

Abstract
BACKGROUND: High-flow nasal-cannula (HFNC) may be an oxygen modality useful for preventing invasive mechanical ventilation and mortality; however, its role in acute hypoxemic respiratory failure is not clearly defined. We sought to evaluate the impact of HFNC on mortality across immunocompromised subjects compared to alternative noninvasive oxygen therapies, namely conventional oxygen therapy and noninvasive ventilation (NIV).
METHODS: We systematically searched the major databases to identify randomized, controlled trials (RCTs) or observational studies (until May 2018). We included studies reporting the use of HFNC in immunocompromised subjects and evaluated its impact on mortality and invasive mechanical ventilation.
RESULTS: Upon review of 6,506 titles, 13 studies (1,956 subjects) fulfilled our inclusion criteria (4 RCTs, 9 observational studies). The predominant cause of immunocompromised status was cancer. Bacterial pneumonia was the most common cause of acute hypoxemic respiratory failure with a median PaO2/FIO2 of 145 mm Hg (interquartile range 115–175). HFNC was used as the first oxygen strategy in 474 subjects compared to NIV (242 subjects) and conventional O2 therapy (703 subjects). There was a 46% rate of invasive mechanical ventilation and 36% mortality. Mortality at the longest available follow-up was lower with HFNC compared to the oxygen therapy controls (NIV or conventional O2 therapy) in 7 studies (1,429 subjects; relative risk 0.72, 95% CI 0.56–0.93, P = .01). There was a lower rate of invasive mechanical ventilation with HFNC compared to the oxygen therapy controls across 8 studies (1,529 subjects, relative risk 0.81, 95% CI 0.67–0.96, P = .02). These results were robust across a series of sensitivity analyses.
CONCLUSIONS: There exists a need to develop a greater evidence base evaluating the utility of HFNC in immunocompromised subjects. In our exploratory analysis, HFNC was found to decrease mortality and use of invasive mechanical ventilation compared to alternative noninvasive oxygen controls. These results are meant to be exploratory. Higher-quality studies evaluating a more homogeneous population are needed to further elucidate its benefit.
Introduction
Acute hypoxemic respiratory failure (AHRF) is the most common cause of critical illness in immunocompromised patients.1 Patients who progress to require invasive mechanical ventilation are subject to increased mortality.2 Increased mortality may be attributed to many factors, including aggressive or drug-resistant pathogens, greater frailty at the time of ICU admission, and host response.3–5
In hypoxemic immunocompromised patients, noninvasive oxygen therapy may be delivered via simple face mask (conventional oxygen therapy), through noninvasive ventilation (NIV), or with a high-flow nasal cannula (HFNC). Although earlier studies in immunocompromised subjects receiving NIV compared to conventional O2 therapy suggested a reduced need for intubation, these results have been called into question in recent years.6–8 One trial included a predominantly solid organ transplant population with pulmonary edema, for which there is ample evidence of benefit of NIV7; another trial was composed of subjects with hematologic malignancy who had a mortality rate in excess of 80%, a finding that has changed in recent years.6 These findings have been challenged by more recent evidence suggesting a lack of benefit with NIV.8–11
The HFNC is a newer device that has recently been shown to provide a survival benefit in critically ill, non-immunocompromised, hypoxemic patients compared to use of NIV or conventional O2 therapy.12 However, this evidence has been inconsistent across the literature.13,14 The mechanisms of effect that lead to better oxygenation include washout of CO2 from the anatomical dead space, generation of PEEP, and more stable FIO2 due to the higher flows administered.15,16 Furthermore, in contrast to low-flow systems, heated humidification prevents airway dryness, preserving mucociliary function and enhancing clearance of secretions.15,16
It is unclear whether these promising results with HFNC translate to the immunocompromised population. With the goal to reserve intubation in those failing noninvasive oxygenation strategies, there is a need to better understand these therapies in this unique population. Therefore, we undertook a systematic review to review the body of literature to date (as of May 2018) to examine the use of HFNC compared to other modalities of oxygenation in immunocompromised subjects with AHRF. We evaluated the data for homogeneity and considered performing a meta-analysis to determine the impact of HFNC on mortality and invasive mechanical ventilation. Any meta-analyses performed are intended only for the generation of hypotheses.
Methods
Search Strategy
A comprehensive search strategy was developed to identify published literature on the use of HFNC (see the supplementary materials at http://www.rcjournal.com). At the time of the search, specific subject headings for high-flow therapy were unavailable in the databases used. The strategy was devised using an extensive list of appropriate text words and phrases. Key words were either mined from sample articles and product descriptions or generated through input from subject specialists on the team. The search was not focused on any particular population, outcome, or study type to keep it sufficiently sensitive.
The following databases were searched from inception through May 15, 2018: MEDLINE, MEDLINE In-Process & Other Non-Indexed Citations, Embase, Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Clinical Trials, and CINAHL. Additionally, we searched a clinical trials registry (http://clinicaltrials.gov) for unpublished and ongoing studies. A supplementary search was conducted in PubMed for non-MEDLINE records. No language restrictions were applied.
Study Selection
Eligibility was determined by 2 reviewers (MCS, AM). Studies of HFNC for AHRF including only immunocompromised subjects were independently selected and reviewed by reviewers. Disagreements were resolved by consensus or in discussion with a senior author (LM). We included any observational studies or randomized, controlled trials (RCTs) of adult immunocompromised subjects undergoing HFNC for AHRF. RCTs were included if HFNC was compared to NIV or conventional O2 therapy. If both HFNC and NIV were included in a cohort, the cohort was categorized based upon which modality predominated in a 24-h period. We excluded pediatric studies and studies involving the application of HFNC in the postextubation or peri-procedural setting.
Study Outcomes
After our descriptive review, we inspected each study for clinical heterogeneity to evaluate the feasibility of performing a meta-analysis. Our primary outcome of interest was mortality at the longest available time point reported comparing HFNC to any oxygen therapy control (ie, a combination of NIV or conventional O2 therapy). Secondary outcomes included the rate of invasive mechanical ventilation for HFNC compared to an oxygen therapy control (NIV or conventional O2 therapy) during that hospitalization. We conducted subgroup analyses evaluating mortality and invasive mechanical ventilation in the subgroups of the oxygen therapy control (HFNC vs NIV and HFNC vs conventional O2 therapy). We performed a sensitivity analysis restricting the meta-analysis to RCTs and observational studies that used propensity-score matching. Finally, across studies that conducted multivariable analysis, we evaluated factors that were found to be statistically significantly associated with mortality and invasive mechanical ventilation across this population.
Data Abstraction and Study Quality
Data from included studies were independently abstracted by the reviewers using a standardized data collection form. Study design, patient demographics, immunocompromised status, characteristics of oxygen delivery methods, and patient outcomes were collected. Two authors (MCS and AM) independently assessed potential sources of bias using the Cochrane Collaboration Risk of Bias Tool17 for RCTs and the Newcastle-Ottawa Scale for observational studies.18
Data Analysis
Data were summarized using medians and interquartile ranges (IQRs) or mean ± SD where appropriate. For the meta-analyses, we compared HFNC to oxygen therapy control (combination of conventional O2 therapy or NIV) for our primary analysis. Meta-analysis included RCTs or any observational studies and were weighted using the inverse variance method. Categorical outcomes were evaluated using relative risk (RR). Study results were pooled using Review Manager (RevMan version 5.2; Cochrane Collaboration, Oxford, United Kingdom) with a 2-sided significance level of 5%. Individual study and summary results are reported with risk ratios and 95% CIs. Random effects models were used for all analyses.19 Statistical heterogeneity among trials was assessed using the I2 statistic, defined as the percentage of total variability across studies attributable to heterogeneity rather than chance, and using published guidelines for low (I2 = 25–49%), moderate (I2 = 50–74%), and high (I2 ≥ 75%) heterogeneity.20
Results
Search Results
Our search strategy identified 6,506 citations. Further screening of 223 full texts yielded a total of 13 studies that fulfilled our inclusion criteria and focused on immunocompromised subjects (see PRISMA Flow Diagram in the supplementary materials at http://www.rcjournal.com).21–33
Characteristics of Included Studies
Thirteen studies reporting on 1,956 subjects were included in this systematic review. The studies included 8 retrospective, cohort studies (532 subjects),22–24,27,30–33 1 prospective observational study (915 subjects, 859 of whom were appropriate for analysis),21 and 4 RCTs, 2 of which were post hoc analyses of previous RCTs (565 subjects) (Table 1).25,26,28,29 Two of the observational studies and 1 post hoc analysis of a previous RCT used propensity-score matching techniques.28,29,31 Nine studies compared HFNC to an oxygen therapy control (3 NIV/conventional O2 therapy, 3 NIV, 3 conventional O2 therapy). Outcomes of interest for our meta-analysis were reported in 8 studies (1,529 subjects, 3 RCTs, 1 prospective observational study, 4 retrospective cohort studies).21,24,26–29,31,32 The 4 RCTs were not considered to be at high risk of bias; however, they were unblended, and 2 of the 4 were post hoc analyses of randomized trials.28,29 The observational studies were of moderate to high quality with 6–9 points awarded on the Newcastle Ottawa Scale (see the supplementary materials at http://www.rcjournal.com).
Study Characteristics
Immunocompromised Population
Immunocompromised Population and Acute Hypoxic Respiratory Failure
The leading cause of immunosuppression was related to an oncologic diagnosis with a predominance of hematologic malignancy (11 of 13 studies). Two studies focused primarily on solid organ transplant.24,32 Infectious pneumonia (mainly bacterial) was the predominant cause of respiratory failure across this cohort (49–83%). Fungal infections, where reported, were found in 3–15% of cases. Opportunistic infections, particularly Pneumocystis jirovecii pneumonia, were reported in 7–24% of cases and was the primary focus of 1 study.33 The rates of no diagnosis for AHRF ranged from 4% to 13%.
There existed variable definitions of AHRF (Table 3), with most subjects demonstrating moderate hypoxia despite supplemental oxygen or tachypnea. HFNC was initiated in the emergency department, acute care ward, or ICU, with the latter being the most common site of initiation (10 of 13 studies). The median PaO2/FIO2 across the studies was 145 mm Hg (IQR 115–175). The duration of HFNC therapy varied widely, ranging from 2 h to 80 h. HFNC FIO2 ranged from 0.60 to 1.00 with flows of 21–60 L/min (Table 3). Rates of intubation varied across the studies given the variable time points of assessment. In 1 study, the need for intubation was reported at 9% 24 h after HFNC initiation.26 For the remaining studies that evaluated intubation rates at 28 d or hospital discharge, a median intubation rate of 46% (IQR 25–67%) was reported. The longest follow-up mortality time points are reported in Table 3 with a median mortality of 36% (IQR 14–58%).
High-Flow Nasal Cannula Details
Mortality and Intubation/Invasive Mechanical Ventilation
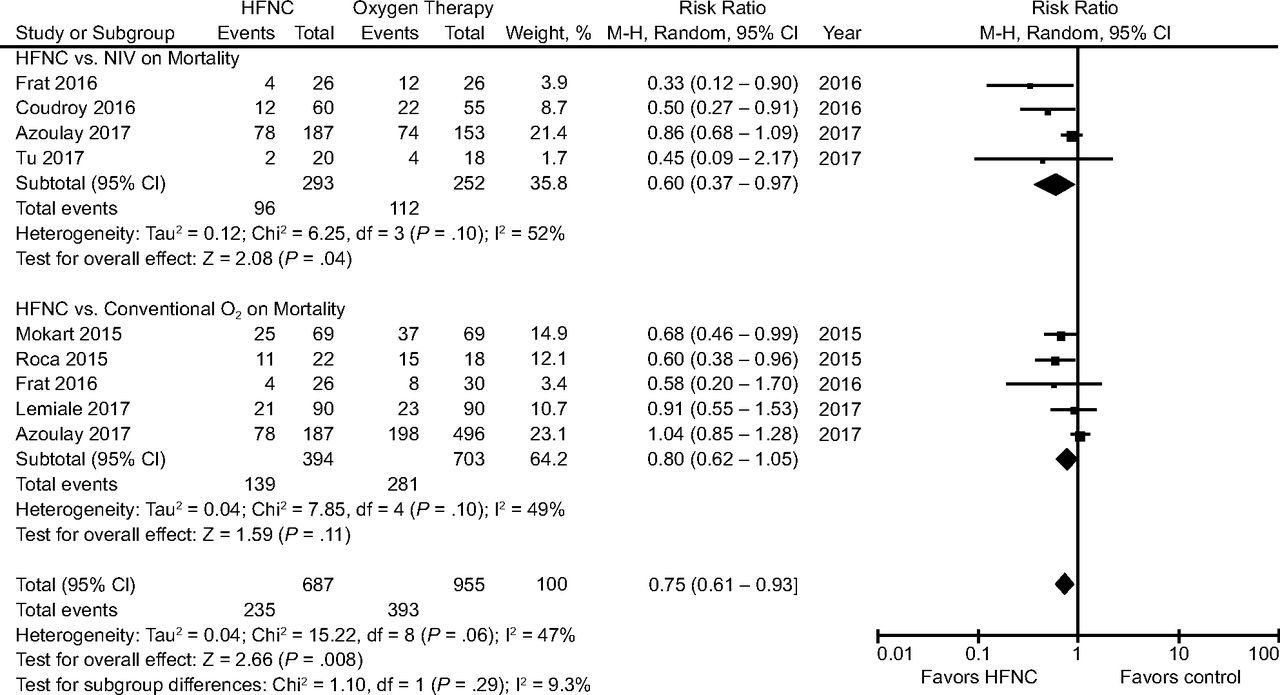
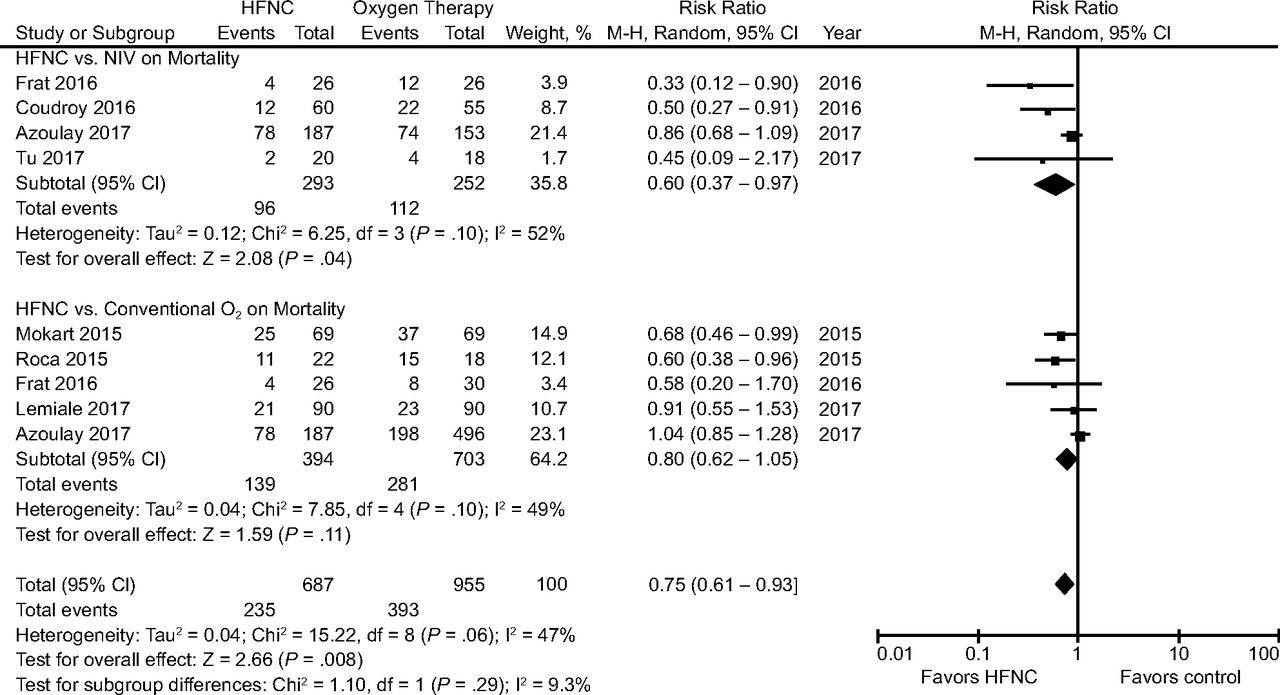
Mortality at the longest available follow-up was reported in 7 studies (1,429 subjects).21,24,27–29,31,32 Using a random effects model, HFNC compared to an oxygen therapy control (NIV or conventional O2 therapy) was associated with a decreased mortality (RR = 0.72, 95% CI 0.56–0.93; I2 = 48%, P = .01) (Fig. 1A). Eight studies reported on the need for intubation and invasive mechanical ventilation (1,529 subjects).21,24,26–29,31,32 HFNC was found to be associated with a decreased need for invasive mechanical ventilation compared to an oxygen control (conventional O2 therapy or NIV) (RR = 0.81, 95% CI 0.67–0.96; I2 = 34%, P = .02) (Fig. 1B). These results were similar when restricted to RCTs and matched observational studies only (see the supplementary materials at http://www.rcjournal.com).

A: Forest plot depicting HFNC compared to oxygen control (continuous oxygen therapy or noninvasive ventilation) on mortality across randomized trials and observational studies. Mortality time point used was 90 d for Azoulay et al and Frat et al, hospital mortality for Tu et al and Roca et al, and 28 d for Lemiale et al, Coudroy et al, and Mokart et al. The results demonstrate a decreased mortality with the use of HFNC with a risk ratio of 0.72 (95% CI 0.56–0.93), I2 48%, P = .01 using a random effects model. B: Forest plot depicting the effect of HFNC compared to oxygen control (continuous oxygen therapy or noninvasive ventilation) on rates of intubation across randomized trials and observational studies. The results demonstrate a decreased risk of intubation with the use of HFNC with a risk ratio of 0.81 (95% CI 0.67–0.96), I2 34%, P = .02 using a random effects model.
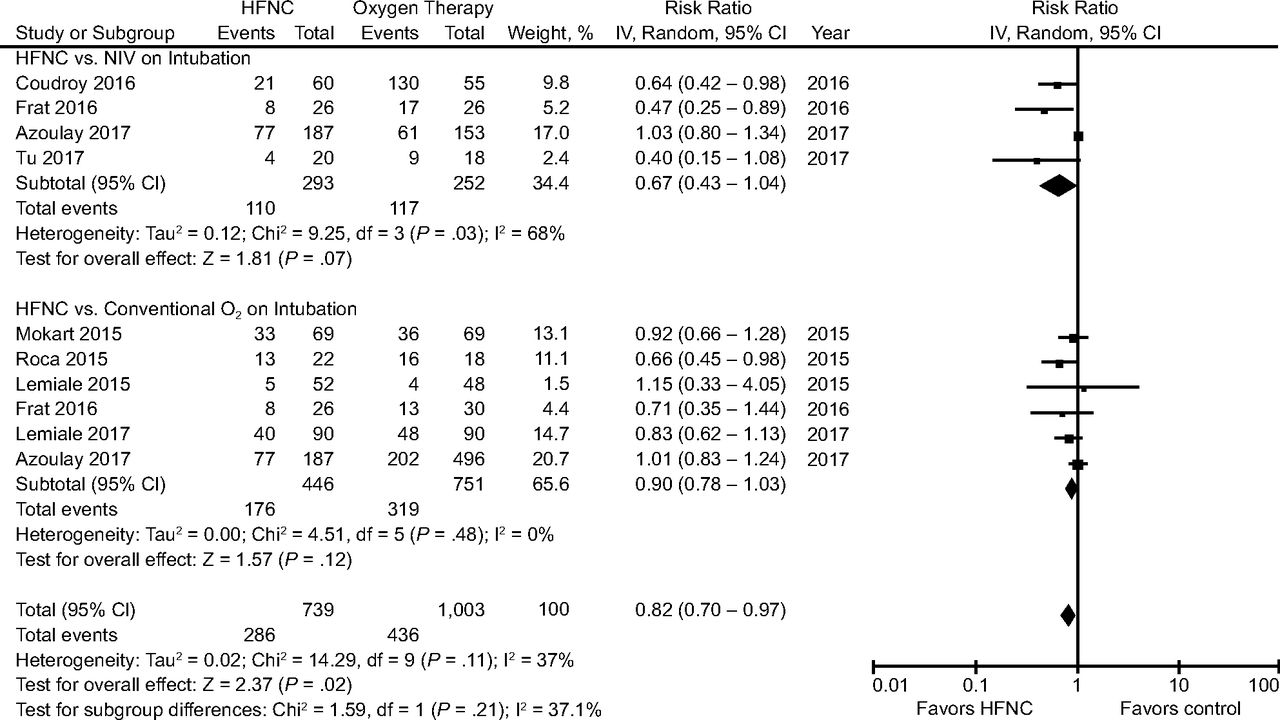
Across the subgroups of oxygen therapy controls (NIV or conventional O2 therapy), HFNC compared to NIV was found to be associated with a decreased mortality (4 studies, with 545 subjects; RR = 0.60, 95% CI 0.37–0.97; I2 = 52%, P = .04)21,24,27,28 but not conventional O2 therapy (5 studies, with 1,097 subjects; RR = 0.80, 95% CI 0.62–1.05; I2 = 49%, P = .11) (Fig. 2).21,28,29,31,32 In the subgroup analysis comparing HFNC to NIV, there was no difference in rates of invasive mechanical ventilation (4 studies, with 545 subjects; RR = 0.67, 95% CI 0.43–1.04; I2 = 68%, P = .07) (Fig. 3).21,24,27,28 There was also no difference in rates of invasive mechanical ventilation comparing HFNC to conventional O2 therapy (6 studies, with 1,197 subjects; RR = 0.90, 95% CI 0.78–1.03; I2 = 0%, P = .12) (Fig. 3).21,26,28,29,31,32 The results are summarized in Table 4 and Table 5.
Forest plot depicting HFNC compared to NIV or conventional oxygen therapy on mortality across randomized trials and observational studies. Mortality time point used was 90 days for Azoulay et al and Frat et al, in-hospital for Roca et al, and 28 days for Lemiale et al and Mokart et al. The results demonstrate a difference in mortality using a random effects model comparing HFNC vs. NIV but not HFNC vs conventional oxygen therapy.

Forest plot depicting HFNC compared to the comparator subgroups of NIV and conventional oxygen therapy on invasive mechanical ventilation rates across randomized trials and observational studies. No difference in rates of invasive mechanical ventilation were noted using a random effects model.
Predictors of High-Flow Nasal Cannula Failure
HFNC Compared to Oxygen Therapy for Acute Hypoxemic Respiratory Failure
Factors Associated With Mortality and Invasive Mechanical Ventilation
To further evaluate predictors of mortality and invasive mechanical ventilation, we evaluated any study that conducted multivariable logistic regression analysis to characterize variables associated with increased mortality or the need for ventilation. Five studies evaluated predictors of these outcomes (Table 4). Consistent predictors of mortality or invasive mechanical ventilation included age, severity of illness score and the use of NIV or non-HFNC oxygen therapy.
Discussion
This systematic review identified 13 studies evaluating the efficacy of HFNC in 1,956 immunocompromised subjects with AHRF. The evidence base to date includes 4 RCTs, 8 retrospective studies, and, most recently, the largest study to date, a prospective observational cohort study.21 Intubation and mortality rates were 46% and 36%, respectively. In our exploratory analysis, we found that mortality and invasive mechanical ventilation were decreased with the use of HFNC compared to any oxygen therapy control (ie, NIV or conventional O2 therapy). Across the oxygen therapy subgroups, HFNC was associated with a decreased mortality compared to NIV but not compared to conventional O2 therapy. No differences in invasive mechanical ventilation were seen in the subgroup analyses comparing HFNC to NIV or HFNC to conventional O2 therapy. Consistent predictors of mortality and invasive mechanical ventilation noted across 5 studies using multivariable logistic regression analysis were age, severity of illness, and NIV (or non-HFNC oxygen therapy).
This is the largest systematic review and meta-analysis to evaluate noninvasive strategies of oxygen support in the immunocompromised patient population. Our main objectives included highlighting the characteristics and evidence to date in this subset of subjects. Importantly, rates of intubation and mortality across this immunocompromised cohort have decreased compared to historic controls, highlighting the improved outcomes across immunocompromised subjects.1–5 However, the population was not homogeneous, with transplant subjects having lower rates of intubation and overall mortality compared to the oncologic and hematologic malignancy subjects. Given the higher mortality across this subset of subjects if they do progress to intubation, strategies to support them to prevent intubation remain important. This review highlights the need for higher-quality data dedicated to this particular population. Across this collected data, which was pooled for hypothesis generation, it suggests potential benefit of HFNC compared to any oxygen therapy control given the lower mortality and rates of invasive mechanical ventilation that we noted. Our results contrast with some of the findings from recently published systematic reviews comparing HFNC to conventional O2 therapy and NIV in 1,715 and 2,004 general medical/surgical subjects with AHRF, respectively.34,35 Neither analysis demonstrated a difference in the rates of invasive mechanical ventilation or mortality. A third, larger meta-analysis of > 3,000 subjects also demonstrated results discordant with our findings.13 Investigators found a reduced rate of invasive mechanical ventilation for HFNC compared to conventional O2 therapy but not NIV, and they found no mortality difference between modalities. The difference in findings from these recent reviews may be attributable to the different populations included in other meta-analyses and our study. A large RCT of > 800 post-cardiac surgery subjects comprised a significant proportion of each analysis.14 Post-cardiac surgery AHRF is vastly different from AHRF in the immunocompromised population for several reasons, including differences in etiology and severity of AHRF. Post-cardiac surgery, cardiogenic pulmonary edema, or atelectasis may be more common, which may benefit from positive pressure delivered via either HFNC or NIV. This could, in part, explain the absence of benefit of one modality over the other.
The benefit of HFNC compared to the pooled oxygen controls may be attributable to more effective alveolar oxygen delivery, PEEP generation, humidity-induced mucociliary clearance, or dead space washout. It is possible that the results are predominantly driven by the comparison between HFNC and NIV. It is theorized that NIV could be associated with harm. One possible explanation for the finding of benefit of HFNC compared to NIV but not noted with conventional O2 therapy could be the pressure levels generated with NIV compared to pressure transmitted via HFNC. During NIV, patients may generate tidal volumes that are above those considered lung-protective (> 8 mL/kg tidal volume based upon ideal body weight), and this mechanism was hypothesized as a potential contributing factor in the trial by Frat and colleagues.12,36 Injurious tidal volumes could be exacerbated in the setting of spontaneous breathing, thus facilitating further ventilator-induced lung injury.37–40 This, in turn, could worsen hypoxemia and generate conditions requiring invasive mechanical ventilation. It is possible that conventional O2 therapy may not precipitate lung injury in the same way as NIV. The survival benefit seen in the HFNC versus NIV analysis may further support the argument of injurious ventilation during NIV. In one study, tidal volumes 1 h after initiation of NIV were 11 mL/kg across those who died compared to 7.6 mL/kg across those who survived, and half of the subjects on NIV had a tidal volume of ≥ 9.5 mL/kg.28 Immunocompromised patients typically present to the ICU with higher illness severity and multiple organ dysfunction5 and are therefore at higher risk of ventilation-associated lung injury, potentially exacerbated by injurious tidal volumes during NIV. A further hypothesis could be that oxygen therapy control groups (NIV or conventional O2 therapy) may delay the identification of the etiology for respiratory failure due to the time needed to obtain computed tomography or fiberoptic imaging if indicated, leading to a higher risk of indeterminant cause of AHRF.21 Indeterminant causes of AHRF has been shown to be associated with increased mortality. Given the small numbers, it remains unclear whether there was a higher proportion of unknown causes of AHRF in the oxygen therapy controls compared to the HFNC group. Additionally, the oxygen therapy control groups, especially NIV, could lead to an interruption in important ICU interventions such as feeding and mobilization, which may be particularly important in the immunocompromised population.
Strengths of our review include that this is the largest study to evaluate the evidence to date in this subset of subjects and to explore the potential differential impact of noninvasive oxygenation strategies on a unique critically ill population. This review, however, has several limitations. First, there was a small number of high-quality studies included in the meta-analysis, which increases the risk of bias. We included the totality of the literature (ie, RCTs and observational studies) in an attempt to utilize important subgroups or post hoc analyses to conduct our exploratory analysis. Given this expected limitation, we also conducted a series of sensitivity analyses of the “higher-quality” studies (ie, RCTs and observational studies with matching) and evaluated the results of multivariate analyses across the subset of studies, adjusting for confounders. These analyses demonstrated similar results compared to our primary analysis. Second, heterogeneity exists with respect to the underlying immunocompromised population (eg, oncology and transplant), definitions of AHRF, indication for therapy, duration of therapy, administration of noninvasive oxygen strategies, and criteria for intubation. However, despite these differences, the signal of effect was similar across most studies. Third, various modalities of NIV currently exist; however, no study reported on the use of face-tent oxygen delivery or more restrictive tidal volume compared to the modalities explored.41 These limitations and the results of this review support the need for larger studies with homogenous inclusion criteria. The results of this systematic review are meant to be hypothesis-generating and to highlight the characteristics across this population of AHRF. Future study will necessitate larger RCTs specifically enrolling immunocompromised subjects to compare conventional O2 therapy, NIV, and HFNC head to head.
Conclusion
HFNC is a unique oxygen-delivery modality that holds theoretical promise for the treatment of AHRF in immunocompromised patients. However, the current body of literature demonstrates that there is a paucity of high-quality data in this specific population to guide evidence-based therapy. In our exploratory analysis, the data suggest that HFNC may prevent mortality and invasive mechanical ventilation in selected settings; however, this remains a hypothesis that needs to be further evaluated with higher-quality data dedicated to this population. This analysis strongly states the need for further research with clinical and physiological studies, including larger RCTs specifically enrolling immunocompromised subjects to more clearly elucidate the benefit of HFNC in this population.
Footnotes
- Correspondence: Laveena Munshi MD MSc, Interdepartmental Division of Critical Care Medicine, Mount Sinai Hospital, Sinai Health System, University of Toronto, 600 University Ave, Toronto, ON M5G 1X5, Canada. E-mail: laveena.munshi{at}sinaihealthsystem.ca.
The authors have disclosed no conflicts of interest.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2018 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}