in children presenting to the emergency department with moderate to severe asthma flares results in significant improvement in FEV1 at 50 min, lasting until at least 110 min. Subsequent randomized trials with increased dosage (40–75 mg/kg) demonstrated similar improvements in peak expiratory flow and were also associated with lower rates of hospital admission, further supported by a small (115 subjects) meta-analysis.45–48 For children subsequently admitted to the ICU, children who received intravenous magnesium on presentation to the emergency room may have a milder course, including lower likelihood of requiring mechanical ventilation.49 Singhi et al50 also demonstrated that magnesium is more effective than either terbutaline or aminophylline as an adjunct therapy to inhaled β agonists, as measured by reductions in clinical asthma scores. Continuous intravenous infusion of magnesium (rather than a single bolus) has been demonstrated to be tolerated without complications, but clinical efficacy for infusions > 4 h has not been evaluated.51–54
More recently, interest has grown in the use of inhaled nebulized magnesium in the setting of status asthmaticus. Demonstrating proof of concept, Mahajan et al55 demonstrated a 25% increase in FEV1 measured at 10 and 20 min following a dose of nebulized magnesium coupled with albuterol compared with albuterol alone in children presenting to the emergency department with mild and moderate asthma. Subsequently, a 2005 Cochrane review combining pediatric and adult subjects demonstrated a similar improvement in lung function when nebulized magnesium was combined with albuterol, but only in subjects with more severe asthma.56 The same study found a nonsignificant reduction in hospital admissions. However, when this same Cochrane analysis was repeated in 2012, the authors concluded that evidence was inadequate to support the routine use of inhaled magnesium with inhaled β agonists.57 Of note, inhaled magnesium alone appeared to be inferior to inhaled β agonists in terms of lung function improvement. The Magnesium Trial in Children (MAGNETIC trial) was published after the 2012 Cochrane review and randomized 500 children to receive 3 doses of either a combination of nebulized albuterol, ipratropium, and magnesium or albuterol and ipratropium without magnesium.57 Similar to prior studies, there was a small improvement in asthma severity scores in the magnesium group compared with the control group, with a trend toward greater benefit in the sicker subjects. However, the noted improvement was probably of little clinical importance, with no differences in any secondary outcomes, including hospital stay or ICU admission. Finally, a large randomized trial in adults demonstrated that whereas neither was particularly effective for acute asthma exacerbations, inhaled magnesium was probably inferior to intravenous magnesium.58
In summary, intravenous magnesium is an inexpensive and low-risk adjunct therapy that probably provides some benefit in children with status asthmaticus, particularly when given early in presentation to the hospital. Although nebulized magnesium appears to be safe and may provide marginal benefit in lung function, it remains unclear whether inhaled magnesium provides any clinical advantage over intravenous administration.
Antibiotics
Asthma exacerbations are commonly precipitated by environmental triggers or viral infections, less commonly by atypical bacterial infections, and rarely by other bacterial infections, yet antibiotics are frequently prescribed during severe asthma exacerbations in children.59 When compared with adults, children have several physiologic characteristics placing them at increased risk of atelectasis, including smaller airways, fewer anatomical pathways of collateral ventilation, and increased chest wall compliance. As such, chest radiography at presentation of a pediatric asthma exacerbation will commonly demonstrate areas of atelectasis that may easily be mistaken for infiltrates. However, because asthma is primarily a problem of small airways, the alveoli are generally spared and concomitant focal bacterial pneumonia is rare. A 2001 Cochrane review of randomized control trials demonstrated no clinical benefit to the addition of antibiotics during acute asthma exacerbations in children or adults.60
More recently, macrolides have been proposed as an adjunct therapy for asthma due to their activity against atypical bacteria as well as their intrinsic anti-inflammatory effects.61 Studies of macrolides in asthma are primarily in adults, lowquality, and focused on the chronic management of asthma rather than treatment during exacerbations. A 2015 Cochrane review found that although chronic macrolide use may have some benefit on lung function, macrolides were no better than placebo at preventing hospital admissions or improving quality-of-life measures.62 There are no data supporting macrolide use in status asthmaticus.
The available evidence does not support routine antibiotic use in status asthmaticus. Use of antibiotics should be limited to children with suspected bacterial infection, either through definitive focal pneumonia on chest radiograph or a history consistent with or exposure to atypical bacterial infection.
Ketamine
Ketamine is a dissociative anesthetic most commonly used for its sedative and analgesic properties. Through its mechanism of action as a noncompetitive N-methyl-D-aspartate receptor antagonist in the cortex and limbic system, ketamine causes a dissociative cataleptic-like state and analgesia.17 In the peripheral nervous system, stimulation of the N-methyl-D-aspartate receptor causes release of norepinephrine and other catecholamines.63 The most common adverse effects of ketamine are a result of this catecholamine release: tachycardia, hypertension, and bronchodilation. This latter effect has led to ketamine use as an adjunct therapy in status asthmaticus. Other notable adverse effects include nausea and increased secretions in the form of sialorrhea and bronchorrhea.17 A rare but potentially life-threatening complication is laryngospasm.
Ketamine was first reported as a therapy for small-airways disease in 1971, when practitioners noted a sudden resolution of wheezing following ketamine administration in a young child with respiratory distress.64 Multiple case reports and case series describe successful use of ketamine in children and adults with status asthmaticus, with no serious adverse effects noted.65–69 For mechanically ventilated patients, ketamine administration was associated with increases in dynamic compliance and PaO2/FIO2 and concomitant decreases in peak inspiratory pressure and PaCO2.67,70
A prospective observational study of ketamine (loading dose 1 mg/kg followed by infusion of 0.75 mg/kg/h) for children presenting to the emergency department with status asthmaticus demonstrated decreases in breathing frequency and clinical asthma score along with improvements in oxygen saturations following ketamine administration.71 Some of these children experienced mild hallucinations, which resolved with benzodiazepine administration. Comparatively, a randomized trial of ketamine (loading dose 0.2 mg/kg followed by infusion of 0.5 mg/kg/h) versus placebo for children presenting to the emergency department with status asthmaticus failed to demonstrate a difference in clinical asthma scores.71
If a child with asthma progresses to respiratory failure, the intubation process itself may be extremely hazardous. Whereas negative intrathoracic pressure (present during spontaneous ventilation) helps augment venous return to the right atrium, the transition to positive-pressure ventilation may compress the right atrium, decreasing preload to the heart and lowering cardiac output, and may lead to cardiac arrest. Ketamine may be of particular use for asthma patients with respiratory failure, coupling bronchodilation with the sedation and analgesia that may be needed for an intubated patient. In contrast to other sedatives that might be used for intubation, ketamine may help maintain preload to the heart through peripheral vasoconstriction from catecholamine release. Potential downsides of ketamine use in the mechanically ventilated patient include increased volume of secretions and risk for delirium with prolonged ketamine use.
The small studies mentioned here suggest that ketamine probably has some benefit in bronchodilation and clinical symptoms when delivered at a dose at or approaching 1 mg/kg. However, no studies provide evidence regarding ketamine compared with other adjunct therapies for asthma or ketamine's effect on long-term clinical outcomes; nor are there any randomized control trials supporting ketamine use with a higher dosing range.
Heliox
Audible wheezing in asthmatics is caused by turbulent flow in the smaller airways, which represents a high-resistance state. During turbulent flow, lower density gases have less resistance to flow. Laminar flow is a lower-resistance state where the air flow is more organized, and resistance to flow is primarily a function of airway diameter. The transition from laminar to turbulent flow is determined by the Reynolds number and is a function of airway diameter, viscosity, and density.72 Gases with lower density are more likely to exhibit laminar flow, as are gases flowing through a larger-diameter airway or with higher viscosity.72,73
Heliox (helium-oxygen mixture) is a low-cost gas mixture where nitrogen, approximately 79% of molecules in atmospheric air, is replaced with helium. Since helium is 7 times lighter than N2, the resultant gas is less dense (with a nominal viscosity change) and therefore improves flow during turbulent states and is more likely to result in low-resistance laminar flow through small airways. The effect of heliox therapy should be fairly instantaneous, because nitrogen should be washed out of the airways within a few breaths. Once laminar flow is achieved (ie, wheezing has subsided), maximal benefit has been achieved. Because O2 is similar in weight to nitrogen, the benefit of heliox decreases as FIO2 increases, and a smaller proportion of helium remains (Fig. 2). It is unclear at what FIO2 the clinical benefit of heliox is negated, but many providers question utility once the helium fraction falls below 0.5. Heliox poses few risks, but delivery must be monitored carefully, because the flow meters on some devices cannot be calibrated for the different gas density and therefore delivered flow may be unreliable. Also, prolonged use of heliox may prevent turbulent flow during coughing and therefore hinder airway clearance. Finally, helium gas is a finite resource and therefore should be used judiciously.

Relative density of nitrogen-oxygen gas mixture compared with helium-oxygen gas mixture.
A 1996 randomized trial of heliox (70% helium/30% O2) in pediatric asthma subjects admitted to the hospital demonstrated a small but significant improvement in peak expiratory flow, but no difference was noted in clinical outcomes, including dyspnea scores.74 Another randomized trial published 1 y later demonstrated that heliox (80% helium/20% O2) improved dyspnea scores and led to a reduction in pulsus paradoxus, which was reversible on discontinuation from heliox.75 No such changes were noted in the control group, and furthermore, these authors reported that the clinical improvements witnessed with the addition of heliox resulted in 3 subjects avoiding intubation. In a separate study of intubated asthmatics, the addition of heliox to the ventilator circuit led to significant decreases in both peak inspiratory pressures and PaCO2.76 However, a 2003 Cochrane review of 6 studies (1 pediatric, 5 adult or mixed ages) detailing heliox use in the emergency department for asthma found no significant differences in pulmonary function for those subjects receiving heliox.77 A 2010 randomized trial (heliox vs air) of 42 children admitted to the pediatric ICU also demonstrated no difference in time to improvement of clinical asthma scores or time to ICU or hospital discharge.78
Another theorized benefit of heliox surrounds the delivery of inhaled therapies, with the proposition that heliox may improve transport of these medicines into the small airways.79 Kim et al80 randomized subjects to receive continuous albuterol delivered by either 100% oxygen or heliox and witnessed improved pulmonary index scores and higher likelihood to be discharged from the hospital within 12 h in the heliox group. These results were not reproducible in a 2006 randomized trial using dyspnea index scores and admission rates as outcomes,81 but a 2010 cohort study witnessed shorter duration of emergency department stay for those subjects receiving heliox-driven (rather than oxygen-driven) nebulized salbutamol.82 Finally, a 2014 systematic review of heliox-driven nebulized β-agonist therapy in pediatric and adult subjects reported increased peak expiratory flows and reduced hospital admissions for heliox compared with control groups, with a trend toward greater benefit in more severely affected subjects.83
It should be noted that application of heliox was not consistent across these studies, with varying FIO2 of the heliox mixture and the control gas and a variety of clinical scoring tools used to evaluate the effectiveness of heliox treatment. Given the conflicting results and heterogeneity of study design, it is difficult to draw any firm conclusions regarding the use of heliox, particularly outside of the emergency department setting. Given the low cost and negligible adverse effect profile, it is reasonable to initiate heliox for status asthmaticus patients in respiratory distress refractory to more standard therapies, but the gas should be discontinued if no improvement in clinical status is witnessed after a short therapeutic trial.
Noninvasive Respiratory Support
Noninvasive respiratory support, including noninvasive ventilation (NIV) and high-flow nasal cannula (HFNC), is increasingly used in many forms of respiratory failure, including severe acute asthma. Positive pressure reduces work of breathing by assisting respiratory muscles, improves oxygenation by raising mean airway pressure, and, in obstructive lung disease, may assist gas exchange by mechanically stenting open the airways.84 Although the potential of avoiding invasive ventilation is a real benefit of this approach, pediatric noninvasive ventilation is often challenging due to the need for a variety of properly sized interfaces and some children's intolerance of the device.
Use of NIV in both children and adults with status asthmaticus has been associated with decreases in PaCO2 and breathing frequency and concomitant increases in pH and PaO2.85–91 Improvements in these parameters are typically noted within the first 1–2 h of therapy and are sustained, with potential continued improvement, for the duration of the therapy (ranging from approximately 2 to 48 h in these studies). NIV is typically reserved for patients not responding to initial asthma therapies, and a minority of these patients advance to requiring intubation and invasive mechanical ventilation. Some may require anxiolytics or mild sedation to tolerate the device. Rare complications may include air-leak syndromes, including pneumothorax, pneumomediastinum, or subcutaneous emphysema.90
Beers et al89 reported their experience using NIV in 83 children in the emergency department with status asthmaticus refractory to other therapies. Whereas 12% of subjects did not tolerate the device, 22% of the subjects treated with NIV demonstrated enough clinical improvement to change their planned ICU disposition to the general wards. A small randomized control trial of NIV versus traditional therapy for children with status asthmatics in 2012 noted significant improvements in breathing frequency and oxygenation requirement in the NIV group.92
HFNC is typically defined as heated, humidified gas flow delivered by nasal cannula at a flow exceeding that patient's inspiratory demand.93 In addition to providing a variable low level of positive pressure, another proposed benefit of HFNC is continuous washout of anatomic dead space. In animal models, increasing flow via HFNC has been demonstrated to assist with CO2 clearance independent of tracheal pressure.94 It is unclear at what flow anatomic washout is complete and maximal benefit is achieved. Although HFNC does not deliver the same consistent positive pressure support of NIV, it is often much better tolerated by patients with a more comfortable interface (nasal cannula vs face mask).
Although few data exist regarding the use of HFNC in children with status asthmaticus, HFNC has been shown to reduce work of breathing in adults with COPD, an obstructive disease that shares some physiologic characteristics with asthma.95 Several retrospective reviews of HFNC use in children include asthma subjects in their case series, demonstrating the commonality of its use in status asthmaticus and suggesting an acceptable safety profile.96,97 Data evaluating its effectiveness in this population are lacking.
In-depth discussion of varying methods of delivery of nebulized aerosols during noninvasive respiratory support is a topic beyond the scope of this review, but this is an area that requires further investigation. For NIV, technical aspects affecting aerosol delivery may include interface design and seal, nebulizer type, and location of the nebulizer within the circuit.98–100 Some studies suggest improved delivery of aerosol medication when coupled with NIV; however, it is difficult to differentiate the benefits of positive pressure from any change in aerosol delivery. HFNC may also impact delivery of inhaled therapies. In an in vitro model, Perry et al101 found decreased delivery of nebulized albuterol with increased flow through a variety of HFNC devices, which was supported in a separate in vitro study by Reminiac.102 However, no clinical studies exist detailing the effects of HFNC aerosol delivery on patient outcomes.
The current data suggest that NIV is safe for children with status asthmaticus and improves symptoms of respiratory distress. No data exist regarding long-term outcomes, including need for invasive mechanical ventilation or ICU or hospital stay. Furthermore, the effect of noninvasive respiratory support on inhaled therapies remains unclear, and there are no studies comparing the effectiveness of noninvasive respiratory support with the other adjunct therapies mentioned in this review. One consistent message in literature describing the use of noninvasive respiratory support centers on the timing of effectiveness. The vast majority of patients will demonstrate improvement in 1–2 h,93,103 and in the absence of this improvement, care should be escalated rather than continuing with noninvasive respiratory support without other interventions. Similarly, a patient who initially demonstrates improvement while receiving noninvasive respiratory support may later worsen, so these are patients who must be monitored closely for signs of impending failure, including increased work of breathing, decreasing mental status, or inability to maintain FIO2 < 0.6. Given these caveats, a closely monitored trial of HFNC and/or NIV is reasonable in most refractory status asthmaticus patients.
Inhaled Anesthetics
If a status asthmaticus patient progresses to respiratory failure, inhaled anesthetic gases may provide another option to enhance bronchodilation. Inhaled anesthetics, such as isofluorane, halothane, and sevoflurane, are powerful smooth-muscle relaxants and can help relieve bronchoconstriction.104 Isoflurane and sevoflurane are most commonly reported, with concerns that halothane may cause severe hepatotoxicity, particularly with prolonged use. Through their systemic effects, the primary adverse effects of inhaled anesthetics are decreased systemic vascular resistance and hypotension. Malignant hyperthermia is a rare and potentially fatal complication of inhaled anesthetics.
Multiple case reports present successful application of inhaled anesthetics to children and young adults with refractory status asthmaticus,105–112 but no clinical trials exist comparing this therapy with other adjunct therapies. Retrospective reviews demonstrate that the initiation of these gases is consistently associated with a decrease in PaCO2 around 20 mm Hg and concomitant rise in pH of about 0.1 within a few hours of administration.105,108,111,113–115 The largest case series to date includes 31 children over a 15-y period, in which children received isoflurane for a mean duration of 55 h (range 1–181 h) and were invasively ventilated for a mean of 252 h (range 16–1,444 h). The majority (77%) of these children developed hypotension requiring vasopressor support, but all survived without long-term sequelae. Char et al104 used the Pediatric Health Information Systems administrative database to compare those centers using inhaled anesthetics for >10% of mechanically ventilated asthma subjects with those rarely using inhaled anesthetics and found no differences in mortality but did note that the use of inhaled anesthetics was associated with greater length of ventilation, length of hospital stay, and costs.
Due to the high cost of this therapy and the potential for adverse effects, inhaled anesthetics are typically saved as a rescue therapy in those status asthmaticus patients failing other adjunct therapies. Providing inhaled anesthetics outside of the operating room requires specialized equipment to prevent release of the active gas into the environment and exposing care providers.116 As such, many ICUs will be limited in their ability to provide this therapy or must rely on equipment and staff borrowed from the operating room.
Extracorporeal Membrane Oxygenation
Invasive mechanical ventilation may be challenging in an asthma patient, because the placement of an artificial airway does not bypass the affected smaller airways and may, in fact, trigger further bronchospasm. Gas trapping is common, leading to worsening hypercarbia, lung hyperinflation, and increased risk of ventilator-induced lung injury. Ventilation strategies for asthma patients are controversial and beyond the scope of this article, but focus should be placed on optimizing expiratory time to allow full exhalation. When providers are unable to meet clinical goals using the ventilator, extracorporeal membrane oxygenation (ECMO) is a mode of technological support that may be used to provide or supplement gas exchange.
Essentially acting as a third lung, ECMO uses large catheters to draw deoxygenated venous blood from the patient and pass that blood through an artificial membrane gas exchanger, which adds oxygen and removes carbon dioxide from the blood. The oxygenated blood is then returned to the patient into either the venous or arterial system. Because of the risks of ECMO, including bleeding and neurological insult, ECMO is typically reserved as a rescue therapy for refractory respiratory failure.117,118
Like mechanical ventilation, ECMO provides lung and/or heart support while a patient recovers from a specific disease process or insult. Also like mechanical ventilation, ECMO does nothing to cure or reverse the underlying disease process, although ECMO typically allows providers to reduce ventilator settings and “rest” the lungs. Because refractory status asthmaticus is a short-term, self-limited disease, it is conceptually an ideal disease for ECMO support. If a patient can be adequately oxygenated and ventilated during the acute asthma flare without causing significant lung injury, the likelihood for long-term lung recovery is excellent.
Multiple case reports describe successful use of ECMO for refractory status asthmaticus119–122; however, there is limited systematic evidence evaluating the efficacy of this therapy. The largest data set describing the outcomes of ECMO for asthma is the Extracorporeal Life Support Organization registry, which captures voluntarily reported data from > 100 international ECMO centers.123 Although the mortality for asthma patients requiring ECMO support is notable, at 17% for the 72 children with status asthmaticus reported to the Extracorporeal Life Support Organization registry, it is important to note that this population has typically failed other therapies for status asthmaticus and therefore has a very high expected mortality. In fact, among children placed on ECMO for respiratory failure, a diagnosis of status asthmaticus is an independent predictor of survival, with 83% survival compared with 56% survival for all pediatric respiratory ECMO patients.124
Because asthma is primarily a disease of ventilation not involving the alveoli, hypercarbia is typically more of a challenge than oxygenation. For this reason, as well as overall safety profile, venovenous ECMO is generally the preferred approach for patients with asthma requiring ECMO.117 The high aqueous solubility of carbon dioxide allows the artificial membrane to be highly efficient at carbon dioxide removal, and adequate ventilation may be achieved at lower blood flows than might be utilized in venoarterial ECMO. Extracorporeal carbon dioxide removal, sometimes referred to as “respiratory dialysis,” is a system similar to venovenous ECMO but using smaller venous cannula and lower flows and has also been reported in select case reports as a successful mode of therapy for status asthmaticus.125,126 A third option of extracorporeal support to consider for asthma patients is pumpless extracorporeal lung assist, in which the patient's own arterial pressure is used to drive blood through the gas-exchange membrane, returning oxygenated and ventilated blood to the patient's venous system. Potential advantages to this strategy include the lack of a mechanical pump and the reduced need for anticoagulation. Although a handful of case reports exist demonstrating successful application of this technique for adults with asthma,127–129 data in children are lacking.
Finally, ECMO may also be beneficial for those patients with asthma who experience complications of mechanical ventilation with additional lung injury, including air-leak syndromes. Air-leak syndromes are rare as a primary cause of ECMO use outside of the neonatal period, but case reports demonstrate successful use of ECMO for air-leak syndromes that could imply similar success for patients with ventilator-induced lung injury in the setting of status asthmaticus.130–133
Similar to inhaled anesthetics, extracorporeal lung support is a costly and resource-intensive therapy that is only clinically indicated for asthma patients failing other therapies. Unfortunately, some of these patients may be failing due to complications from mechanical ventilation that may be secondary to suboptimal management. However, in these patients and for select other asthma patients, the evidence is favorable that ECMO may be a life-saving therapy with minimal long-term morbidity.
Discussion
Despite the high prevalence of status asthmaticus as an indication for emergency room visits, hospital admissions, and ICU admissions, there remains a frustrating lack of clear guidance on appropriate therapies for escalation of care when patients are refractory to the initial therapies of inhaled albuterol, systemic corticosteroids, and ipratropium. The NIH guidelines1 recommend consideration of adjunct therapies for patients who display an incomplete or poor response to initial therapy with albuterol, corticosteroids, and ipratropium but give no further guidance on the pathway for escalation.
Table 1 summarizes the mechanism of action, potential risks and benefits, and evidence class for each of the adjunct therapies discussed above. Although a good number of randomized studies exist regarding the use of these therapies for status asthmaticus, significant heterogeneity in these studies limits our ability to make definitive conclusions regarding the effectiveness and utility of most adjunct therapies. Several studies suggest a greater benefit of these therapies in sicker patients, but the absolute numbers of these more severe asthma patients in any given study are typically too small to make definitive conclusions.
Adjunct Therapies for Status Asthmaticus
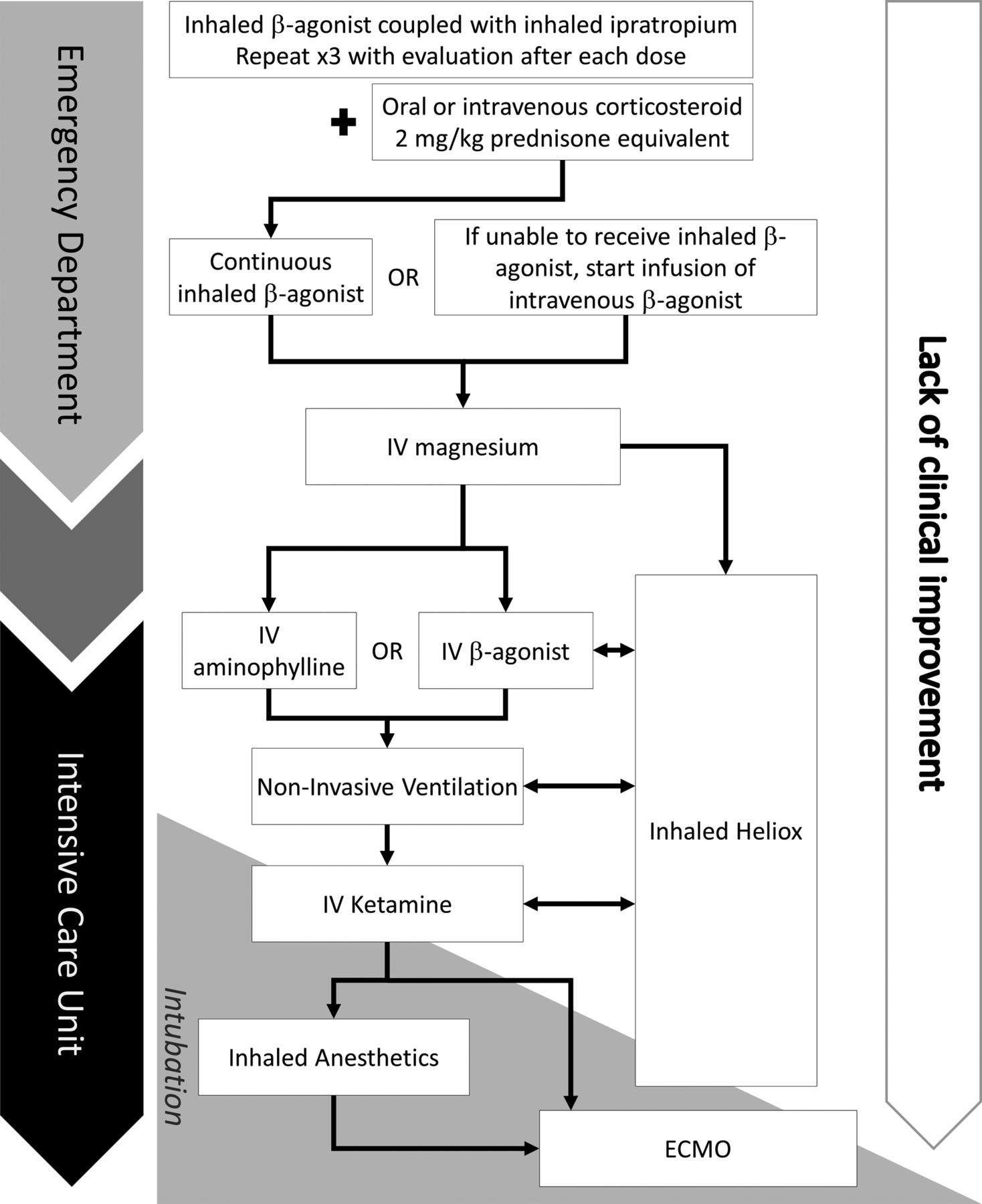
Given the potential risks inherent in invasively ventilating asthma patients, efforts should be made to avoid intubation whenever possible. Overall, 12% of patients intubated for status asthmaticus had complications during that hospitalization, and 4% died.4 Despite the paucity of data for the adjunct therapies listed in this paper, most are low risk, and it is reasonable to consider use of most these therapies for asthma patients in impending respiratory failure. Figure 3 presents a suggested care map for advancing adjunct asthma therapies, given their potential for benefit and associated risks. Similar care maps have been published by Wong et al6 and Nievas et al.135 However, it must be noted that it is unlikely that these therapies will consistently offer significant benefits in terms of ICU or hospital stay.

Care pathway for advancement of asthma therapies. ECMO = extracorporeal membrane oxygenation.
Given the remaining equipoise for many of these adjunct therapies, even in the setting of careful literature review, clinical focus should first be shifted to standardizing the approach to management of status asthmaticus. Significant heterogeneity exists in the utilization of the adjunct therapies for asthma.136 Even when a best practice is clearly defined and evidence-based, such as early delivery of inhaled β agonists and corticosteroids, achieving optimal delivery of these therapies is often inconsistent. In a retrospective review of children intubated for status asthmaticus at 8 children's hospitals, Newth et al4 noted that before intubation, only 69% of children received corticosteroids, 75% received intermittent inhaled albuterol, 45% received continuous albuterol, and 36% received ipratropium. For > 13,500 children admitted for critical asthma captured by the Pediatric Health Information Systems database, only 87% of subjects received inhaled albuterol and 86% received steroids during their hospitalization.137 In this same database, the use of adjunct therapies was widely variable: ipratropium (69%), magnesium (42%), terbutaline (22%), methylxanthines (6%), and heliox (9%). Whereas 13% received invasive ventilation, only 5% received noninvasive ventilation.
Standardizing asthma therapies may have unique benefits for each portion of a hospital visit. Ensuring consistent, early delivery of inhaled albuterol, systemic steroids, and inhaled ipratropium followed by intravenous magnesium in non-responders probably has the greatest potential to halt the progression of the asthma flare and potentially prevent hospital admissions. Furthermore, if patients require admission to the hospital, early administration of magnesium may ameliorate that patient's trajectory and prevent intubation in some of the most severe cases. Standardizing escalation of therapy after ICU admission will allow us to better understand which of these adjunct therapies may provide the most benefit and help to delineate optimal treatment strategies. Once the patient is in the recovery phase of his or her illness, standardizing the weaning process may produce more consistent reduction of therapies, with potential improvements in ICU and hospital stay. Several clinical asthma scores exist that can provide an objective indicator for both escalation and weaning of therapies.138–141 Adjunct therapies are commonly weaned in the reverse order in which they were added, such that the latest addition is the first to be weaned. However, the respective benefit and toxicity of each therapy in that patient should be considered, with therapies providing low benefit or high toxicity taking priority for weaning.
Finally, efforts to optimize out-patient asthma care before hospital presentation have the potential to make a profound impact on asthma morbidity and mortality as well as overall health-care costs related to asthma. Whereas some of these efforts may focus on optimization of medication strategies, the importance of asthma education cannot be overstated.142–144 Asthma education with patient engagement is the best strategy to ensure consistent delivery of those medications that may prevent asthma exacerbations as well as to assist with early identification and treatment of asthma exacerbations.145
Summary
Early intervention with inhaled β agonists and ipratropium and systemic steroids for children presenting to the emergency department with moderate to severe asthma exacerbation has the best potential to halt the progression of status asthmaticus. A bolus dose of intravenous magnesium should be administered within the hour if clinical improvement is not noted after these initial treatments. There remain insufficient data to guide use of specific adjunct therapies if symptoms persist or hospital admission is required; however, a variety of therapies may be considered and may provide marginal benefit in the sickest patients.
Discussion
Berlinski:
Thank you for your presentation. First of all, I would like to strongly agree with your recommendation of using protocol-based, score-based decision making pathways for management to go from the emergency department to the pediatric ICU and then to the pediatric wards to prepare for discharge. The importance of working collaboratively cannot be underscored enough. But it is a real challenge in many institutions, where 3 or 4 groups have to agree on what they are going to be doing. The second thing is: Do you have any data on the use of repeated courses of intravenous magnesium? I see it being used often after it was tried in the emergency department and just wanted to know your thoughts.
Rehder:
I definitely agree with the need for protocolization. It has been shown again and again in multiple settings, not just for asthma, that protocols improve care in many ways. For magnesium, unfortunately there are not supporting data for repeated doses. It certainly is tried, and that gets into use of infusions for the theoretical benefit of keeping the magnesium at a high level. But really the only data on magnesium infusions demonstrate it is well tolerated, but there are no solid outcome data.
Sweet:
Thanks, that was a great overview. When it comes to protocolization, I wonder whether the efforts to do quality-based reimbursement could help drive that process? And whether people are talking about really nailing down some of the things you put on your slide as part of the process measures for asthma, which makes up a significant component of acute care in most of our pediatric hospitals.
Rehder:
We need more studies like Derek Wheeler's,1 where they compared the cost-effectiveness of 2 different medicines. If 2 therapies have similar effectiveness, then whichever therapy is less costly should be an important aspect of protocols. Hopefully, we can get our own [Duke Children's] experience with an asthma protocol published and start the conversation about not only cost reduction through protocolization, but also hopefully better care and outcomes.
Panitch:
Thanks for a great talk, Kyle. In your pathway, the scheme went ultimately to ECMO, with no intermediate steps of intubation or mechanical ventilation in the pathway?
Rehder:
While I didn't specifically talk about intubation in the presentation, we talked about inhaled anesthetics, and obviously that would not be possible without mechanical ventilation. In fact, the version of the care map that will be included in the paper has intubation listed in the setting of using inhaled anesthetics or ECMO. Mechanical ventilation of an asthma patient is a large topic in itself, and can be quite challenging with lots of potential for gas trapping and barotrauma. However, the thought of initiating ECMO prior to intubation for an asthma patient has not been reported to my knowledge, but is certainly an interesting idea. In the paper, I reference extracorporeal carbon dioxide removal and some of those other less invasive ECMO support systems. Since these patients often primarily need CO2 removal, you could mimic the respiratory dialysis model that is being used in some European sites. This method entails placing a dialysis-sized catheter as opposed to a larger ECMO cannula and running much lower flows. With this model, you might be able to lower the CO2 levels enough to potentially prevent intubation and the associated morbidities. I think it's a very interesting concept, but there are no real data.
Stokes:
We had a $3 million CMS innovation award that helped us develop a high-risk asthma program, and I think a key component of that was giving kids who had repeated trips to the emergency department a different system so that they could call after hours. They were actually given steroids as part of the grant to start before they went to the emergency room, and we were able to cut down on a lot of admissions, emergency department visits, and reduce costs by having a system prior to arrival in the emergency department. One of the things that we do as part of the clinic evaluation of high risk are PFTs [pulmonary function tests]. We see a lot of different patterns when we do PFTs of high-risk asthma patients, some of whom are walking around with pretty significant pulmonary abnormalities, and others are completely normal in between exacerbations. I've never seen a link between pre-emergency department visit pulmonary function and modifying our therapy approach in the emergency department. We sort of take one approach to asthma when they end up in the emergency department, but asthma is not all the same, and having those patterns available to the emergency department physician might change the therapeutic approach.
Rehder:
I think that's another interesting concept; to be honest, I am not as familiar with the out-patient literature because that's not where I practice, but in reviewing this, I didn't see anything published on pre-emergency department evaluation being used to guide therapy. The balance between personalized care and standardized care is always a challenge. If you could target children with different genetic polymorphisms that change their response to medicines, I think that's something to really look at going forward. Is there a certain population who—because of their polymorphisms or ethnic background—might they really respond well to methylxanthines, but you have another group who is non-responsive? Can we use PFTs to evaluate or identify those patients before they show up in the emergency department? I think these are really great concepts that need to be studied.
Stokes:
It's an interesting idea. We look at bronchodilator reversibility in that population, but it would be interesting to look at methylxanthine or even look at reversibility with other agents.
Rehder:
Most of the data I have seen are looking specifically at genetic polymorphisms. They're often looking at “acute asphyxial-asthma” or “near-fatal asthma,” described as those patients who go from being clinically well to needing intubation very rapidly, as opposed to those who have a more gradual onset of their asthma flare-ups. Certainly I think there is growing interest in the area of different asthma phenotypes.
Stokes:
One aspect of the classic asthma triad, the classic Netter diagram of acute asthma, that you didn't address, is mucus obstruction. Do you know of any literature that addresses potential therapies directed against mucus obstruction?
Rehder:
I don't know of any literature that really addresses it. The only real medicine of these adjunct therapies that primarily addresses something other than bronchospasm is ipratroprium, which should decrease mucus production. Most of the others are focused on bronchoconstriction or bronchospasm.
Fedor:
I would also include patient education in your adjunct therapy, because there is a lot of evidence that addresses the issue of readmissions related to asthma for poor adherence and poor understanding of the disease process.
Rehder:
I think that's a great idea; people may not view education as an adjunct therapy, but it really could be considered as such.
Berlinksi:
Can you comment on the futility of megadoses of steroids? Unfortunately, it is still widely used, especially when the patient is not doing well.
Rehder:
I'm not aware of any data that support an advantage of higher doses of steroids than the typical dose of 2 mg/kg/d of prednisone (or equivalent). I agree that it is common where people may say “a little is good, so more must be better,” but all we probably do is increase the risk for adverse effects from the steroids.
Walsh:
A lot of these patients who are refractory to our standard therapies have other issues going on like pneumonia or some viral illness. What's your stance on antibiotics and those types things on these guys who are refractory to the standard therapy?
Rehder:
My personal stance is I try to avoid antibiotics. More often than not, we recognize that it's a viral trigger as opposed to a bacterial cause. One thing I would potentially look at would be azithromycin—there is some evidence that it has anti-inflammatory properties, and it has certainly been used for this in the cystic fibrosis population. The other aspect is any bacterial infections which might be more likely to cause wheezing, and that would be atypical. That may be worth considering, but unless there is a true focal infiltrate on chest x-ray—and not the right middle lobe atelectatsis that often is mistaken for an infiltrate. Or, after you get the airways open, if there continues to be hypoxia, that's more likely explained by a true alveolar process. Other than that, I would really try to stay away from antibiotics. [Author's note: A section on antibiotics for acute asthma was subsequently added to the manuscript.]
Walsh:
It's so hard to understand, especially when we see them in the ICU; they are fatiguing and they may have atelectasis from fatigue, or it could be that they have an underlying pneumonia that triggered the whole episode. It seems difficult for us to sort out as we continue down this pathway of asthma, asthma, asthma, and doing things like isofluorane and even ECMO and not thinking about other strategies for treating pneumonia.
Rehder:
In my career I've seen 2 patients put on ECMO for asthma. As the attending, I put one on; the other I was involved later in her care, and both of them were on antibiotics for a treatment course despite the fact that we didn't have any evidence of bacterial infection. But again, you get into risk/benefit, and clearly once you're reached that severity point, you're outside the typical expected course for an asthma patient, so something is unique about that patient.
Berlinski:
The use of airway clearance therapies, such as positive expiratory pressure, in a very select group of patients who have significant bronchorrhea is helpful. I want to go back to the use of large dose of steroids; there are probably 10 or 15 y of data that show increased doses just give you more adverse effects, hypertension, increased glucose, and not any additional benefits. That goes along with the lack of additional benefit of giving intravenous steroids as opposed to using the oral route.
Footnotes
- Correspondence: Kyle J Rehder MD, Division of Pediatric Critical Care, DUMC Box 3046, Durham, NC 27710. E-mail: kyle.rehder{at}duke.edu.
Dr Rehder has disclosed no conflicts of interest.
Dr Rehder presented a version of this paper at the 55th Respiratory Care Journal Conference, “Pediatric Respiratory Care,” held June 10-11, 2016, in St Petersburg, Florida.
- Copyright © 2017 by Daedalus Enterprises
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.
- 33.
- 34.
- 35.
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.
- 47.
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.
- 53.
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.
- 67.↵
- 68.
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.
- 87.
- 88.
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.
- 107.
- 108.↵
- 109.
- 110.
- 111.↵
- 112.↵
- 113.↵
- 114.
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.
- 121.
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.↵
- 128.
- 129.↵
- 130.↵
- 131.
- 132.
- 133.↵
- 134.
- 135.↵
- 136.↵
- 137.↵
- 138.↵
- 139.
- 140.
- 141.↵
- 142.↵
- 143.
- 144.↵
- 145.↵









{kind=link}
{kind=link}
{kind=link}