

Abstract
BACKGROUND: Heated and humidified high-flow nasal cannula (HFNC) is a widely used form of respiratory support; however, data regarding optimal flows for a given patient size or disease state are lacking. A comprehensive study of the physiologic effects of HFNC is needed to better understand the mechanisms of action. The objective of the current study was to quantify the effect of HFNC settings in age-specific, anatomically correct nasal airways and spontaneously breathing lung models. We hypothesized that there is an effect of flow on pressure and ventilation.
METHODS: Three-dimensionally printed upper airway models of a preterm neonate, term neonate, toddler, small child, and adult were affixed to the ASL 5000 test lung to simulate spontaneous breathing with age-appropriate normal ventilation parameters. CO2 was introduced to simulate profound hypercapneic respiratory failure with an end-tidal partial pressure of carbon dioxide (PETCO2) of 90 ± 1 mm Hg. Two commercially available HFNC systems were applied to the airway models, and PEEP, inspired CO2, and exhaled CO2 (PETCO2) were recorded for 6 min across a range of flow.
RESULTS: Increasing HFNC flow provided a non-linear increase in PEEP in closed-mouth models, with maximum tested flows generating 6 cm H2O in the preterm neonate to 20 cm H2O in the small child. Importantly, PEEP decreased by approximately 50% in open-mouth models. Increasing HFNC flow improved expiratory CO2 elimination to a certain point, above which continued increases in flow had minimal additional effect. This change point ranged from 4 L/min in the preterm neonate to 10 L/min in the small child.
CONCLUSIONS: These findings may help clinicians understand the effects of HFNC at different settings and may inform management guidelines for patients with respiratory failure.
Introduction
Heated and humidified high-flow nasal cannula (HFNC) was initially proposed as an alternative to CPAP for premature neonates.1 HFNC use has rapidly expanded to patients with respiratory insufficiency, including infants with bronchiolitis2 and adults with COPD3 and ARDS.4,5 Clinical studies suggest that HFNC effectively supports some patients who would have otherwise been treated with CPAP and noninvasive ventilation.5–7 However, there is a lack of experimental evidence to support widespread clinical implementation of HFNC.
HFNC may improve oxygen delivery when flow exceeds peak inspiratory flow, thereby reducing air entrainment.8 Multiple studies suggest HFNC generates PEEP, improving alveolar recruitment and reducing airway obstruction.9–12 HFNC may also reduce minute ventilation demand by overcoming increased airway resistance13 and flushing extrathoracic dead space, thereby reducing rebreathed exhaled CO210,14,15 It is unclear which settings constitute HFNC therapy, and there is not consensus on initial flow for a given patient size, weaning, or indications for other forms of respiratory support. A comprehensive study of the physiologic effects of HFNC is needed to inform clinical management strategies and design future studies to better understand the mechanisms of action of HFNC.
The objective of the current study was to quantify the effect of HFNC settings in age-specific, anatomically correct nasal airways and spontaneously breathing lung models. We hypothesized that there is an effect of flow on pressure and ventilation.
QUICK LOOK
Current knowledge
High-flow nasal cannula (HFNC) is increasingly being used as an intermediary form of noninvasive support. Studies have shown that HFNC may improve oxygenation and ventilation and reduce work of breathing, breathing frequency, and the need for intubation. The precise mechanisms by which physiologic parameters are improved with HFNC are unknown, but may be related to increases in PEEP and CO2 elimination from the anatomic nasopharyngeal airways. Currently, there is no consensus on initial flow for a given patient size, weaning, or indications for other forms of respiratory support.
What this paper contributes to our knowledge
These data show direct associations between HFNC flow, PEEP, and ventilation across a range of patient ages. PEEP increased with flow and varied between open- and closed-mouth conditions and the models. Reductions in inspired CO2 levels suggest that purging CO2 from the anatomic dead space is a major contributing factor for improved ventilation in preterm models, whereas disproportionate decreases in inspired CO2 relative to expiratory CO2 imply that CO2 flushing may occur during inhalation and exhalation in all models. The effect of HFNC flow on PEEP and ventilation observed in this study suggests that HFNC support may approximate other forms of noninvasive support.
Methods
Nasal Airway and Lung Models
Upper-airway models were constructed using 3-dimensional rapid prototyping devices from CT scans of the upper airways of a preterm neonate (28 weeks, 1 kg), term neonate (38 weeks, 4 kg), toddler (17 months, 10 kg), small child (5 y, 20 kg), and adult (17 y, 70 kg).16–18 Preterm and small child models had established oral airway openings, so open-mouth and closed-mouth conditions were simulated in these models. Term-neonate, toddler, and adult models did not have oral airway openings, so only closed-mouth conditions were simulated. Adapter, tubing, and pneumotachometer size were adjusted (quantified with water) to approximate previously published age-specific extrathoracic dead space values19 in all models except the preterm due to the minimum fixed volume of CO2 and pressure adaptors (Table 1).
Lung Model Configuration, Instrumental Dead Space, Cannula Sizes, and Flows
Models were attached to the ASL 5000 Test Lung (Ingmar Medical, Pittsburgh, Pennsylvania) in series with a CO2 injection adapter, CO2 analyzer adapter, and pneumotachometer (Fig. 1). Spontaneous breathing was simulated using age-specific normal values.17,20–24 The inspiratory-to-expiratory ratio was held constant at 1:3, and inspiratory effort was adjusted to maintain constant tidal volume (6 mL/kg) in each model at different HFNC flows. A CO2 injection port adapter with integrated unidirectional catheter was placed 5 mm within the lung model to preferentially direct CO2 flow to the lung compartment using a CO2 flow meter (Cole-Palmer, Vernon Hills, Illinois). CO2 was measured with a calibrated mainstream CO2 sensor (CO2SMO, Philips Respironics, Murrysville, Pennsylvania).

Experimental setup. Studies were conducted using 5 different 3-dimensional anatomic airway models attached to a spontaneously breathing lung model configured with normal lung mechanics values for each simulated model. The airway model shown is the toddler version. Continuous analogue data were acquired from the individual monitors and lung model, converted with an analogue/digital (A/D) converter, and displayed on a computer monitor (not shown).
HFNC Systems and Prongs
Infant and Pediatric Optiflow Junior and Adult Optiflow (Fisher & Paykel Healthcare, Auckland, New Zealand) and Precision Flow (Vapotherm, Exeter, New Hampshire) HFNC systems were used. Flows were confirmed using a calibrated gas flow analyzer (PF-350, ImtMedical, Buchs, Switzerland) before testing each condition. The HFNC systems were preset at 37°C and FIO2 1.0. Age-specific flow ranges were chosen based on flows from previously published studies5,25 and manufacturer recommendations. HFNC cannula sizing was based on manufacturer recommendations. The prongs were secured in the models' nares to achieve approximately 50% occlusion (Table 1). The Optiflow HFNC system was set up with an Optiflow Junior heated-wire corrugated breathing circuit (RT329 8-mm outer diameter; pressure relief valve ∼40 cm H2O) for infant and toddler models and an adult noninvasive heated-wire corrugated circuit (RT319; 22-mm outer diameter) for small child and adult testing. Both circuits were attached to an MR850 heated humidifier and respective Optiflow or Optiflow Junior cannulae. A standard air/oxygen blender (Bird High Flow, BD Medical, Yorba Linda, California) and an attached oxygen flow rotameter (Cole-Palmer, Vernon Hills, Illinois) were used to adjust flow.
The Precision Flow HFNC system incorporates a standalone user interface module that houses the vapor transfer cartridge, oxygen analyzer, blender, and electronic mass flow sensor. Flow, temperature, and FIO2 are adjusted independently, and parameters are digitally displayed on the module. The patient circuit incorporates heated water and gas pathways within a smooth-bore patient circuit. A low-flow or high-flow vapor cartridge was used when testing HFNC flows of 1–8 and 5–40 L/min, respectively. In some cases, vapor cartridge sizing was based on the manufacturer's suggested size per the different cannula sizes.
The resolution of flow measurement with the Precision Flow was 0.5 and 1.0 L/min with the high- and low-flow cartridges, respectively. Since the measured flows with the Precision Flow appeared to vary from the preset flow setting on the device, the analog flow meter with the Optiflow was adjusted to match the flow output of the Precision Flow system and confirmed with both systems using a calibrated unidirectional gas flow analyzer before testing at each flow condition.
Experimental Procedures/Data Acquisition
Each experiment was performed by first random selection of the model, followed by randomized selection of the HFNC system, and then the flow settings were tested in random order. Data were collected in triplicate on 3 separate days for each model and system. Continuous analog output of inspiratory CO2, expiratory CO2, and PEEP were collected from the CO2SMOplus monitor and ASL 500 lung model, respectively, and processed using an analog-to-digital converter (ADInstruments, Colorado Springs, Colorado). Tracheal flow was measured using a calibrated heated pneumotachometer head (Hans Rudolph, Shawnee, Kansas) and acquired using a PowerLab Spirometer Pod (ADInstruments). All data were displayed and recorded digitally with LabChart 5.5.6 data analysis software (ADInstruments).
CO2 flow into the lung was adjusted to simulate profound hypercapneic respiratory failure with an end-tidal partial pressure of carbon dioxide (PETCO2) of 90 ± 1 mm Hg. Data were inspected in real time, and steady state was determined visually from streaming data. Pressure and ventilation measurements were collected for 1 min before and 6 min after cannula placement. Immediately following cannula placement, ASL lung model muscle pressures were adjusted to maintain targeted tidal volumes (Table 1).
Data Analysis
Inspiratory CO2 was determined as the measured CO2 at peak inspiratory flow, whereas expiratory CO2 (also known as PETCO2) and PEEP were measured at zero flow at end expiration. Inspiratory CO2 values represented exhaled CO2 that was rebreathed from the airway model (dead space), whereas expiratory CO2 values represented simulated alveolar CO2 from the lung model. Baseline and response variables for each signal were determined by the arithmetic means of measurements acquired during the 1 min preceding and 5th minute following cannula placement, respectively. Data were analyzed using random-intercept linear mixed-effects models; segmented linear mixed-effects models with fixed effects for both the change point and the slope differences before and after the change point were used when data indicated a nonlinear relationship between flow and signal. All data were analyzed in R (v.3.4.1, R Foundation for Statistical Computing, Vienna, Austria).26,27 Piece-wise linear dependence was observed between PEEP and flow, so segmented random-intercept linear mixed-effects models were fitted with fixed effects for both the change point and the slope differences before and after the change point. PEEP data were right-skewed, so the analysis was performed on the log scale. Model results are reported as the estimated change point and the mean percentage increase with 95% CIs for each unit increase in flow below and above the change point.
All analyses were done separately for each model. First, PETCO2 and inspired CO2 at the minimum tested flow were compared with baseline using summary statistics and linear mixed-effects models with a random intercept for the experimental day. Model results are reported as mean difference ± SE of the difference between the 2 flows. Separate analyses were performed for positive flows. There, signal variations were modeled as a function of flow using random-intercept linear mixed-effects models. Where piece-wise linear dependence was observed, segmented random-intercept linear mixed-effects models were fitted with fixed effects for both the change point and the slope differences before and after the change point. In segmented linear mixed-effects models, change points were estimated iteratively and simultaneously with other parameters. Residual analyses were performed using summary and graphical statistics. Model results are reported as the mean change in response for a 1-L/min increase in flow below and above the change point.
Results
There was a nonlinear increase in PEEP as a function of HFNC flow in all models (Fig. 2). The rate of increase was greater at flows below the change point than above the change point in all models except for the preterm open-mouth model (Table 2). The change point increased with age from 4 L/min in the preterm and term neonates to 10 L/min in the toddler and small child to 22 L/min in the adult (Table 2). The flow required to generate a PEEP of 6 cm H2O also increased with age: preterm neonate, 8 L/min; term neonate, 5–7 L/min; toddler, 14–20 L/min; small child, 12–20 L/min; adult, 24–36 L/min. The Precision Flow system generated higher PEEPs than the Optiflow system in the term neonate, toddler, and small child models (Fig. 2 and Table 2).

Lung model end-expiratory pressure or PEEP representing simulated alveolar pressure at baseline (no high-flow nasal cannula) and pressure at different flows provided with the Optiflow and Precision Flow high-flow nasal cannula systems. Individual data points are shown for each measurement of pressure, fitted with locally weighted scatterplot smoothing curves. Gray vertical lines represent the change point where a nonlinear relationship between flow and pressure is observed.
PEEP at Increasing High-Flow Nasal Cannula Flow
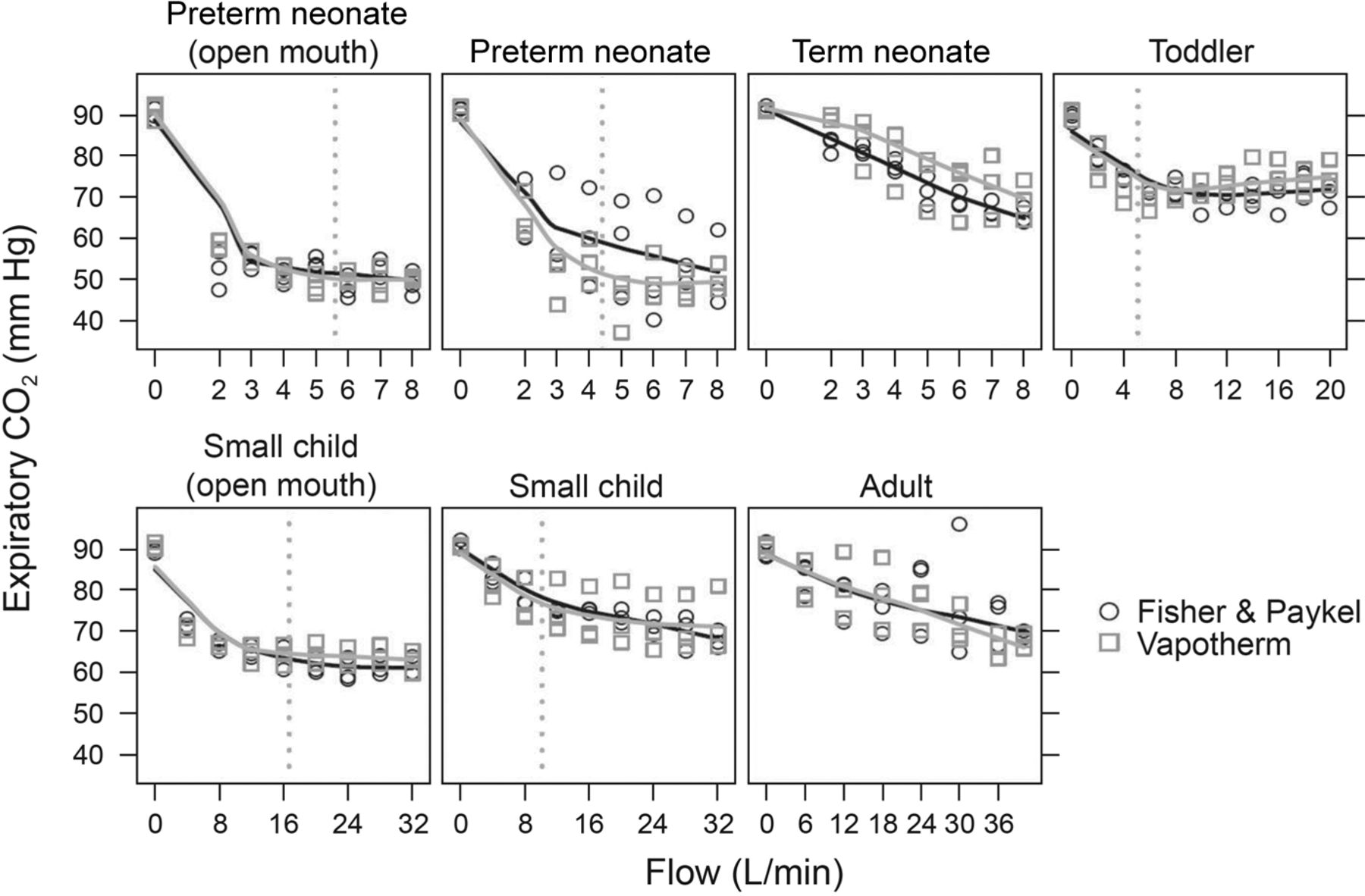
Expiratory CO2 clearance increased from baseline at the minimum tested flow in all models (Table 3). The relationships between expiratory CO2 and flow were linear in the term-neonate and adult models and approximately piece-wise linear in all other models (Fig. 3). The estimated change point for CO2 clearance increased with age. The average decrease in expiratory CO2 per 1-L/min increase in flow was greatest between baseline and the minimum tested flow. There was no difference in expiratory CO2 clearance between HFNC systems across all testing conditions (Table 3).
Expiratory CO2 Change at Minimum and Increasing High-Flow Nasal Cannula Flows
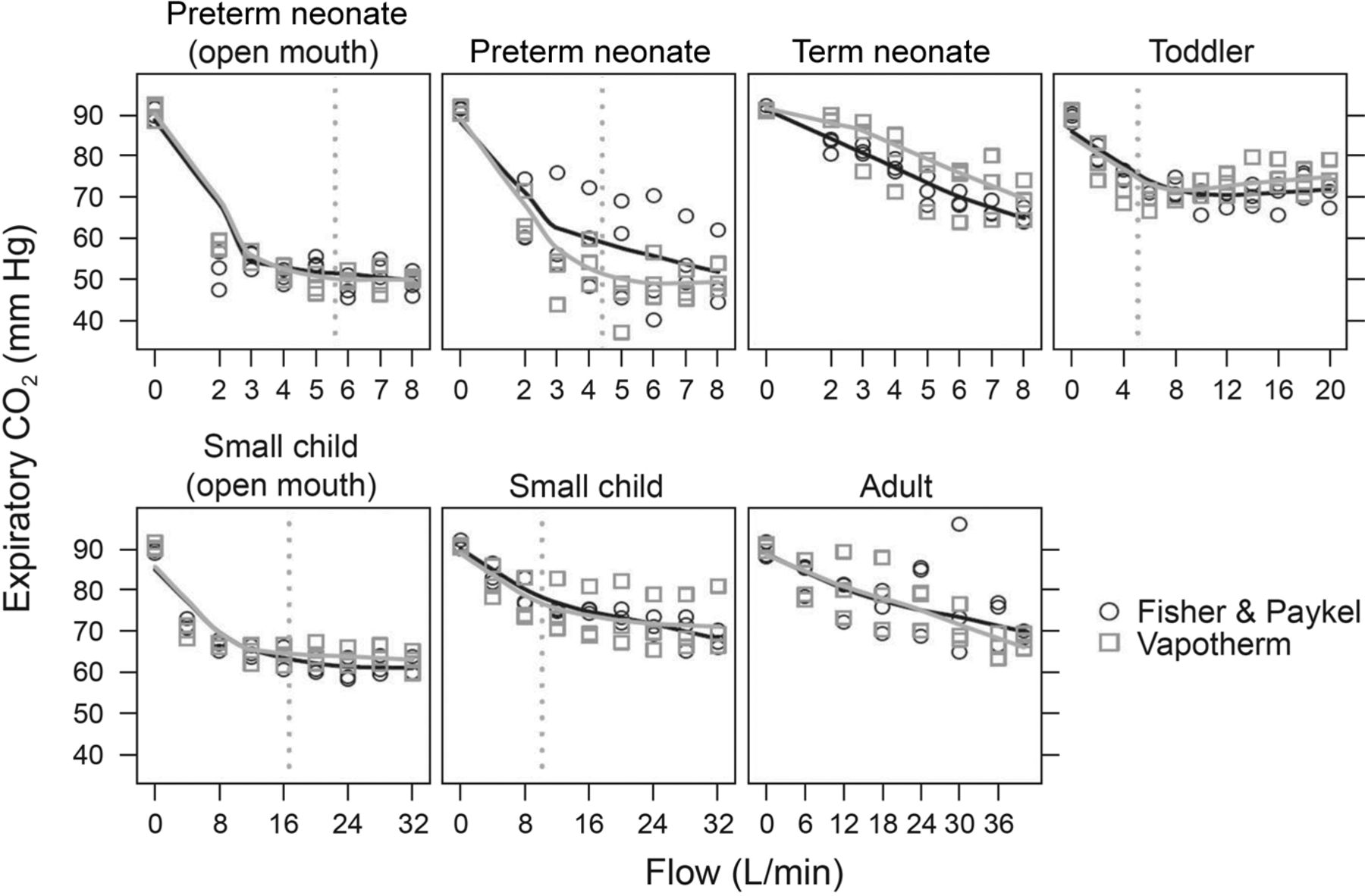
Lung model expiratory CO2 (or PETOv2) representing simulated alveolar CO2 at baseline (no high-flow nasal cannula) and effect on expiratory CO2 at different flows provided with the Optiflow and Precision Flow high-flow nasal cannula systems. Individual data points are shown for each measurement of CO2, fitted with locally weighted scatterplot smoothing curves. Gray vertical lines represent the change point where a nonlinear relationship between flow and expiratory CO2 was observed. There was no change point observed in expiratory CO2 in adult and term newborn models.
Inspiratory CO2 decreased as HFNC flow increased, but the magnitude was less than that observed with expiratory CO2 (Fig. 4). The greatest absolute decrease in inspiratory CO2 per 1-L/min increase in flow was in the preterm neonate between baseline and the minimum tested flow (Table 4). Non-linear relationships between flow and inspiratory CO2 were observed in the preterm neonate, term neonate, and toddler models, with a change point of 5 L/min. There was minimal to no clinically relevant change in inspiratory CO2 in the adult and small-child models. There was no difference in inspiratory CO2 clearance between HFNC systems (Table 4).
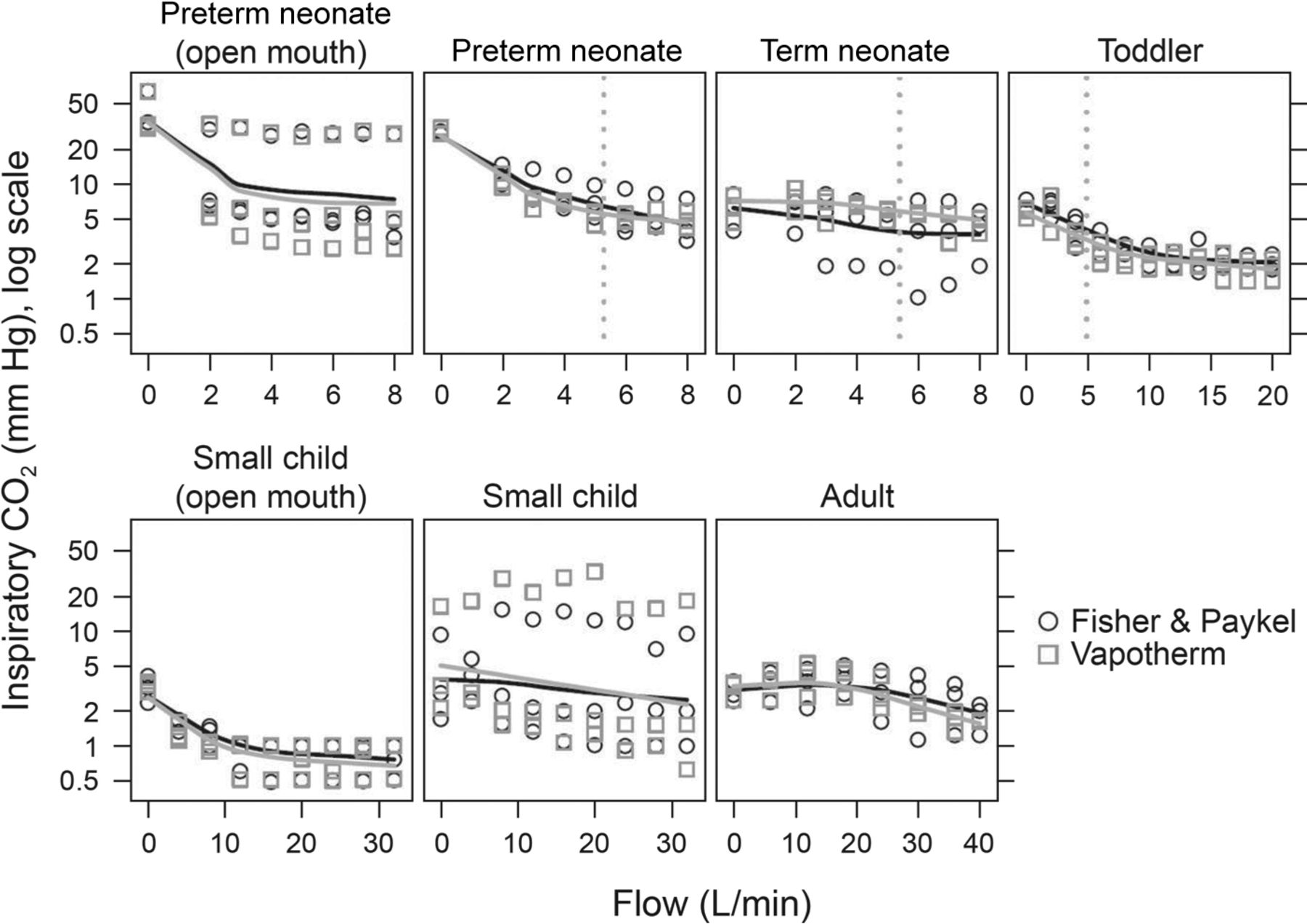
Lung model inspiratory CO2 representing simulated inspired CO2 from the anatomic airway dead space at baseline (no high-flow nasal cannula) and effect on inspired CO2 at different flows provided with the Optiflow and Precision Flow HFNC systems. Individual data points are shown for each measurement of CO2, fitted with locally weighted scatterplot smoothing curves. Grey vertical lines represent the change point where a nonlinear relationship between flow and inspiratory CO2 was observed. The change point was present only in preterm and term newborn and toddler closed-mouth models.
Inspiratory CO2 Change at Minimum and Increasing High-Flow Nasal Cannula Flows
An oral leak decreased the PEEP response to flow by approximately 50% at the maximum tested flow (Fig. 2). In open-mouth models, both the decrease in expiratory CO2 at minimum tested flow from baseline and the change point estimate were larger than in the corresponding closed-mouth models (Fig. 3 and Table 3). The magnitude of decrease in inspiratory CO2 at minimum tested flow was larger in open-mouth versus closed-mouth models (Fig. 4 and Table 4).
Discussion
These are the first data using realistic airway and lung models to show associations between HFNC flow, PEEP, and ventilation across a range of patient ages. Our major finding is that HFNC provided PEEP similar to those used with CPAP, but only at certain flows in closed-mouth models. Increasing HFNC flow improved CO2 elimination, but only to a certain point, above which continued increases in flow had no additional effect. These findings may help clinicians define optimal HFNC settings, inform management guidelines, and help in designing future studies for pediatric patients with respiratory failure.
A recent meta-analysis showed similar rates of survival and bronchopulmonary dysplasia in premature infants supported with nasal CPAP and HFNC,1 which may be related to similarities in effective PEEP. One study showed that HFNC increased both PEEP and end-expiratory lung volume, providing evidence that HFNC can recruit collapsed alveoli.28 The PEEPs observed in our models correlate well with those reported in infants1,28,29 and adults,11,30–32 with the exception of 2 studies using adult nasopharyngeal models9,33 that we attribute to model differences. Thus, the current study contributes to the growing body of evidence that HFNC generates PEEP.
With HFNC's nonocclusive interface, it is essential to consider the effect of an open mouth, as pressure decreases with an oral leak.34 We observed a 50% decrease in PEEP with an open mouth. Luo et al9 recently reported nearly absent PEEP in their open-mouth model, suggesting that strategies to close the mouth may benefit patients with disease processes requiring higher PEEP. However, our data also suggest that PEEP rapidly rises to >10 cm H2O in the small child treated with ≥20 L/min with a closed mouth. As such, clinicians must recognize the high level and potentially injurious support that can be administered by HFNC when the patient's mouth is closed. Although these findings differ from one study in premature infants,1 open-mouth pressures in our preterm neonate model approximate distending pressures observed in premature infants receiving HFNC and nasal CPAP, 6 cm H2O.35 Two adult studies30,31 and one lung and airway model study9 also support our results, reporting a substantial loss of pressure with an oral leak.
Another notable finding was the difference in PEEP generated by the 2 HFNC systems. The higher PEEP with the Precision Flow system is consistent with a previous neonatal bench study.34 These differences could be related to the integrated pressure-relief valve in the Optiflow system, which has been shown to vent flow to the atmosphere.36 Importantly, the previous studies used first generation Optiflow HFNC prongs rather than the Optiflow Junior. Although the current Optiflow HFNC system still incorporates the pressure-relief valve, the Optiflow Junior cannula's decreased resistance reduces venting of flow to the atmosphere. Another possible explanation for PEEP differences could be increased nasal airway occlusion with the Precision Flow cannulae. This could explain differences in the term neonate; however, the Precision Flow cannula was less occlusive in the toddler and small child models in which greater PEEP was generated at maximum flows. An additional explanation could be differences in prong design, tubing diameter, and relative resistance within the systems. Optiflow cannulae have independent flow channels to each prong and wider bore tubing, whereas the Precision Flow cannulae have a common flow channel and narrower tubing. Three-dimensional computational fluid dynamic models have shown that smaller bore cannulae may produce a higher flow velocity,37 and we speculate that a similar phenomenon occurs with the Precision Flow cannulae.
Improved CO2 clearance with HFNC helps explain reported clinical reductions in breathing frequency, arterial CO2, and work of breathing in patients treated with HFNC.38 One study using tracer gases demonstrated improved CO2 clearance when HFNC flows exceeded peak expiratory flow.39 The decrease in expiratory CO2 appears to be due, in part, to an immediate reduction in inspired CO2, which was also observed in a tracheotomized adult supported with HFNC.40 Similar to prior reports,10,31,41 CO2 clearance was more pronounced with an oral leak. These data and previous studies suggest that flushing anatomic dead space with fresh gas is an important mechanism by which HFNC reduces minute ventilation demands. Our results suggest age-dependent differences in the effect of flow on minute ventilation that are explained by the reduction in dead space fraction (VD/VT) with increasing age.
The disproportionate decrease in inspired CO2 relative to expiratory CO2 implies that CO2 flushing may occur during inhalation and exhalation. This combined inspiratory/expiratory purging effect may be more pronounced with flows exceeding peak inspiratory flow, which could explain the observed change point in exhaled CO2 clearance. Assuming an extrathoracic volume of 9 mL, tidal volume of 6 mL, and inspiratory time of 0.28 s, the calculated peak inspiratory flow of 3.2 L/min approximates the observed change point in our preterm neonate model, implying that higher flows allow CO2 clearance around the nasal cannula during inspiration. Since the adult model showed minimal decrease in inhaled CO2, we assume that linear reductions in exhaled CO2 are related more to flushing during inhalation than exhalation.
Although this study simulated patients in hypercapneic respiratory failure, there are limitations. The anatomic models are based on CT images but lack the mucosal layer and upper-airway elasticity that may affect pressure and airway resistance. The test lung model is unable to simulate atelectasis; hence, generation of PEEP does not recruit alveoli, decreases physiologic dead space and improves ventilation-perfusion matching. Thus, reductions in expiratory CO2 can only be attributable to effects on anatomic dead space. We also used age-appropriate normal lung mechanics rather than a pathophysiologic state in which HFNC would be used, making it challenging to extrapolate our results to clinical use. One of the greatest shortcomings was the variation in cannula placement, resulting in increased variability in measurements. Although markers were used to improve consistency, placing a cannula in the exact position every run proved challenging. However, this probably represents real-world conditions in which cannula position changes with patient positional changes.
We originally intended to completely randomize data collection for each model, HFNC system, and flow to minimize variability due to experimental conditions on a particular day. However, the time required to set up each model and HFNC system made this design impractical. Hence, we opted for randomizing flows within each experimental day. With this design, we observed a systematic bias in ventilation variables associated with the day of collection in some models. Given the employed randomization scheme, a linear mixed-effect model with a random intercept was used to account for the effect of the acquisition day.
Conclusions
Despite these limitations, the observed associations between HFNC flow, PEEP, and ventilation across a wide range of patient sizes contribute to improved understanding of the effects of HFNC. The effect of HFNC flow on PEEP and ventilation observed in this study suggests that HFNC support may approximate other forms of noninvasive support. Studies in infants42 and adults43 have shown that HFNC is potentially as effective as noninvasive ventilation in preventing invasive ventilation, so its use may result in decreased morbidity associated with invasive ventilation. Although our findings may serve as a guide for clinicians using HFNC, clinical studies to delineate HFNC effects in children and adults are necessary to determine whether these findings hold true.
Footnotes
- Correspondence: Robert M DiBlasi RRT-NPS FAARC, Seattle Children's Research Institute, 1900 Ninth Ave North, Seattle, WA 98101. E-mail: robert.diblasi{at}seattlechildrens.org.
Mr DiBlasi has disclosed relationships with Draeger, Mallinckrodt, United Therapeutics, and Aerogen. The other authors have disclosed no conflicts of interest.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2018 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}
{kind=link}