

Abstract
BACKGROUND: The outcomes of patients with tuberculosis admitted to an ICU remain undetermined. Herein, we reviewed the literature to describe the mortality of subjects with tuberculosis who are critically ill, and explore the effect of glucocorticoids on survival.
METHODS: A systematic review of medical literature databases was performed for studies that describe the outcome of subjects with tuberculosis who required ICU admission. We calculated the proportion of hospitalized subjects with tuberculosis who required ICU admission. Pooled estimates of ICU and hospital mortality, and tuberculosis-related ARDS were calculated. We also studied the effect of systemic glucocorticoids on survival of subjects with tuberculosis who were critically ill.
RESULTS: A total of 35 studies (N = 1,815) were included. The pooled proportion of hospitalized subjects with tuberculosis who required ICU admission was 3.4% (95% CI 1.6–5.7%). The pooled ICU and hospital mortality was 48% (95% CI 41–55%) and 54% (95% CI 46–62%), respectively. Tuberculosis-related ARDS was associated with higher odds (odds ratio 3.88, 95% CI 1.73–8.72) of death. The use of glucocorticoids was not related to an improvement in survival (odds ratio 0.65, 95% CI 0.27–1.57).
CONCLUSIONS: Tuberculosis is a rare cause of ICU admission but is associated with high mortality. Tuberculosis-related ARDS is also associated with lower survival. The role of glucocorticoids in patients with tuberculosis who are critically ill remains unclear and needs further evaluation.
Introduction
Tuberculosis is an important cause of morbidity and mortality globally. Occasionally, patients with tuberculosis may present acutely and require intensive care, especially those with rapid symptom onset.1–4 Despite decades of research, many facets of tuberculosis in patients who are critically ill remain unclear. For instance, the proportion of individuals with tuberculosis who require admission to an ICU has been variably reported, ranging from <1% to >8%.5,6 Even in countries with a high tuberculosis burden, the proportion of patients with tuberculosis who require ICU admission is different across centers.6,7 Similarly, the survival and the factors responsible for mortality among patients with tuberculosis who are critically ill are uncertain, despite the availability of effective antituberculosis therapy and improvement in the standards of ICU care.6,7
In some but not all studies, the presence of ARDS and miliary tuberculosis has been shown to be associated with high mortality.5–9 Systemic glucocorticoids are often used in patients with tuberculosis who are critically ill, with an aim to improve survival. In fact, in a recent meta-analysis, the use of systemic glucocorticoids was shown to improve survival.10 However, this study did not specifically report the outcomes in subjects with tuberculosis who were critically ill. Thus, the role of systemic glucocorticoids in the those who are critically ill still remains speculative.1,5 The current review was performed to ascertain mortality in subjects with tuberculosis who were critically ill and who required ICU care. We also investigated whether the use of systemic glucocorticoids improves survival in subjects with tuberculosis who were critically ill.
Methods
This review was reported in accordance with the guidelines of PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement.11 Ethics committee approval was not required because this was a systematic review of published data.
Search Strategy
We searched the PubMed, Embase, and Scopus databases from inception until May 1, 2017, for studies that describe outcomes of subjects with tuberculosis who required ICU admission. We used the following free-text terms: (“tuberculosis” or “TB” or “Mycobacterium tuberculosis” or “MTB” or “pulmonary TB” or “extrapulmonary TB”) and (“critical care” or “intensive care unit” or “ICU” or “respiratory failure” or “ARDS” or “acute lung injury” or “acute respiratory distress syndrome” or “adult respiratory distress syndrome” or “ALI” or “ARF” or “acute hypoxic respiratory failure” or “hypoxic respiratory failure”). The reference lists of all the included articles and previous review articles were reviewed to search for additional studies.
Inclusion Criteria
We included studies that describe the course of subjects with active tuberculosis who required ICU admission. The following were excluded: (a) case series with <10 subjects, case reports, correspondence, letters, editorials, conference abstracts, and reviews; (b) studies that did not provide information about outcomes; (c) studies published in non-English language; (d) animal studies; (e) studies that primarily included subjects with tubercular meningitis or sequelae of tuberculosis in the past; and, (f) studies conducted outside the ICU setting.
Initial Review of Studies
A database was created from the electronic searches by using the reference manager Endnote (version X8, Clarivate Analytics, Philadelphia, Pennsylvania), and duplicate citations were discarded. Two authors (VM, ISS) screened these citations and identified the relevant studies from the title and abstract. Any disagreement was resolved by discussion between these two authors. After scrutinizing the database to include only primary articles, the full texts of these studies were obtained and reviewed in detail.
Study Selection and Data Abstraction
All the studies were independently assessed by 2 authors (VM, ISS) for inclusion in the systematic review. Data were then extracted and entered into a standard data abstraction form. The following information was recorded: (i) details of publication (authors, country, and year of publication); (ii) study design (prospective or retrospective); (iii) criteria used for making a diagnosis of tuberculosis; (iv) number of subjects (including the demographic profile) and the inclusion criteria; (v) presence of comorbid illness(es); (vi) proportion of subjects with drug-resistant tuberculosis and past history of tuberculosis; (vii) details and duration of mechanical ventilation, length of hospital and ICU stay; (viii) treatment regimen used; (ix) use of glucocorticoids; (x) factors predicting mortality; and (xi) the final outcome.
Assessment of Study Quality
Two authors (VM, ISS) independently assessed the quality of the included studies by using the QualSyst tool. The QualSyst tool includes a set of 10 questions, with each question having a possible score of 0, 1, or 2.12 Interobserver agreement for the selection of studies was assessed by using the weighted Cohen's kappa.
Data Analysis
The statistical software packages RevMan (Review Manager, version 5.3, 2014, The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark) and StatsDirect (version 3, StatsDirect, Cambridge, United Kingdom) were used to perform the statistical analyses.
Determination of the Pooled Effect
For each study, we calculated the proportion with 95% CI of hospitalized subjects with tuberculosis who required ICU admission, and the proportion of subjects with tuberculosis in an ICU. We calculated the ICU and hospital mortality among subjects with tuberculosis admitted to the ICU for the individual studies. Forest plots were constructed to display the pooled results by using the random effects model.
Sensitivity Analysis
Sensitivity analysis was planned to estimate the crude odds ratio with 95% CI of mortality in tuberculosis-related ARDS and miliary tuberculosis. The mortality in subjects with tuberculosis who were critically ill and treated with glucocorticoids was also analyzed.
Assessment of Heterogeneity
Heterogeneity for the individual outcomes was assessed by using the I2 test, with a value of ≥50%, which indicated significant heterogeneity.13
Results
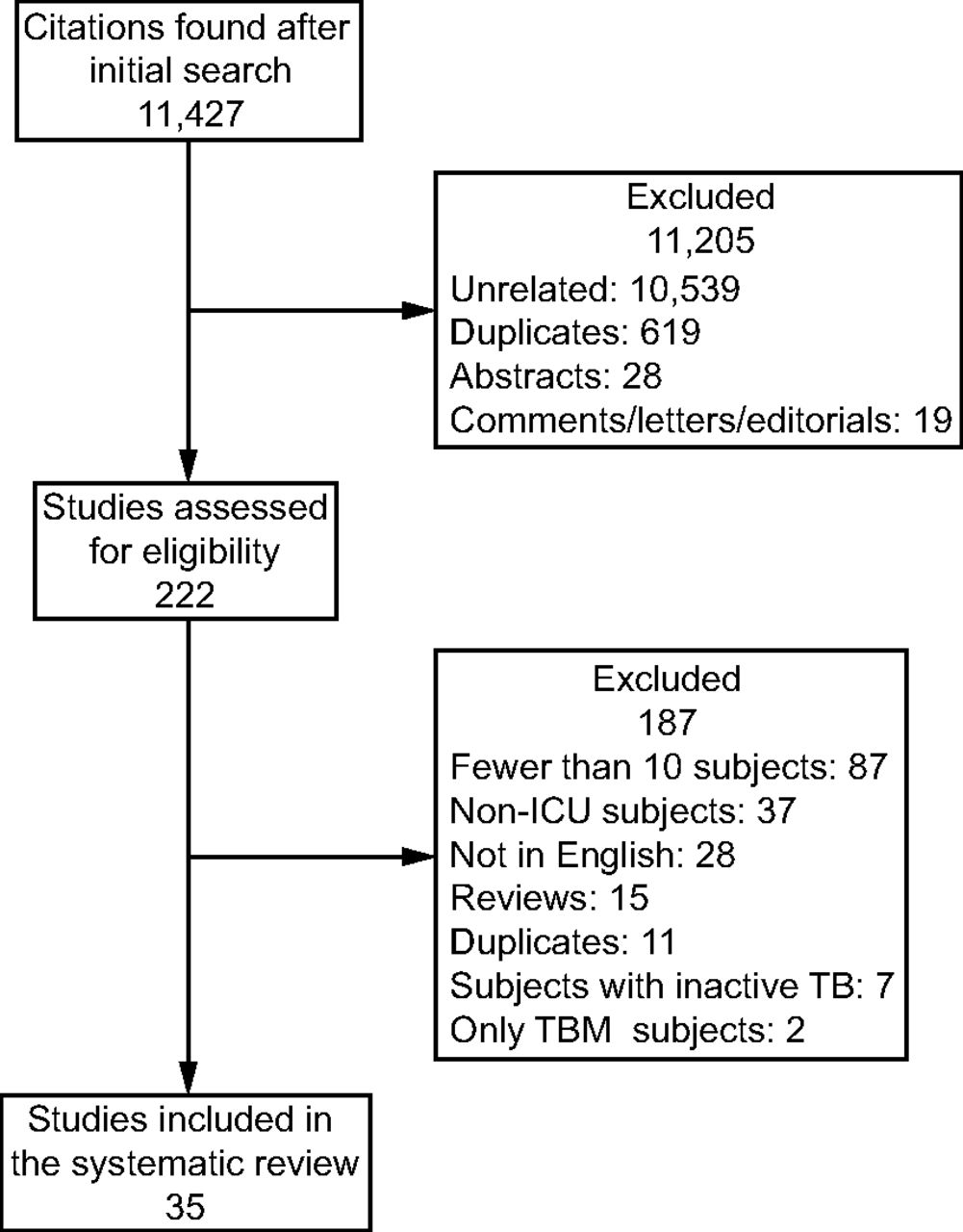
The initial database search yielded 11,427 citations, of which 35 studies (N = 1,815) were included in the current analysis (Fig. 1).1–3,5–7,16–44 All the studies except two3,35 had a retrospective study design. Of the included studies, 19 studies were from high tuberculosis burden countries.2,3,5–7,18,19,22–24,26–28,31,35,37,39,42,43 One study each exclusively included subjects who were critically ill with chronic kidney disease29 or with human immunodeficiency virus42 and affected with tuberculosis. Six studies included only subjects with tuberculosis-related ARDS.5–7,23,31,41 The most common indication for ICU admission was acute respiratory failure (mean 64.1%, 95% CI 53.5–74.7%) (Table 1). The common causes of acute respiratory failure were pneumonia and ARDS (with or without miliary tuberculosis).25,33

Flow chart. TB = tuberculosis; TBM = tuberculosis meningitis.
Summary of Studies Describing Subjects With Tuberculosis Who Were Critically Ill and Required ICU Admission
The other indications for ICU admission included sepsis (with or without shock), neurologic dysfunction, hemoptysis, and multiorgan failure (Table 1). The proportion of subjects with a prior history of tuberculosis (6 studies) ranged from 3 to 50%, whereas the proportion of subjects with multidrug-resistant tuberculosis (17 studies) ranged from 0 to 17%. The proportion of subjects who required mechanical ventilation was between 37.9 and 100% (Table 2). Invasive mechanical ventilation was the most common form of ventilation. The duration of mechanical ventilation was between 3 and 40 d. The ICU length of stay (5–28 d) and the hospital length of stay (13–87 d) was also variable.
Description of Hospital and ICU Outcomes and Complications
Nosocomial pneumonia, ventilator-associated pneumonia, urinary tract infection, and bacteremia were the common hospital-acquired complications. Pneumothorax due to mechanical ventilation was reported between 4 to 17% of the subjects (Table 2). The major factors that contributed to an ICU or hospital mortality included the presence of multiorgan failure, sepsis, development of nosocomial infections, cardiogenic shock, and refractory hypoxemia (see Supplemental Table 1 at http://www.rcjournal.com). One study described predictors of developing ARDS in subjects with tuberculosis who were critically ill.6 These included miliary tuberculosis, shorter duration of illness (<30 d), lymphopenia (<1,625 cells/mm3) and elevated serum alanine aminotransferase (>100 IU).6
Fifteen studies described the use of systemic glucocorticoids (see Supplemental Table 2 at http://www.rcjournal.com).1,5,6,18,21,23–25,27,28,31,40,41,43,44 The common indications for the use of glucocorticoids were miliary tuberculosis, respiratory failure, ARDS, and shock. Eight studies compared mortality in subjects with and without glucocorticoids (Supplemental Table 2).1,5,24,27,28,40,43,44 Only one study provided the details of dose and duration of glucocorticoids (methylprednisolone, 80 mg/d for 5 d) used.5
Quality of Studies
Most of the included studies were of poor quality, with a median (interquartile range) QualSyst score of 11 (10–13) (see Supplemental Table 3 at http://www.rcjournal.com). The interobserver agreement for scoring the study quality was good (weighted Cohen's kappa = 0.92).
Pooled Proportion of Subjects With Tuberculosis Who Were Critically Ill
The proportion of all hospitalized subjects with tuberculosis who required ICU admission was between 0.5% and 8.4%, with a pooled proportion of 3.4% (95% CI 1.6–5.7, I2 = 96.6%, P < .001) (see Supplemental Fig. 1 at http://www.rcjournal.com).5,6,16,18,24,25,32,40 The pooled proportion of all subjects with tuberculosis as an indication for ICU admission was 2.3% (95% CI 1.1–4, I2 = 95.5%, P < .001).7,17,19,22,28,35
Pooled Effect
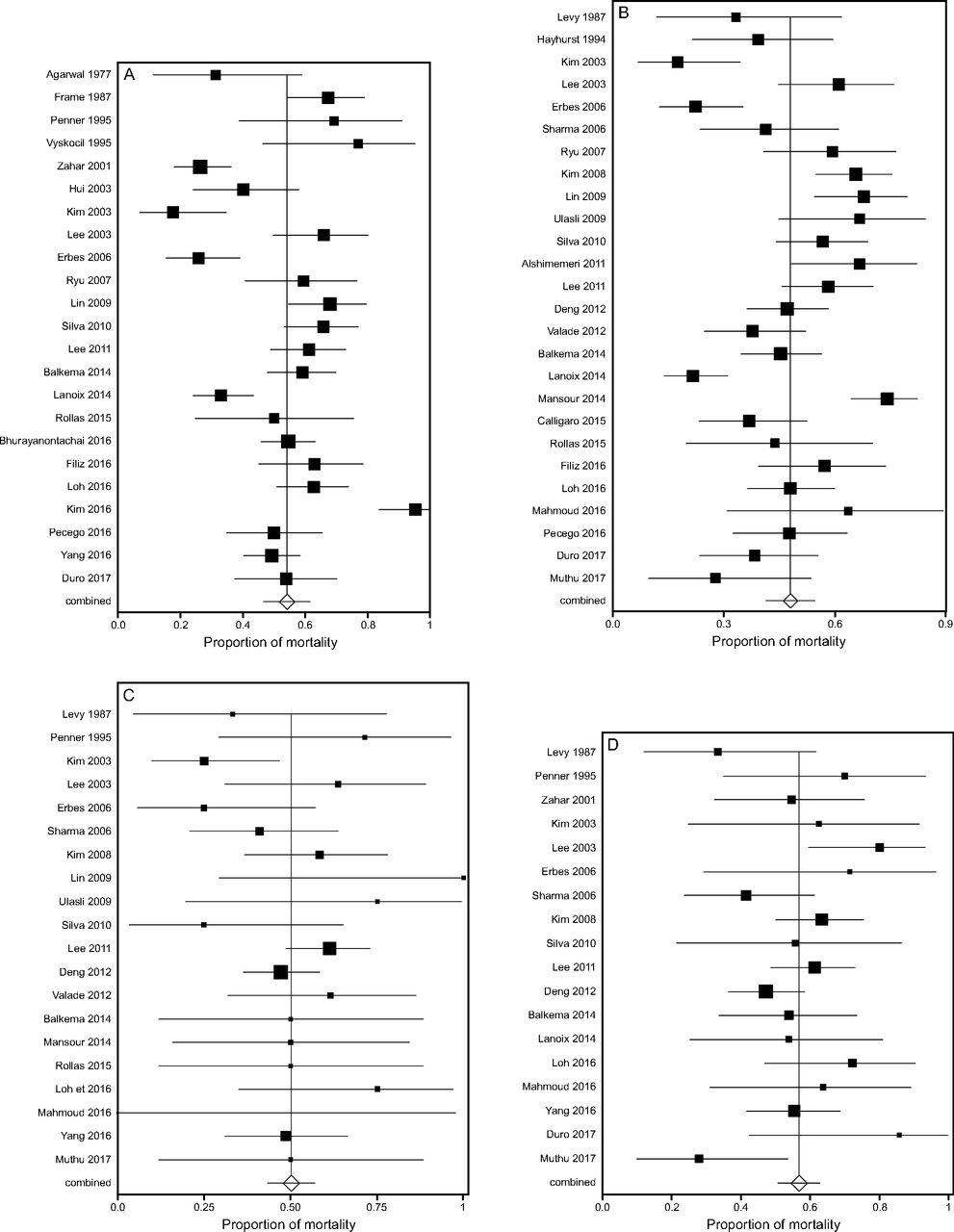
The mortality of subjects with tuberculosis who are critically ill varied from 17 to 67%.1–3,5–7,16–44 The pooled ICU (26 studies [n = 1,282])2,3,5–7,18,19,23–26,38,40–42,44 and hospital mortality (23 studies [n = 1,283])1,3,16,17,20–26,28,31,33,36–40,42–44 was 48% (95% CI 41–55%, I2 = 86.11%, P < .001) and 54% (95% CI 46–62%, I2 = 92.58%, P < .001), respectively (Fig. 2).

Forest plots depicting hospital mortality (A), ICU mortality (B), mortality in miliary tuberculosis (C), and mortality in subjects with tuberculosis-related ARDS (D), among subjects with tuberculosis who required ICU admission. The proportion of mortality in individual studies is represented by a square through which runs a horizontal line (95% CI). Pooled mortality is represented by the diamond and the 95% CI is represented by the line running through it.
Sensitivity Analysis
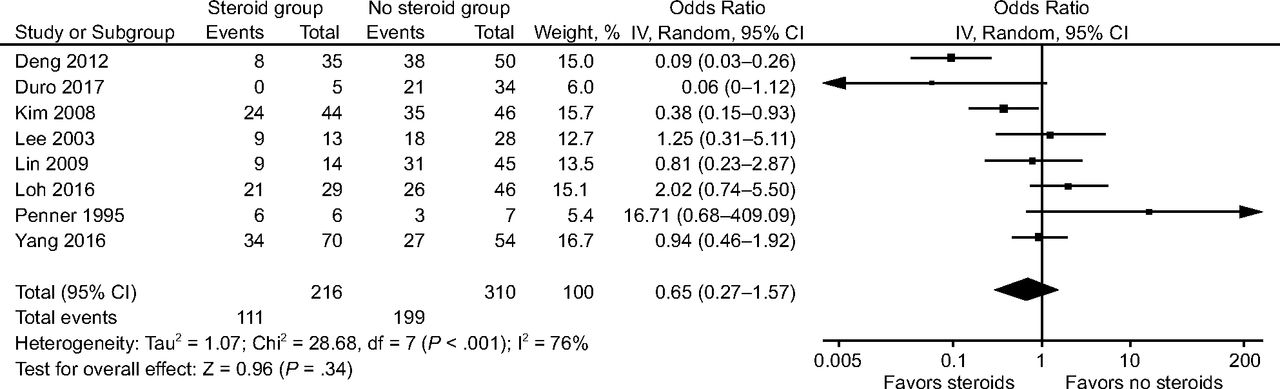
The pooled mortality in subjects with miliary tuberculosis (20 studies [n = 354])1–3,5–7,18,23–25,27–29,31,32,34,36,40,41,43 and tuberculosis-related ARDS (18 studies [n = 486])1–3,5–7,18,21,23–25,27,31,33,40,41,43,44 was 50% (95% CI 43–57%, I2 = 43.6%, P = .02) and 57% (95% CI 51–63%, I2 = 53.3%, P = .004), respectively (Fig. 2). Tuberculosis-related ARDS (9 studies, n = 587)2,3,23–25,27,33,40,44 was found to be associated with higher odds of death compared with non-ARDS tuberculosis (pooled odds ratio 3.88, 95% CI 1.73–8.72, I2 = 68%, P = .02) (Fig. 3). The presence of miliary tuberculosis (16 studies, n = 776)2,3,6,7,18,23–25,27–29,32,34,36,40,41 did not increase the risk of death vis-a-vis non-miliary tuberculosis (pooled odds ratio 1.15, 95% CI 0.71–1.87, I2 = 74%, P = .24) (Fig. 3). The use of systemic glucocorticoids (8 studies, n = 526)1,5,24,27,28,40,43,44 did not improve survival in subjects with tuberculosis who were critically ill (odds ratio 0.65, 95% CI 0.27–1.57, I2 = 76) (Fig. 4). One study described the use of glucocorticoids exclusively in subjects with tuberculosis-related ARDS and found a reduction in mortality.5

Forest plots, depicting the comparison of mortality in subjects who were critically ill with or without miliary tuberculosis (A) and tuberculosis with or without ARDS (B). The odds ratio of mortality in individual studies is represented by a square through which runs a horizontal line (95% CI). Pooled odds ratio is represented by the diamonds.

Forest plot, depicting the mortality in subjects with tuberculosis who were critically ill with or without the use of systemic glucocorticoids. The odds ratio of mortality in individual studies is represented by a square through which runs a horizontal line (95% CI). The diamond represents the pooled odds ratio.
Heterogeneity
There was significant heterogeneity in the included studies. The I2 value was 86.1% and 92.6% for studies that describe the ICU and hospital mortality, respectively.
Publication Bias
Publication bias was assessed for studies by estimating the proportion of subjects with tuberculosis in the ICU, proportion of hospitalized subjects with tuberculosis who required ICU and studies reported ICU and hospital mortalities. There was publication bias on visual inspection of the funnel plot (see the Supplemental Fig. 2 at http://www.rcjournal.com); however, there was no evidence of publication bias on the Egger test14 (P = .92, P = .66, P = .37, and P = .67 for hospital mortality, ICU mortality, mortality due to miliary tuberculosis, and ARDS, respectively) and the Begg-Mazumdar test15 (P = .71, P = .97, P = .61, and P =.92 for hospital mortality, ICU mortality, mortality due to miliary tuberculosis, and ARDS, respectively).
Discussion
The results of this meta-analysis indicated that tuberculosis is an uncommon indication for ICU admission (3.4% of hospitalized subjects with tuberculosis and 2.3% of all ICU admissions). The overall mortality of subjects with tuberculosis who were critically ill was high (48% and 54%, ICU and hospital mortality, respectively), with tuberculosis-related ARDS having higher odds of death compared with those without ARDS. The use of systemic glucocorticoids did not improve survival in subjects with tuberculosis who were critically ill.
Tuberculosis remains an uncommon indication for ICU admission. Early detection, availability of effective anti-tuberculosis therapy, and assurance of high adherence to anti-tuberculosis therapy under directly observed therapy could explain the lower prevalence of tuberculosis in the ICU. However, it might also be possible that patients with tuberculosis who are critically ill are not admitted to the ICU due to the lack of infection control measures, such as negative pressure rooms, requisite air exchanges, and high efficiency particulate air filtration, especially in resource-constrained settings.45
Once admitted to the ICU, there is high mortality in individuals with tuberculosis who are critically ill, and this has been attributed to several factors. These include the presence of comorbid illness, delay in initiating anti-tuberculosis therapy, unpredictable pharmacokinetics, and pharmacodynamics of anti-tuberculosis therapy in the patient who is critically ill, disseminated tuberculosis, ARDS, drug-resistant tuberculosis, delay in identifying patients with tuberculosis at a higher risk of mortality, and the lack of use of objective criteria for risk stratification.1,4,32 The high mortality could also reflect a referral bias with the sickest of patients getting admitted to ICU.37 Finally, infection with Mycobacterium tuberculosis may suppress monocyte expression that causes a state of immunosuppression that could possibly increase the risk for secondary infections.39,46 Development of nosocomial infection was associated with increased mortality in some studies.2,28
Tuberculosis is an unusual cause of ARDS and is believed to result from inflammation mounted against mycobacterial cell wall components, similar to bacterial sepsis.47 The pooled analysis in the current study indicated that the occurrence of ARDS in tuberculosis was associated with higher odds of mortality compared with subjects with tuberculosis but without ARDS. However, tuberculosis-related ARDS behaves like ARDS due to any other etiology.9,48 In a recent study, no difference was observed in outcomes between subjects with tuberculosis-related ARDS and ARDS due to other causes.7 Miliary tuberculosis is considered to be associated with high mortality because it signifies mycobacteremia. However, we found the survival to be similar in subjects with or without miliary tuberculosis.
In a recent meta-analysis, the use of glucocorticoids was found to reduce mortality in all forms of tuberculosis, including pulmonary tuberculosis.10 However, the analysis predominantly included subjects with meningitis and not specifically subjects who were critically ill.10 Contrary to the previous study, our study did not find any survival benefit with the use of systemic glucocorticoids. The lack of benefit with glucocorticoids could be due to the variable dose and duration in these studies.5,43 Also, patients who are critically ill and are treated with glucocorticoids represent an even sicker group of individuals and leads to a selection bias. Thus, the role of systemic glucocorticoids in individuals who are critically ill remains unclear and needs further evaluation in prospective studies.
Our review had a few limitations. Most studies included in the review had a retrospective study design with a limited number of subjects. However, a prospective study seemed impractical due to the low frequency of patients with tuberculosis being admitted to the ICU. The results of this meta-analysis could not be extrapolated to patients with human immunodeficiency virus infection, meningeal tuberculosis, and drug-resistant tuberculosis because separate information was not available for such individuals. In one study that exclusively involved subjects with tuberculosis and human immunodeficiency virus who were critically ill, the ICU mortality (52%) was similar to the pooled mortality observed in the current analysis although the time to death was shorter in subjects with lower CD4 counts.42 The odds for ARDS and miliary tuberculosis mortality were calculated by using the numbers of cases and controls reported. Therefore, “crude” odds ratio of death was provided in this review and may not represent the true burden of ARDS and miliary tuberculosis on death. There also was significant heterogeneity in the criteria used to define tuberculosis and the regimen of anti-tuberculosis therapy used. Also, most of the studies were of short duration and did not report on the long-term outcomes. Finally, the role of glucocorticoids in subjects with tuberculosis-related ARDS and miliary tuberculosis could not be ascertained because the individual studies did not provide this information.
Conclusions
Tuberculosis is an uncommon cause of ICU admission, with a high ICU mortality. The role of systemic glucocorticoids in patients with tuberculosis who are critically ill remains unclear and needs further evaluation.
Footnotes
- Correspondence: Inderpaul Singh Sehgal MD, DM, Department of Pulmonary Medicine, Postgraduate Institute of Medical Education and Research, sector 12, Chandigarh, India 160012. E-mail: inderpgi{at}outlook.com.
The authors have disclosed no conflicts of interest.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2018 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}
{kind=link}