

Abstract
BACKGROUND: The objective of this work was to identify the unique characteristics of patients who experienced success in a 30-min spontaneous breathing trial (SBT) but failed at 120 min.
METHODS: Patients who had received mechanical ventilation for >24 h were eligible for inclusion in this study. The SBT was performed by 7 cm H2O of pressure support with zero PEEP. After a successful 120-min SBT, weaning from mechanical ventilation was performed. Data were collected at 30 and 120 min or at the failure of the SBT. All patients who successfully completed a 30-min SBT were enrolled.
RESULTS: We enrolled 352 subjects in this study. Of these, 311 subjects (88.4%) directly completed a 120-min SBT (success group), and 41 subjects (11.6%) passed the test for at least 30 min but failed before 120 min (failure group). In data collected before the SBT, presence of chronic cardiopulmonary disease, number of previous SBT attempts before 30-min SBT success, age, and PaCO2 were independently associated with 120-min SBT failure. A scale was developed that used these 4 variables. The failure rate was low in subjects with ≤2 points (3%) but significantly higher in subjects with >2 points (46%). In data collected at the 30-min SBT, PaCO2, rapid shallow breathing index, ΔPaO2/FIO2, Δbreathing frequency, and ΔpH were independently associated with 120-min SBT failure. These 5 variables were then used to develop another scale to predict SBT success. Similar to the previous score, the failure rate was low in subjects with ≤2 points (1%) and significantly higher in subjects with >2 points (55%).
CONCLUSIONS: This study highlights differences between subjects who completed a 120-min SBT and those who succeeded at 30 min but failed by 120 min. In subjects with a score >2 points, reflecting a greater risk of SBT failure, a 120-min SBT may be required.
Introduction
Mechanical ventilation is a life-saving tool for critically ill patients, but it is also associated with many complications, such as ventilator-associated pneumonia and ventilator-associated lung injury.1,2 Therefore, it is important to wean patients from mechanical ventilation as soon as possible if the respiratory failure that necessitated ventilation has been reversed and the patient is able to sustain spontaneous breathing. However, premature disconnection from mechanical ventilation has been shown to result in a high risk of re-intubation, and delaying extubation also unnecessarily extends the duration of mechanical ventilation and increases the risk of ventilator-associated pneumonia.3,4 Therefore, it is necessary to know whether a patient will be able to successfully liberate from mechanical ventilation.
A spontaneous breathing trial (SBT) has been recommended to judge a patient's ability to spontaneously breathe without assistance.5,6 Previous studies have reported that outcomes did not differ between subjects who passed a 30- or a 120-min SBT.7,8 However, Esteban et al7 observed SBT failure rates of 12.2% in a 30-min SBT and 15.6% in a 120-min SBT. In addition, Perren et al8 reported SBT failure rates of 6.5% in a 30-min SBT and 11.5% in a 120-min SBT. These findings indicate that some patients who successfully complete a 30-min SBT may nevertheless fail a 120-min SBT. To the best of our knowledge, no study has yet reported on subjects who experienced success with a 30-min SBT but failure with a 120-min SBT. Thus, we aimed to identify the clinical characteristics of subjects who passed a 30-min SBT but went on to fail a 120-min SBT.
QUICK LOOK
Current knowledge
The recommended duration of a spontaneous breathing trial (SBT) has been between 30 and 120 min. However, some patients have a successful 30-min SBT but fail at 120 min. The clinical characteristics differentiating these groups are unclear.
What this paper contributes to our knowledge
This study, using a pressure support level of 7 cm H2O, found that the presence of chronic cardiopulmonary disease, SBT attempts before 30-min SBT success, age, PaCO2, rapid shallow breathing index, ΔPaO2/FIO2 (subtracting the value collected at the beginning of the SBT from the value collected at 30 min; T30-T0), Δbreathing frequency (T30-T0), and ΔpH (T30-T0) were predictors of 30-min SBT success but 120-min failure. The failure rate increased with an increased risk score. In patients with risk score >2 points, 120-min SBT may be required.
Methods
This study was prospectively performed in the ICU of a teaching hospital between March 2016 and April 2017, and the investigational review board approved the study protocol. Before enrollment, all patients or next of kin provided informed consent. All patients who had been receiving mechanical ventilation for >24 h were potential cases for this study. If they passed at least a 30-min SBT, we enrolled them in this study. Patients with a tracheotomy or <18 y of age were excluded from participation.
Subjects were managed according to the guidelines recommended by the Society of Critical Care Medicine of China.6 Orotracheal intubation was the first choice to build an artificial airway. However, in patients with difficult orotracheal intubation, nasotracheal intubation was instead performed with guidance from a bronchofibroscope. The cuff pressure of the endotracheal tube was maintained at 25–30 cm H2O to prevent mucosal injury, and it was measured every 8 h. Active humidification was performed in all subjects, and the temperature was maintained at 37°C. The circuit of the ventilator was changed every 7 d. However, if the circuit was visibly soiled or if it malfunctioned, it was changed immediately. Tidal volume was maintained at 8 mL/kg of predicted body weight in subjects without ARDS and at 6 mL/kg of predicted body weight in subjects with ARDS. Sedation was performed to reduce the work of breathing or reach optimal patient-ventilator interaction. Typically, the sedation was titrated to maintain a breathing frequency of <30 breaths/min and a Richmond Agitation-Sedation Scale of +1 to −2.
We used pressure support ventilation to wean subjects from mechanical ventilation. Every morning, the respiratory therapists screened the subjects to identify those who were eligible for an SBT. The criteria for SBT were as follows: sufficient improvement of the underlying causes that required mechanical ventilation, PaO2/FIO2 >150–200mm Hg, PEEP <5–8 cm H2O, FIO2 ≤0.5, stable hemodynamics, body temperature <38.5°C, and subject wakefulness (without continuous sedation). The 120-min SBT was performed with low-pressure support (7 cm H2O) with no PEEP and the same level of FIO2 used during mechanical ventilation. Failure of an SBT was defined if the following occurred: breathing frequency >35 breaths/min, rapid shallow breathing index (f/tidal volume) >105, heart rate >140 beats/min, systolic blood pressure >180 or <90 mm Hg, PaO2 <60 mm Hg or PaO2/FIO2 <150 mm Hg, presence of acute hypoventilation and an increase of PaCO2 by at least 10 mm Hg, and presence of labored breathing resembling that seen during vigorous activity (eg, contraction of accessory muscles or a paradoxical abdominal breathing pattern). If the SBT failed, mechanical ventilation was reinstituted according to previous parameters, and weaning screening was repeated the next day. If the 120-min SBT was successfully completed, the endotracheal tube was removed.
Vital signs and arterial blood gas tests were collected at initiation, after 30 min of SBT, and at failure or after 120 min of SBT. Subjects who experienced success for at least 30 min but failed before reaching 120 min were placed into the failure group, and those who directly passed the 120-min SBT were placed into the success group.
Statistical Analysis
Data were reported as mean values and SD, median values and interquartile ranges, or numbers and percentages when appropriate. The differences between groups were analyzed using statistical software (SPSS 20.0, SPSS, Chicago, Illinois). For continuous variables, the difference between 30 min of SBT and initiation of SBT (T30-T0) was calculated by subtracting the value collected at the beginning of the SBT from the value collected at 30 min. To identify independent risk factors associated with 120-min SBT failure, variables with P < .20 in the univariate analysis were entered into a multivariable logistic regression model. A score was developed according to the weight (β regression coefficient) of each variable.9 P < .05 was considered to indicate a significant difference.
Results
A total of 352 subjects successfully completed a 30-min SBT and were enrolled in this study. Of these, 41 subjects (11.6%) had failed by 120 min (failure group), and 311 subjects successfully completed the 120-min SBT (success group). Compared with the success group, subjects in the failure group were older, had longer duration of mechanical ventilation before the first SBT attempt, and had made more SBT attempts before successfully completing a 30-min SBT (Table 1).
Demographics at enrollment
Just before the SBT, subjects in the failure group had a higher heart rate and higher PaCO2 than those in the success group (Table 2). After 30 min of the SBT, they also had a higher heart rate, a higher breathing frequency, a higher rapid shallow breathing index, and higher PaCO2. In addition, greater changes were seen in vital signs and arterial blood gas tests between the beginning of the SBT and 30 min.
Comparisons Between Groups
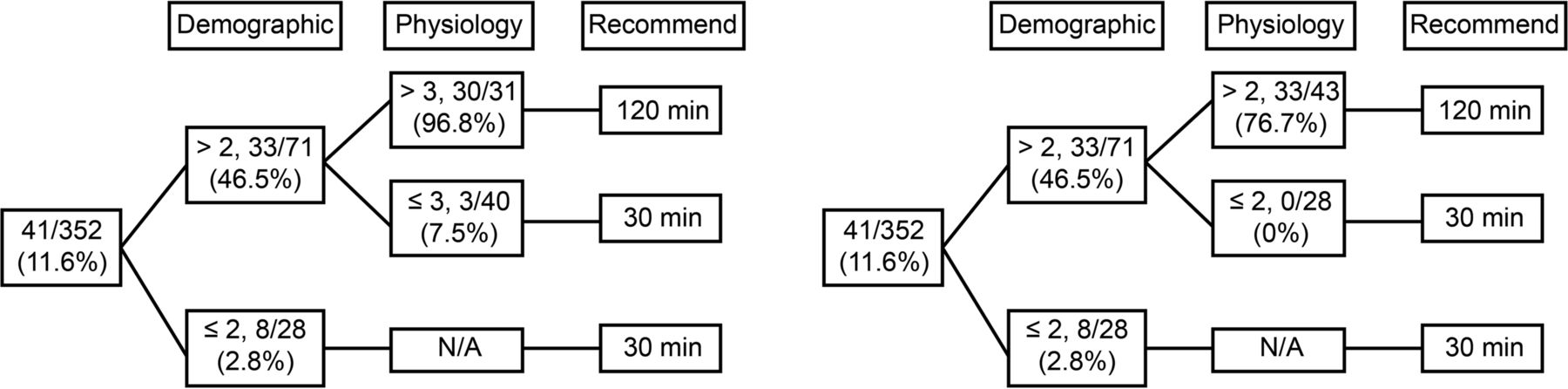
Before performance of an SBT, the presence of chronic cardiopulmonary disease, the number of SBT attempts before 30-min SBT success, age, and PaCO2 were independently associated with 120-min SBT failure (Table 3). The cutoff values, sensitivity, and specificity are summarized in Table 4. Points were assigned to each variable according to the β regression coefficient to create a risk scale. The failure rates were 2, 7, 0, 33, 36, and 100% in subjects with 0, 1, 2, 3, 4, and ≥5 points, respectively (Fig. 1). In data collected at 30 min, PaCO2, rapid shallow breathing index, ΔPaO2/FIO2 (T30-T0), Δbreathing frequency (T30-T0), and ΔpH (T30-T0) were independently associated with 120-min SBT failure. Finally, another scale was developed using the weight of each variable. Failure rates were 0, 0, 7, 16, 33, 75, and 100% in subjects with 0, 1, 2, 3, 4, 5, and ≥6 points, respectively. The power of this scale to predict 120-min SBT failure is summarized in Figure 2. A decision tree was developed in Figure 3 to show whether to prolong the SBT to 120 min.
Multivariable Logistic Regression Analysis Identifying Independent Risk Factors for 30-Minute SBT Success but 120-Minute Failure
Sensitivity, Specificity, and Points Assigned to Independent Risk Factors
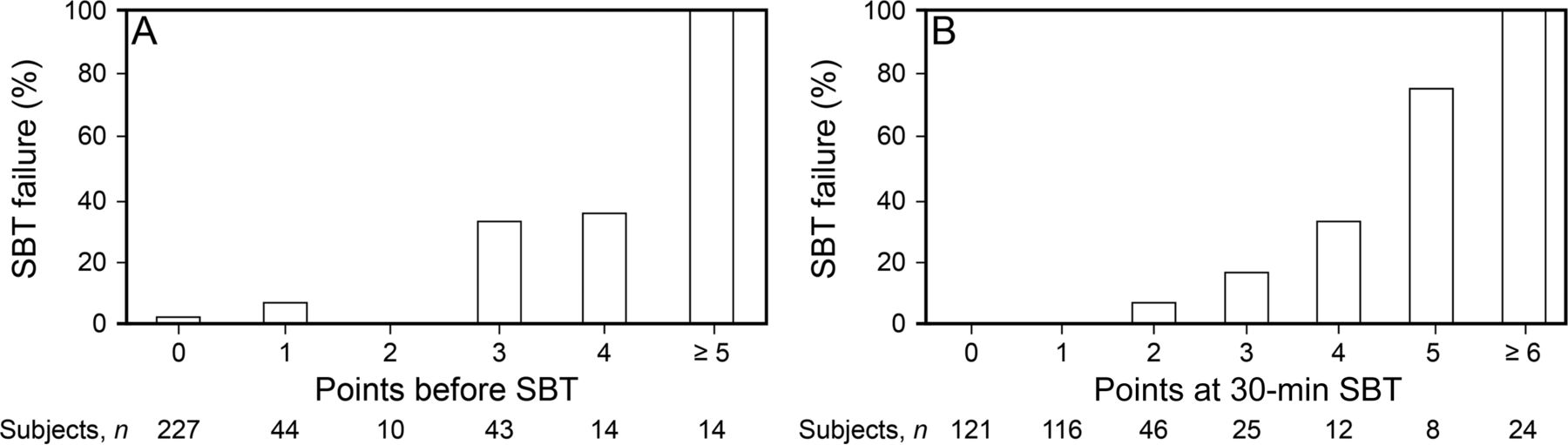
120-min spontaneous breathing trial failure rate in subjects with different points on the risk scale. SBT = spontaneous breathing trial.
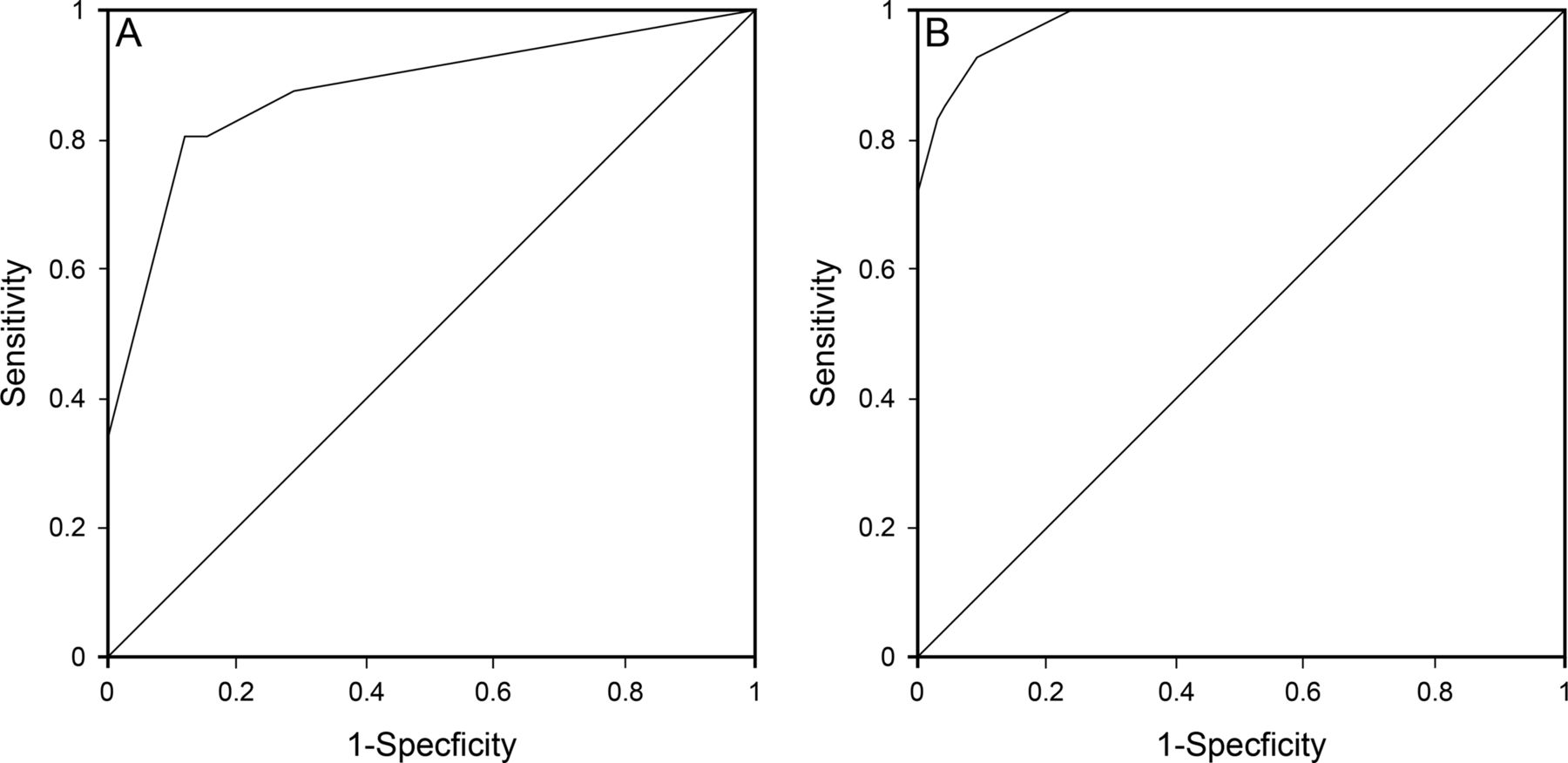
Power of risk scores to identify subjects who would experience 120-min spontaneous breathing trial (SBT) failure. A: Score developed before SBT, area under the curve = 0.88 (95% CI 0.81–0.95). B: Score developed at 30 min of SBT, area under the curve = 0.98 (95% CI 0.96–0.99).
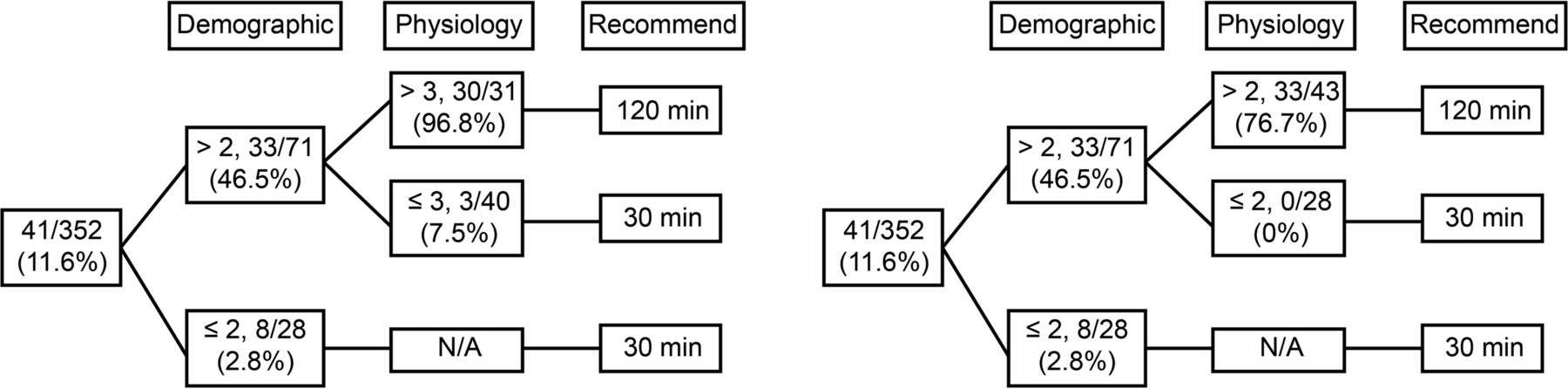
The decision tree to determine whether to prolong the SBT to 120 min. Different SBT failure rates in subjects with different points were descried in 2 models. The 2 models provide references for clinical practitioners to decide whether or not to prolong the SBT to 120 min.
Discussion
The current study observed an incidence of 30-min SBT success paired with 120-min failure of 11.6%. Before SBT, the presence of chronic cardiopulmonary disease, number of SBT attempts before 30-min SBT success, age, and PaCO2 were independently associated with 30-min SBT success + 120-min SBT failure. In addition, PaCO2, rapid shallow breathing index, ΔPaO2/FIO2 (T30-T0), Δbreathing frequency (T30-T0), and ΔpH (T30-T0) after 30 min of SBT were independently associated with 30-min SBT success + 120-min failure. Subjects with a higher score that incorporated these risk factors had a higher risk of 120-min SBT failure.
Several guidelines have recommended an SBT to assess readiness for ventilator weaning.5,6 A duration of between 30 and 120 min has also been recommended (ie, the SBT should last at least 30 min but no more than 120 min). However, 2 studies reported that the SBT failure rate was higher in subjects who received a 120-min SBT than in those who received only a 30-min SBT.7,8 This indicates that some subjects passed a 30-min SBT but encountered failure by 120 min. To the best of our knowledge, no study has yet reported the characteristics of these patients. Our study found that, in subjects with a risk score ≤2 points, a 30-min SBT may be sufficient. However, in subjects with a risk score >2 points, a 120-min SBT may be required.
In a previous study reported by Thille et al,10 subjects with advanced age and chronic cardiopulmonary disease were more likely to experience extubation failure. In their study, the SBT lasted only 60 min, indicating that a 60-min SBT may be inadequate to assess the ability of patients with advanced age or chronic cardiopulmonary disease to breathe unassisted. In another study focused on the elderly, the SBT failure rate increased from 20.3 to 35.8% if the duration of SBT was lengthened from 2 to 8 h; however, the extubation failure rate decreased from 48.4 to 7.5%.11 This study further confirmed that a lengthened SBT may be required in older patients. In our study, the mean time between initiation and SBT failure was 94 min in subjects who experienced a 30-min SBT success paired with 120-min failure. Advanced age and the presence of chronic cardiopulmonary disease were each risk factors for 30-min SBT success + 120-min SBT failure. Thus, a longer duration of SBT may be more appropriate in patients with advanced age or presence of chronic cardiopulmonary disease.
In our study, we also found that subjects who had already made one or more SBT attempts before this study were more likely to experience 30-min SBT success but 120-min failure. These subjects were classified as those with difficult or prolonged weaning based on the consensus of the European Respiratory Society, the American Thoracic Society, and the European Society of Intensive Care Medicine.12 After a 30–120-min SBT, subjects with this classification more often experience a higher rate of extubation failure than subjects who have undergone simple weaning.13 This may indicate that a 30–120-min SBT may not fully identify the ability of difficult or prolonged-weaning patients to spontaneously breathe. A longer SBT may be required in these patients.
The rapid shallow breathing index is commonly measured during SBT to predict successful weaning. However, a previous study reported that the rapid shallow breathing index increased significantly after 30 min of the SBT and increased further after 60 min in subjects with extubation failure but did not increase in subjects with extubation success.14 In this study, the rapid shallow breathing index was increased but still within an acceptable range after a 30-min SBT. However, when the SBT lasted 60 min, the rapid shallow breathing index exceeded accepted ranges. This serves as yet another indicator that a 30-min SBT may overestimate spontaneous breathing ability. In our study, we found that subjects with a rapid shallow breathing index >69 at 30 min of SBT were more likely to experience 30-min SBT success but proceed to failure at 120 min. In these patients, a longer duration of SBT may be more reasonable.
Our study was limited by the methodology. The SBT was applied via low-pressure support. However, a low-pressure support may overestimate the ability of the body to spontaneously breathe compared with a T-piece.15 Also, subjects with a T-piece were more likely to experience SBT failure than subjects with a low-pressure support.16 Therefore, the use of low-pressure support may mask early SBT failure. This may partly explain why 11.6% of subjects experienced at least 30 min of SBT success but failed by 120 min in our study. However, SBT also can be performed using a continuous positive airway pressure device or a T-piece. Because these 2 methods were not involved in our study, this issue requires further exploration. In addition, the decision tree was developed in accordance with the cut-off value measured at the beginning and at 30 min of SBT. However, the power of the decision tree needs to be duplicated in multi-center trials.
Conclusions
A 30-min SBT performed with 7 cm H2O of pressure support may overestimate the ability to spontaneously breathe. In subjects with a risk score ≤2 points, the 30-min SBT was sufficient. However, in those with a risk score >2 points, a 120-min SBT may be required.
Footnotes
- Correspondence: Yan Kang MD, Department of Critical Care Medicine, West China Hospital, Sichuan University, No. 37 Guoxue Road, Chengdu, Sichuan 610041, China. E-mail: Kang_yan_123{at}yahoo.com or Kang_yan_123{at}163.com.
The authors have disclosed no conflicts of interest.
See the Related Editorial on Page 493
- Copyright © 2018 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}