

Abstract
BACKGROUND: Albuterol hydrofluoroalkane (HFA) either alone or with a valved holding chamber is used to treat bronchoconstriction. Delays between actuation and inhalation are common. Currently, the recommended interval between actuations of an albuterol HFA is 60 s. Using a shorter interval when multiple actuations are ordered will improve productivity in the hospital setting.
METHODS: We studied aerosol characteristics of albuterol HFA (Ventolin, ProAir, and Proventil) with a cascade impactor calibrated at 30 L/min. We studied pressurized metered-dose inhalers (pMDI) alone, coupled to a nonelectrostatic valved holding chamber, and coupled to the valved holding chamber but introducing a 10-s delay between actuation and measurement. We tested intervals between actuations of 60, 30, and 15 s (not for delay scenario). The variable of most interest was fine-particle mass. Albuterol was measured by spectrophotometer (276 nm).
RESULTS: Variations in fine-particle mass from 60-s values were < 15% for Ventolin and ProAir for all conditions tested and for Proventil with a valved holding chamber. Variations in fine-particle mass from 60-s values were > 15% for Proventil (pMDI alone with a 30-s interval and pMDI/valved holding chamber with delay and a 30-s interval). Adding a valved holding chamber increased fine-particle mass for all brands (ProAir 7–12%, Ventolin 26–35%, and Proventil 44–47%). The introduction of a 10-s delay reduced fine-particle mass for all brands (ProAir 34–39%, Ventolin 39–42%, and Proventil 27–32%). Comparison of fine-particle mass among brands showed that Proventil was > ProAir > Ventolin.
CONCLUSIONS: Decreasing the interval between actuations from 60 to 30 and 15 s does not seem to affect the aerosol characteristics of ProAir and Ventolin. Although some changes were noticed for Proventil, the pMDI outperformed Ventolin that had the lowest fine-particle mass. The use of a valved holding chamber increased fine-particle mass, but introducing a 10-s delay between actuation and inhalation significantly reduced fine-particle mass.
Introduction
Asthma is a highly prevalent disease affecting approximately 6 million children in the United States.1 Almost 60% of these patients experienced at least one asthma attack, and almost 137,000 patients were discharged with a diagnosis of asthma from hospitals in the United States during 2010.1 The National Asthma Education and Prevention Program Expert Panel Report 3 defines asthma as “a complex disorder characterized by variable and recurring symptoms, air-flow obstruction, bronchial hyper-responsiveness, and an underlying inflammation.”2 Inhaled bronchodilators are used for management of acute episodes of bronchoconstriction.2
Several studies have found that aerosol delivery via pressurized metered-dose inhalers (pMDI) and via pMDI with a valved holding chamber are as efficacious as nebulized albuterol for the treatment of asthma exacerbations in adults and children, respectively.3 Length of treatment of a nebulized bronchodilator is typically around 10–15 min but is actually 5–10 min longer when preparation and cleaning are taken into account. Manufacturers of albuterol in the United States recommend a 1-min interval between actuations.4–6 Therefore, if large number of actuations of albuterol pMDI are prescribed, the length of treatment might become similar to that of a nebulizer treatment. Being able to administer albuterol pMDI with a shorter interval between actuations would allow greater productivity in the hospital setting. Previously, Hautmann et al7 reported that the fine-particle mass increased from pMDI, and pMDI with a valved holding chamber increased when the interval between actuations increased from 15 to 120 s. However, they provided limited data on the characterization of the aerosols. Clark et al8 reported that a delay between actuation and inhalation resulted in a decrease in lung bioavailability of albuterol pMDI delivered with a valved holding chamber. Delays between actuation and inhalation are common during real-life administration of pMDI with a valved holding chamber. Therefore, it is clinically relevant to investigate the effect of the delay on the aerosol characteristics of albuterol pMDI. Several authors have reported differences in the aerosol characteristics of different brands; therefore, evaluating all available brands is also relevant.7,9
In this study, we compared the aerosol characteristics of 3 different brands of albuterol hydrofluoroalkane (HFA) pMDI alone, with a valved holding chamber, and with a valved holding chamber introducing a 10-s delay between actuation and inhalation. We hypothesized that (1) there would be differences in the characteristics of the aerosol generated by each brand of inhaler actuated at different time intervals, (2) the use of a valved holding chamber would eliminate those differences, and (3) the introduction of a 10-s delay between actuation and measurement could change aerosol characteristics.
QUICK LOOK
Current knowledge
Currently, the recommended interval between actuations of an albuterol hydrofluoroalkane is 60 s. Using a shorter interval when multiple actuations are ordered will improve productivity in the hospital setting.
What this paper contributes to our knowledge
Intervals between actuations of albuterol hydrofluoroalkane of 30 or 15 s produced an aerosol with similar characteristics to the one with a 60-s interval. The addition of a valved holding chamber increased the fine-particle mass. Conversely, a delay between actuation of pressurized metered-dose inhaler/valved holding chamber and testing resulted in a significant decrease in fine-particle mass.
Methods
The experiments were performed at the Pediatric Aerosol Research Laboratory at Arkansas Children's Research Institute in Little Rock, Arkansas. The study comprised 3 parts. Particle size distribution was determined for the pMDI alone (part A), pMDI with a valved holding chamber (part B), and pMDI with a valved holding chamber and a 10-s delay between actuation and measurement (part C).
The pMDI and the Valved Holding Chamber
We tested 4 new units of albuterol HFA of 3 different brands. ProAir HFA (Teva Specialty Pharmaceuticals, Horsham, Pennsylvania) and Ventolin HFA (GlaxoSmithKline, Philadelphia, Pennsylvania) have incorporated counters to monitor the remaining number of actuations. Proventil HFA (3M Health Care, Loughborough, United Kingdom) was also tested. Since the latter did not have a counter, the number of actuations was recorded in the laboratory notebook. Four new, nonelectrostatic valved holding chambers (AeroChamber Plus Flow-Vu, Monaghan Medical, Plattsburgh, New York) with mouthpiece were used for parts B and C of the study.
Study Design
Four pMDIs of each brand were tested for the scenarios. During part A, pMDIs were tested without a valved holding chamber, and 3 different timing intervals between actuations were studied (15, 30, and 60 s). During part B, pMDIs were tested with a valved holding chamber and the same time intervals between actuations used in part A. Part C was similar to part B, except that a 10-s delay between actuation and connection of the valved holding chamber to the cascade impactor was introduced. Also during part C, the only timing intervals between actuations that were tested were 30 and 60 s.
Procedure
A Next Generation Impactor (model 170 NGI, MSP Corporation, Shoreview, Minnesota) assembled with internal and external filters was used.10 At the beginning of each procedure, the temperature (median 23°C [95% CI 23–23.5°C]) and humidity (47% [95% CI 44–47%]) were documented, and the impactor was calibrated to 30 L/min using a mass flow meter (Mass Flowmeter 4043, TSI, Shoreview, Minnesota). A silicon adapter was used to connect the throat of the NGI to either the pMDI or the valved holding chamber. Each pMDI was primed with 4 actuations at the beginning of each testing day. During part A, the impactor was powered on, and the pMDI was shaken for 5 s and then connected to the adapter and actuated once, with 3 s elapsing between the last shake and the actuation. The pMDI was removed after 5 s. The procedure was repeated 9 more times for a total of 10 actuations. The canisters were weighed at the beginning and at the end of the 10 actuations for quality control. Interval periods between actuations of 15, 30, and 60 s were tested. During part B, the pMDI was placed in the posterior opening of the valved holding chamber and shaken for 5 s. The system was then connected to the impactor with 3 s elapsing between the last shake and the actuation (Fig. 1). The pMDI/valved holding chamber was removed after 5 s. The procedure was repeated 9 more times for a total of 10 actuations. The canisters were weighed at the beginning and at the end of the 10 actuations for quality control. Interval periods between actuations of 15, 30, and 60 s were tested. During part C, the pMDI connected to the valved holding chamber was shaken for 5 s and actuated once, with 3 s elapsing from the last shake and the actuation. A 10-s interval was introduced between actuation of the pMDI and connection to the impactor. The pMDI/valved holding chamber was removed after 5 s. The procedure was repeated 9 more times for a total of 10 actuations. The canisters were weighed at the beginning and at the end of the 10 actuations for quality control. Interval periods between actuations of 30–60 s were tested. The median (99% CI) pooled differences in canister weight were 1.020 g (1.009–1.024 g), 0.453 g (0.447–0.458 g), and 0.400 g (0.374–0.412 g) for Ventolin, ProAir, and Proventil, respectively.

Investigational setup used to measure particle size of albuterol hydrofluroalkane.
The impactor was disassembled at the end of 10 actuations, and the throat, cups, and filters were eluded with 10 mL of double-distilled water. Valved holding chambers were cleaned after each series of 10 runs, and they were tested for the presence of albuterol before the following test. The plastic actuator of the pMDI was also flushed with double-distilled water and dried with compressed air. All washings were tested for albuterol concentration using spectrophotometry (Biomate 3 UV-visible spectrophotometer, Thermo Fisher Scientific, Waltham, Massachusetts) at 276 nm.
Mass median aerodynamic diameter (MMAD), geometric standard deviation (GSD), and percentage of drug mass associated with particles < 5 μm and between 1 and 3 μm were calculated using CITDAS 3.1 software (Copley Scientific, Nottingham, United Kingdom). Fine-particle mass was calculated as the amount of drug captured in stages 4–7 of the impactor.7 Variation was calculated as follows: (variable at 30 or 15 s − variable at 60 s)/variable at 60 s × 100. Variations in FPM, percentage <5 μm, and percentage 1–3 μm of ≤ 15% were considered acceptable.11
Statistical Analysis
Comparisons between variables obtained with the same pMDI/valved holding chamber and pMDI/valved holding chamber with 10-s delay were done with a paired t test with unequal variance. Comparisons among variables obtained with the same pMDI brand at difference time intervals and scenarios were done with analysis of variance for repeated measures followed by a Dunnett test when necessary. Comparison of fine-particle mass among brands at each scenario was done with analysis of variance for repeated measures followed by the Tukey test when necessary. A P value of < .05 was considered statistically significant. A statistical software package was used for all of the calculations (Kaleidagraph 4.53, Synergy Software, Reading, Pennsylvania).
Results
pMDI Alone
There were no significant differences in MMAD among the 3 time intervals for Ventolin (P = .32) and Proventil (P = .26) (Table 1). However, MMAD for ProAir was larger with 30-s (P < .001) and 15-s (P < .001) intervals when compared with 60-s intervals. The differences between the smallest and largest MMAD were 0.23, 0.21, and 0.14 μm for Ventolin, ProAir, and Proventil, respectively. The differences do not appear to be clinically relevant.
Aerosol Characteristics of Pressurized Metered-Dose Inhaler Alone Actuated at Different Interval Periods*
There were no significant differences in GSD among the 3 time intervals for Proventil (P = .11). However, GSD for ProAir with 15 s was similar to the 60-s interval (P = .057), and the 30-s was larger than the 60-s interval (P = .005). In addition, GSD for Ventolin for 30 s was similar to the 60-s interval (P = .30), and the 15-s was larger than the 60-s interval (P = .02). The differences between the smallest and largest GSD were 0.18, 0.07, and 0.24 for Ventolin, ProAir, and Proventil, respectively. All aerosols were heterodisperse, and the differences do not appear to be clinically relevant.
There were no significant differences in percentage < 5 μm among the 3 time intervals for Ventolin (P = .46). However, the percentage < 5 μm for ProAir was larger at a 60-s interval than at 30 and 15 s (P = .004 and P = .01, respectively). Similar behavior was noted for Proventil (P = .01 and P = .02 for 30 and 15 s, respectively). Variations from 60-s values were < 15% for Ventolin and ProAir but > 15% for Proventil.
There were no significant differences in percentage 1–3 μm among the 3 time intervals for Ventolin (P = .12). However, for ProAir (P < .001 and P = .006) and Proventil (P = .02 and P < .001), the 60-s interval had a larger percentage 1–3 μm than 30- and 15-s intervals, respectively. Variations from 60-s values were < 15% for Ventolin and ProAir, but > 15% for Proventil at the 15-s interval.
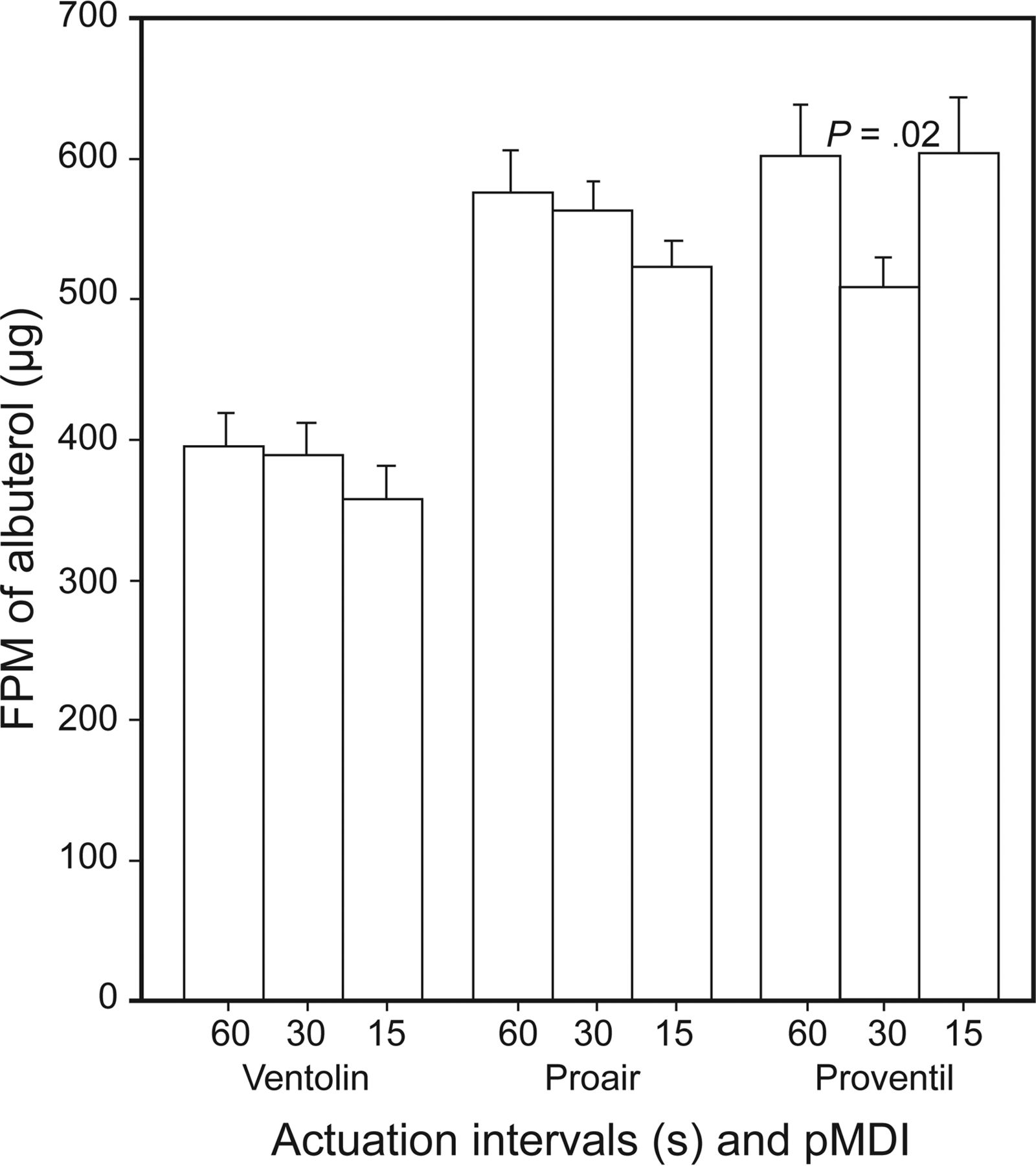
There were no significant differences in fine-particle mass among the different actuation intervals for Ventolin (P = .71) (Fig. 2). ProAir showed a decrease in fine-particle mass with a decrease in actuation intervals (P = .031 and P = .01 for 30- and 15-s intervals, respectively). Proventil showed a decrease in fine-particle mass for the 30-s, but not for the 15-s, interval (P = .02 and P = .80, respectively). Variations from 60-s values were < 15% for Ventolin, Proventil, and ProAir, except for Proventil at the 30-s interval. Comparison of fine-particle mass among brands showed that Proventil was > ProAir > Ventolin at all tested intervals (P ≤ .004).

Fine-particle mass (FPM) of albuterol hydrofluroalkane pressurized metered-dose inhaler (pMDI) alone. Bars show means, and error bars represent SD. P values are fine-particle mass difference from a 60-s interval. * Variation from 60 s is > 15%.
pMDI With Valved Holding Chamber
There were no significant differences in MMAD among the 3 time intervals for Ventolin, ProAir, and Proventil (P = .64, P = .99, P = .26, respectively) (Table 2). The differences between the smallest and largest MMAD were 0.20, 0.25, and 0.26 μm for Ventolin, ProAir, and Proventil, respectively. The differences do not appear to be clinically relevant.
Aerosol Characteristics of Pressurized Metered-Dose Inhaler Coupled to a Valved Holding Chamber Actuated at Different Interval Periods
There were no significant differences in GSD among the 3 time intervals for ProAir (P = .35) and Proventil (P = .23). The GSD for Ventolin with the 15-s interval was similar to the 60-s interval (P = .95) but larger for the 30-s interval (P = .02). The differences between the smallest and largest GSD were 0.16, 0.08, and 0.22 for Ventolin, ProAir, and Proventil, respectively. All aerosols were heterodisperse, and the differences do not appear to be clinically relevant.
There were no significant differences in percentage < 5 μm among the 3 time intervals for ProAir (P = .16) and Proventil (P = .64). However, the percentage < 5 μm for Ventolin was similar for 60- and 30-s intervals (P = .58) but was larger for the 15- than for the 60-s interval (P = .02). Variations from 60-s values were < 15% for all brands.
There were no significant differences in percentage 1–3 μm among the 3 time intervals for Ventolin (P = .09), ProAir (P = .29) and Proventil (P = .44). Variations from 60-s values were < 15% for all brands.
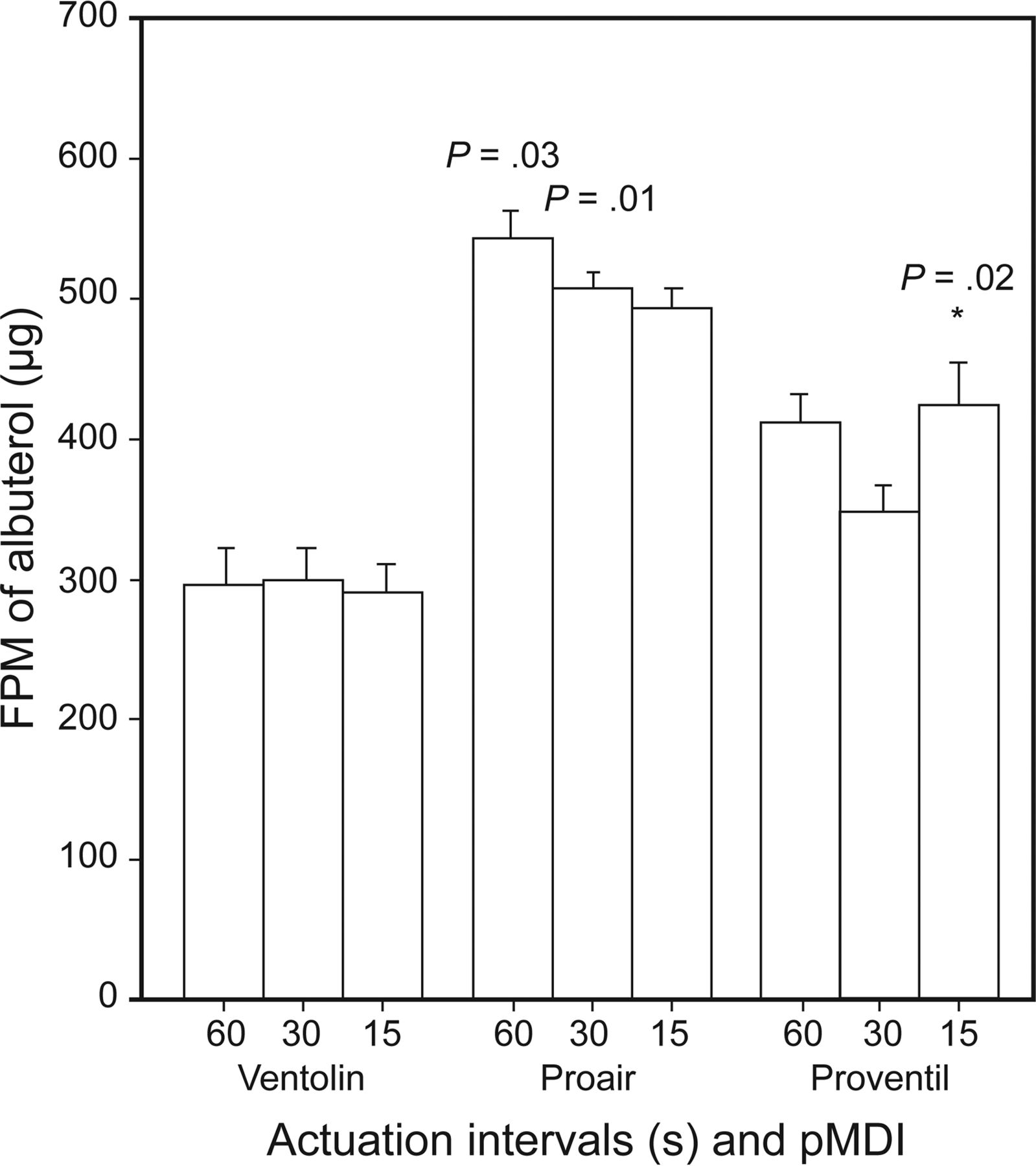
There were no significant differences in fine-particle mass among the different actuation intervals for Ventolin (P = .15) and ProAir (P = .059) (Fig. 3). Proventil showed a decrease in fine-particle mass for the 30-s, but not for the 15-s, interval (P = .02 and P = .99, respectively). Variations from 60-s values were < 15% for all brands. Comparison of fine-particle mass among brands showed that Proventil = ProAir (P = .50) > Ventolin at 60-s intervals (P < .001). The addition of the valved holding chamber resulted in a modest increase in fine-particle mass for ProAir (7–12%) and in a significant increase for Ventolin (26–35%) and Proventil (44–47%). Comparison of fine-particle mass among brands showed that Proventil was > ProAir > Ventolin at 30- and 15-s intervals (P ≤ .02).
Fine-particle mass (FPM) of albuterol hydrofluroalkane pressurized metered-dose inhaler (pMDI) coupled to a valved holding chamber. Bars show means, and error bars represent SD. P value is fine-particle mass difference from a 60-s interval.
pMDI With Valved Holding Chamber and Delay
There were no significant differences in MMAD between the 2 time intervals for Ventolin (P = .90), and ProAir (P = .07) (Table 3). However, MMAD for Proventil was larger for the 30-s interval (P = .02). The differences between the smallest and largest MMAD were 0.18, 0.20, and 0.16 μm for Ventolin, ProAir, and Proventil, respectively. The differences do not appear to be clinically relevant.
Aerosol Characteristics of Pressurized Metered-Dose Inhaler Coupled to a Valved Holding Chamber Actuated at Different Interval Periods When a 10-s Delay Between Actuation and Testing Was Introduced*
There were no significant differences in GSD among the 3 time intervals for ProAir (P = .29). Ventolin had a larger GSD with a 30-s interval than with 60 s (P = .02), and Proventil showed the opposite effect (P = .048). The differences between the smallest and largest GSD were 0.09, 0.10, and 0.19 for Ventolin, ProAir, and Proventil, respectively. All aerosols were heterodisperse, and the differences do not appear to be clinically relevant.
There were no significant differences in percentage < 5 μm among the 3 time intervals for ProAir (P = .65) and Proventil (P = .062). However, the percentage < 5 μm for Ventolin was larger for a 60-s interval than for a 30-s interval (P = .009). Variations from 60-s values were < 15% for all brands.
There were no significant differences in percentage 1–3 μm among the 3 time intervals for ProAir (P = .69) and Proventil (P = .063). The percentage 1–3 μm for Ventolin was smaller for the 30-s than for the 60-s interval (P = .01). Variations from 60-s values were < 15% for all brands.
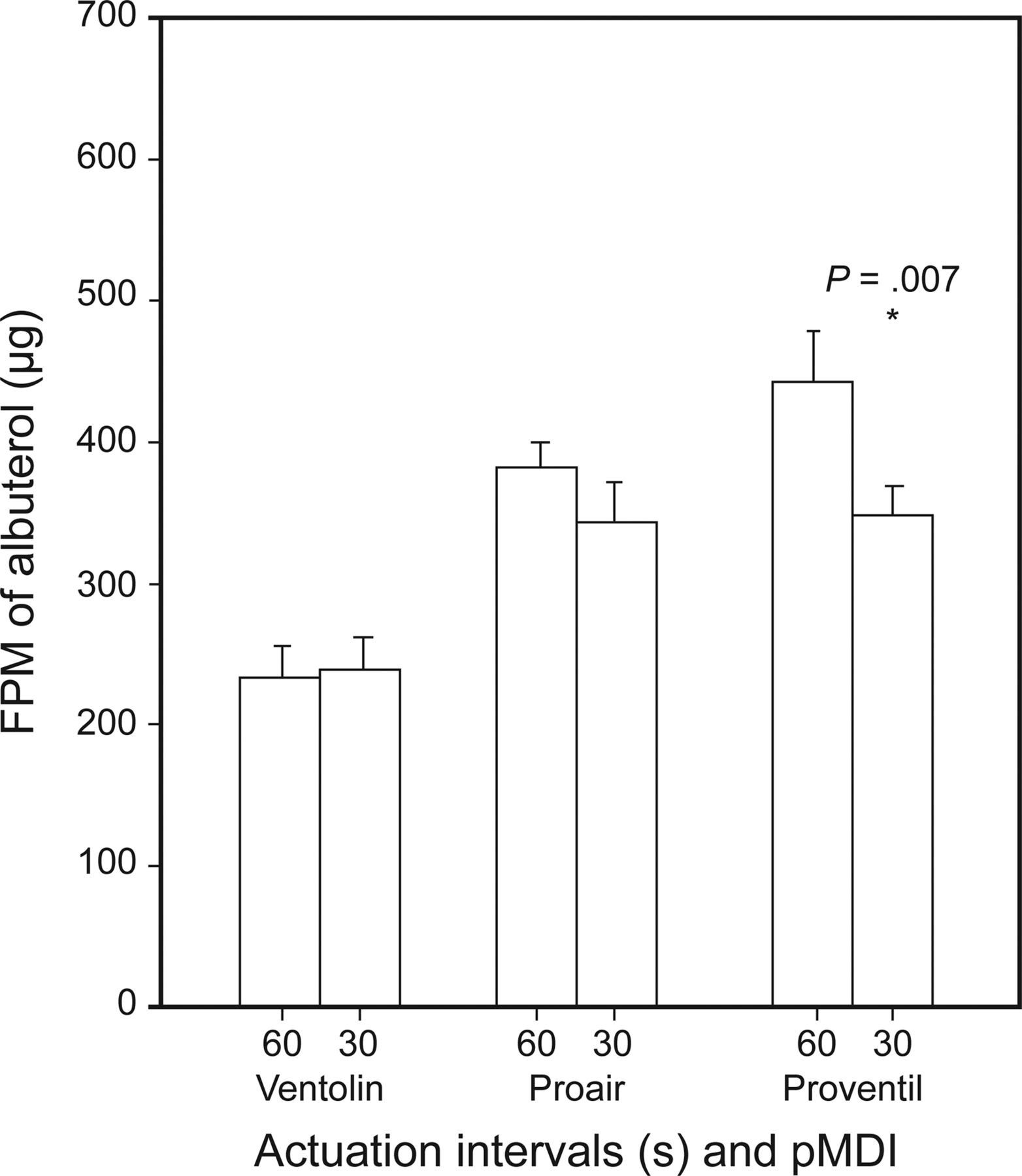
There were no significant differences in fine-particle mass among the different actuation intervals for Ventolin (P = .07) and ProAir (P = .68) (Fig. 4). Proventil showed a decrease of 21% in fine-particle mass for the 30 s (P = .007). Variations from 60-s values for Ventolin and ProAir were < 15%. Comparison of fine-particle mass among brands showed that Proventil was > ProAir > Ventolin at the 60-s interval (P ≤ .03). Comparison of fine-particle mass among brands showed that Proventil = ProAir (P = .96) > Ventolin at the 30-s interval (P < .001). The introduction of a 10-s delay resulted in a significant reduction in fine-particle mass for all brands (ProAir 34–39%, Ventolin 39–42%, and Proventil 27–32%).

Fine-particle mass (FPM) of albuterol hydrofluroalkane pressurized metered-dose inhaler (pMDI) coupled to a valved holding chamber after a 10-s delay between actuation and measurement was introduced. Bars show means, and error bars represent SD. P value is fine-particle mass difference from a 60-s interval. * Variation from 60 s is > 15%.
Discussion
We compared the aerosol characteristics of 3 brands of albuterol sulfate HFA when the intervals between actuations were 60, 30, and 15 s, and the pMDI was operated alone, coupled to a valved holding chamber, and coupled with a valved holding chamber while introducing a 10-s delay between actuation and measurement. We found that, in general, there were either no differences or no clinically relevant differences in the aerosol characteristics of albuterol HFA and ProAir when used alone, with a valved holding chamber, and with a valved holding chamber with a 10-s delay. However, Proventil had changes in percentage < 5 μm (30 and 15 s), percentage 1–3 μm (15 s), and fine-particle mass (30 s) when used alone and in fine-particle mass when used with a valved holding chamber with a 10-s delay. Proventil had the highest fine-particle mass, followed by ProAir. The latter appears to be the most stable of the different brands of albuterol HFA pMDI tested.
The aerosol characteristics of the pMDI alone of Ventolin and ProAir are similar to those reported by McCabe et al9 They reported an MMAD/GSD/fine-particle dose (calculated as mass for percentage < 5 μm) for Ventolin alone of 2.4 μm/2.0/26 μg, compared with our findings of 2.39 μm/1.41/29.3 μg. Similarly, they reported MMAD/GSD/fine-particle dose for ProAir alone of 2.3 μm/1.6/53 μg, and we measured 2.21 μm/1.43/42.9 μg.
Slator et al12 compared the percentage of label claim of ProAir HFA coupled to several valved holding chambers, including one similar to the one we used. They evaluated several variables, including the effect of delay between actuation and inhalation. They reported that the emitted dose decreased by 20% when a 10-s delay between actuation and measurement was introduced. We also found a significant effect of the delay resulting in a 34–39% decrease in fine-particle mass when compared with ProAir pMDI/valved holding chamber. The same phenomenon was seen for Ventolin (39–42%) and Proventil (27–32%). Our data are also consistent with the findings of Rau et al,13 who compared fine-particle mass of Ventolin HFA used with several valved holding chambers, including one similar to the one we used. They reported that increasing the delay between actuation and inhalation from 2 to 5 s resulted in a 20% decrease in fine-particle mass. This has to be kept in mind when diagnostic studies, such as response to bronchodilators, are done.
Hautman et al7 compared fine-particle mass of albuterol of the same inhalers we studied. They used intervals between actuations of 15, 30, 60, and 120 s and reported that fine-particle mass increased for ProAir alone and for Proventil and Ventolin with and without a valved holding chamber when interval time was increased from 15 to 120 s. Similarly, we found that the introduction of a delay resulted in a significant increase in fine-particle mass. The authors also reported that the use of a valved holding chamber results in an increase in fine-particle mass that is modest for ProAir but large for Ventolin and Proventil. Our data are consistent with their report. We speculate that the difference in magnitude seen between ProAir and the others is because its aerosol velocity is slower than the others.7,9 Hautman et al7 limited the particle size distribution analysis to fine-particle mass. Our study provides a more complete description of the aerosols and also introduces the effect of delay between actuation and measurement as novel data.
The clinical implications of our findings are severalfold. First, albuterol HFA pMDI either alone or with a valved holding chamber could be actuated with intervals < 60 s without affecting the aerosol characteristics. This would allow an increase in productivity for the practitioner administering the aerosol. Second, the use of a small-volume valved holding chamber made of nonelectrostatic material could optimize drug delivery. Finally, delays between actuation and inhalation should be avoided because of the negative effect on fine-particle mass. These data cannot be extrapolated to add-on devices that require the removal of the canister from the plastic actuator to be used and/or other valved holding chambers (ie, different volume or made from nonconductive material).
One limitation of our study is that we did not use any mechanical system to introduce the delay between actuation and testing.12,13 Another potential limitation of this study is that breathing simulation was not coupled to the measurement of particle size.
Conclusions
Decreasing the interval between actuations from 60 s to 30 and 15 s does not seem to affect the aerosol characteristics of ProAir and Ventolin. Although some changes were noticed for Proventil when decreasing the interval between actuations from 60 s to 30 and 15 s, the pMDI outperformed Ventolin that had the lowest fine-particle mass. Although the use of a valved holding chamber increased fine-particle mass, introduction of a 10-s delay between actuation and inhalation significantly reduced fine-particle mass.
Footnotes
- Correspondence: Ariel Berlinski MD, Pediatric Pulmonology Division, University of Arkansas for Medical Sciences, College of Medicine, 1 Children's Way, Slot 512-17, Little Rock, AR 72202. E-mail: BerlinskiAriel{at}uams.edu.
Dr Berlinski presented a version of this paper at the European Respiratory Society Meeting, held September 6, 2016, in London, United Kingdom.
Dr Berlinski has disclosed relationships with AbbVie, Anthera, Aptalis Pharma, Cempra, Janssen Research and Development, Gilead, National Institutes of Health, Novartis, Therapeutic Development Network, Vertex, and the International Pharmaceutical Aerosol Consortium on Regulation and Science. Mr Pennington was supported by a University of Arkansas for Medical Sciences College of Medicine Research Grant. Mr Pennington has disclosed no conflicts of interest.
See the Related Editorial on Page 1224
- Copyright © 2017 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}
{kind=link}