

Abstract
BACKGROUND: Impulse oscillometry is a method of airway assessment and diagnosis that provides data on lung mechanics. In the literature, studies have used different types of mouthpieces or did not describe the model used for the tests. We sought to compare the 3 most commonly described mouthpieces in terms of test results, comfort, and subject preference.
METHODS: Thirty-nine healthy volunteers were evaluated with spirometry and impulse oscillometry, assessing the resistance at 5 Hz and 20 Hz (R5 and R20, respectively), reactance at 5 Hz (X5), reactance area, and resonant frequency. A filter heat exchanger with a circular mouthpiece (B1), a filter heat exchanger with an oval mouthpiece (B2), and a filter heat exchanger with a circular mouthpiece coupled with a free-flow piece (B3) were compared using an acceptability and tolerance scale, and subjects noted their preference.
RESULTS: Statistical analysis showed differences between all the mouthpieces and the predicted values for R5, R20, and X5. The mouthpiece comparison showed differences in R5 between a filter heat exchanger with an oval mouthpiece (B2) and a circular mouthpiece coupled with a free-flow piece (B3) (P = .007); resonant frequency between a filter heat exchanger with a circular mouthpiece (B1) and a filter heat exchanger with an oval mouthpiece (B2) (P = .004) and between a filter heat exchanger with a circular mouthpiece (B1) and a circular mouthpiece coupled with a free-flow piece (B3) (P = .003); and reactance area between a filter heat exchanger with a circular mouthpiece (B1) and a circular mouthpiece coupled with a free-flow piece (B3) (P = .01). In the subjective evaluation, acceptability and tolerance differences were found in the ease of carrying out the evaluation, and no difference was found with regard to the degree of discomfort. Ten subjects preferred a filter heat exchanger with a circular mouthpiece (B1), 15 preferred a filter heat exchanger with an oval mouthpiece (B2), and 14 preferred a circular mouthpiece coupled with a free-flow piece (B3).
CONCLUSIONS: A circular mouthpiece coupled with a free-flow piece (B3) appeared to be the most suitable mouthpiece for the impulse oscillometry tests. It assured smaller impedance values for the respiratory system, and subjects expressed the most confidence in using this mouthpiece.
Introduction
The impulse oscillometry system is a method of evaluating and diagnosing airway components that was developed using the forced-oscillation technique.1 Impulse oscillometry is distinguished from the forced-oscillation technique in that it obtains resistance and reactance measurements in multi-frequency bands.2
Impulse oscillometry is an accurate method that offers reliable data on respiratory mechanics, and it is easy to apply because it obtains measurements during quiet breathing and only requires passive cooperation from subjects.3 Measurements are made while the volunteer breathes through a mouthpiece, and this method provides respiratory system parameters such as impedance, resistance, reactance, and resonant frequency (Fres), in addition to those evaluated in the simple spirometry test.4 It has been shown to be a promising tool for the early detection of pulmonary alterations when compared to spirometry5–7 and may be a promising tool for assessing the effects of treatments.
To obtain standardized results, the tests must be performed with subjects in a sitting position with the feet supported, the head in a neutral position, and hands supporting their cheeks, because the quality of the impulse oscillometry evaluation can be compromised by the movement of cheeks and tongue and bad coupling of the lips to the mouthpiece.3 However, studies found in the literature describe the use of different mouthpiece models, and adequate methods for avoiding leakages and tongue movements during the tests are not well defined.
Considering that different models of commercially available mouthpieces exist and that there is no consensus about the most appropriate model to use, it is important to evaluate the most reliable and comfortable mouthpiece to eliminate variables that may compromise the results of the examination. The objective of this study was to compare the different types of mouthpieces used in impulse oscillometry laboratory studies with respect to test results, comfort, and subjects' ability to adhere to instructions for different types of mouthpieces.
QUICK LOOK
Current knowledge
Impulse oscillometry is a method of airway assessment and diagnosis that might help distinguish between variable and fixed airway obstruction, aiding in treatment decisions. Studies have used different types of mouthpieces or provided no description of the model used for the tests with an impulse oscillometry system.
What this paper contributes to our knowledge
In this study, the circular mouthpiece coupled with a free-flow piece appears to be the most suitable mouthpiece for evaluations in impulse oscillometry assessment. This mouthpiece ensured the lowest resistance values of the respiratory system and was referred to as the mouthpiece that provided greater safety to the volunteers during the tests.
Methods
This was a randomized study of 40 volunteers without pulmonary disease (age range was 18–30 y). The study was approved by the Human Research Ethics Committee of the Clinical Hospital of the Ribeirão Preto Medical School, University of São Paulo, under the CAAE process number 55678416.7.0000.5440. The subjects were informed about the objective and protocol of the study, and all provided signed informed consent. The sample was calculated based on the results of Handa et al,8 using a variable resistance at 5 Hz (R5) and assuming a 0.29-kPa/L/s effect with SD = 0.29, power = 0.95, and α = 0.05.
Subjects were initially assessed with a spirometer (Jaeger, Wurzburg, Germany) to certify that their pulmonary function was normal. Next they performed the impulse oscillometry tests with the subject in a seated position with the feet supported, the head in the neutral position, and using a nasal clip. The tests were performed with 3 commercially available mouthpieces that have been described previously in the literature: a filter heat exchanger with a circular mouthpiece (B1) (MicroGard Microbial Filter, Vyaire Medical, Mettawa, Illinois), with a diameter of 3 cm; a filter heat exchanger with an oval mouthpiece (B2) (Spirogard 2800/21, GVS do Brazil, Monte Mor, Brazil), with a diameter of 3 cm; and a filter heat exchange with a circular mouthpiece coupled with a free-flow piece that had lip-sealing flaps and a tongue depressor (B3) (FreeFlow mouthpiece, Vyaire Medical, Mettawa, Illinois), with a diameter of 5 cm (Figure 1). For each mouthpiece, at least 3 measurements were performed, and all evaluations were carried out in a single visit during the same time period each day (ie, between 11:00 am and 1:00 pm). Mouthpiece order was randomized using an Excel program (Microsoft, Redmond, Washington). Evaluated parameters included resistance at 5 Hz and 20 Hz (R5 and R20, respectively), reactance at 5 Hz (X5), reactance area (AX), and resonant frequency. During the procedure, the following instructions were given: Keep your tongue on the floor of your mouth, avoid coughing and/or swallowing, firmly support your cheeks with your hands, and keep your lips sealed to the mouthpiece to prevent air leaks.

A: Heat exchanger filter with the circular mouthpiece. D: Diameter of the circular mouthpiece. B: Heat exchanger filter with the oval mouthpiece. E: Diameter of the oval mouthpiece. C: Heat exchange filter with circular mouthpiece coupled with a free-flow piece. F: Diameter of the free-flow piece.
After performing the impulse oscillometry using each mouthpiece, the subjects responded to a 7-point scale assessing the acceptability, tolerance, and comfort for each test condition, in accordance with recommendations by Eaton et al.9 They were asked to rate the degree of ease in understanding the instructions, the degree of ease in performing the evaluation, the degree of fatigue, and the degree of discomfort (1 = extreme discomfort, 7 = no discomfort) (see the supplementary materials at http://www.rcjournal.com). At the end of the tests, the subjects were asked about their personal preference regarding which mouthpiece to use.
Data were analyzed using the statistical programs R (R Core Team, Vienna, Austria) and SAS Statistical Software (version 9.3; SAS Institute, Cary, North Carolina). Regression models with mixed effects for dependent variables were used for analysis. The averages of the 3 measures with random effects and α = 0.05 were used. For comparisons between the predicted and obtained values, 95% confidence intervals were calculated using the proportion of the observed value by the predicted value. P < .05 was considered significant.
Results
After performing spirometry, 1 subject was excluded from the study because the test results did not reach the predicted values of spiromety. Anthropometric and sociodemographic characteristics of the 39 subjects are shown in Table 1.
Volunteer Attributes
The subjects performed 3 (64%) to 5 tests with each mouthpiece. Differences were found between the means obtained for all mouthpieces and the predicted values for R5, R20, and X5. A comparison of the predicted and obtained values can be found in Table 2.
Predicted and Obtained Values for Resistance and Reactance
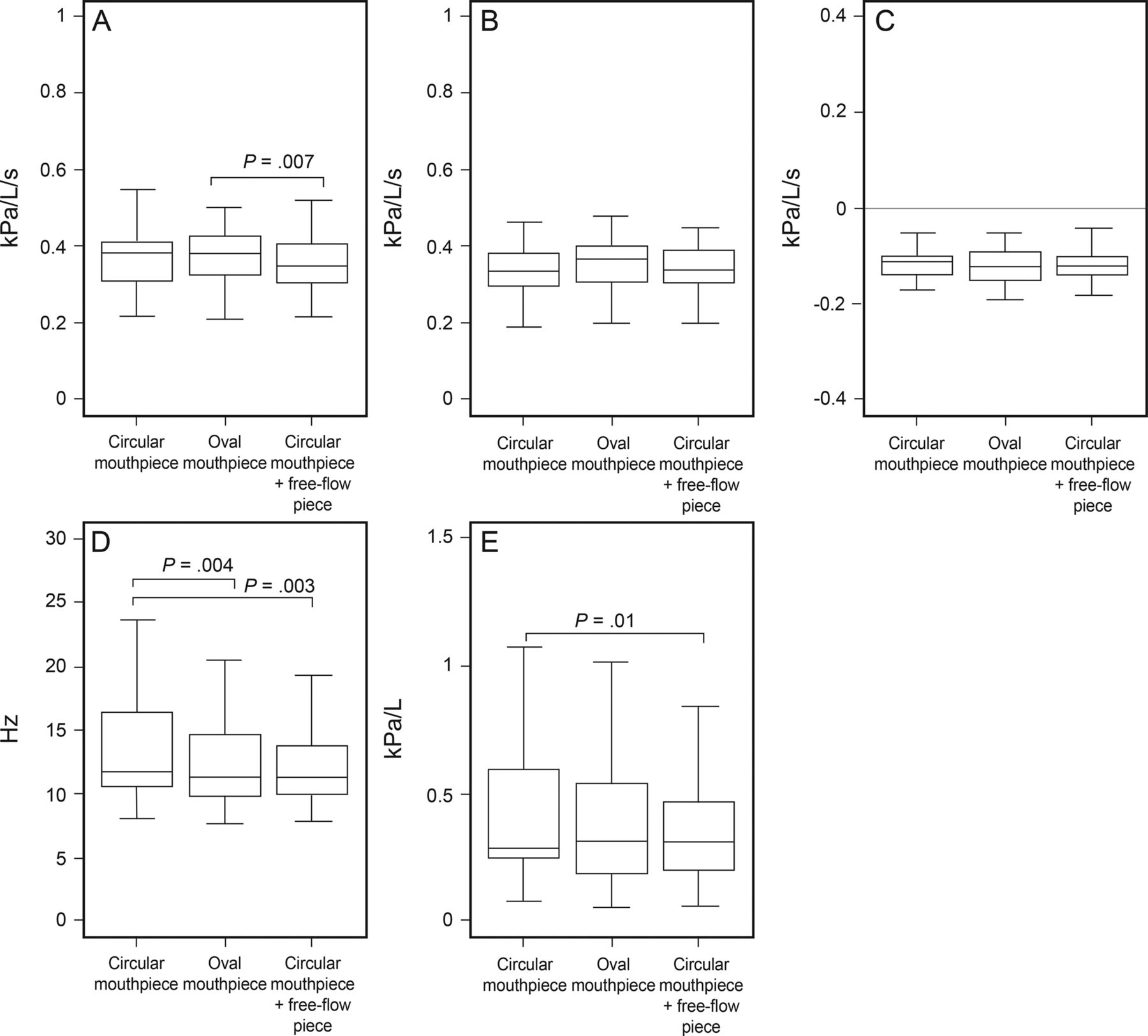
The comparison between the different mouthpieces showed differences in R5 (kPa/L/s) between a filter heat exchanger with an oval mouthpiece (B2) (0.37 ± 0.06) and a circular mouthpiece coupled with a free-flow piece (B3) (0.35 ± 0.07) (P = .007); in Fres (Hz) between a filter heat exchanger with a circular mouthpiece (B1) (13.33 ± 3.85) and a filter heat exchanger with an oval mouthpiece (B2) (12.31 ± 3.21) (P = .004) and between a filter heat exchanger with a circular mouthpiece (B1) (13.33 ± 3.85) and a circular mouthpiece coupled with a free-flow piece (B3) (12.29 ± 3.08) (P = .003); and in reactance area (kPa/L) between a filter heat exchanger with a circular mouthpiece (B1) (0.431 ± 0.29) and a circular mouthpiece coupled with a free-flow piece (B3) (0.372 ± 0.23) (P = .01). There was no difference between the different mouthpieces for the parameters R20 and X5 (Table 3, Figure 2).
Comparison Between the Different Mouthpieces

Box plot of comparisons among the mouthpieces a filter heat exchanger with a circular mouthpiece (B1), a filter heat exchanger with an oval mouthpiece (B2), and a circular mouthpiece coupled with a free-flow piece (B3) for the resistance at 5 Hz (A) and 20 Hz (B), reactance at 5 Hz (C), resonant frequency (D), and reactance area (E).
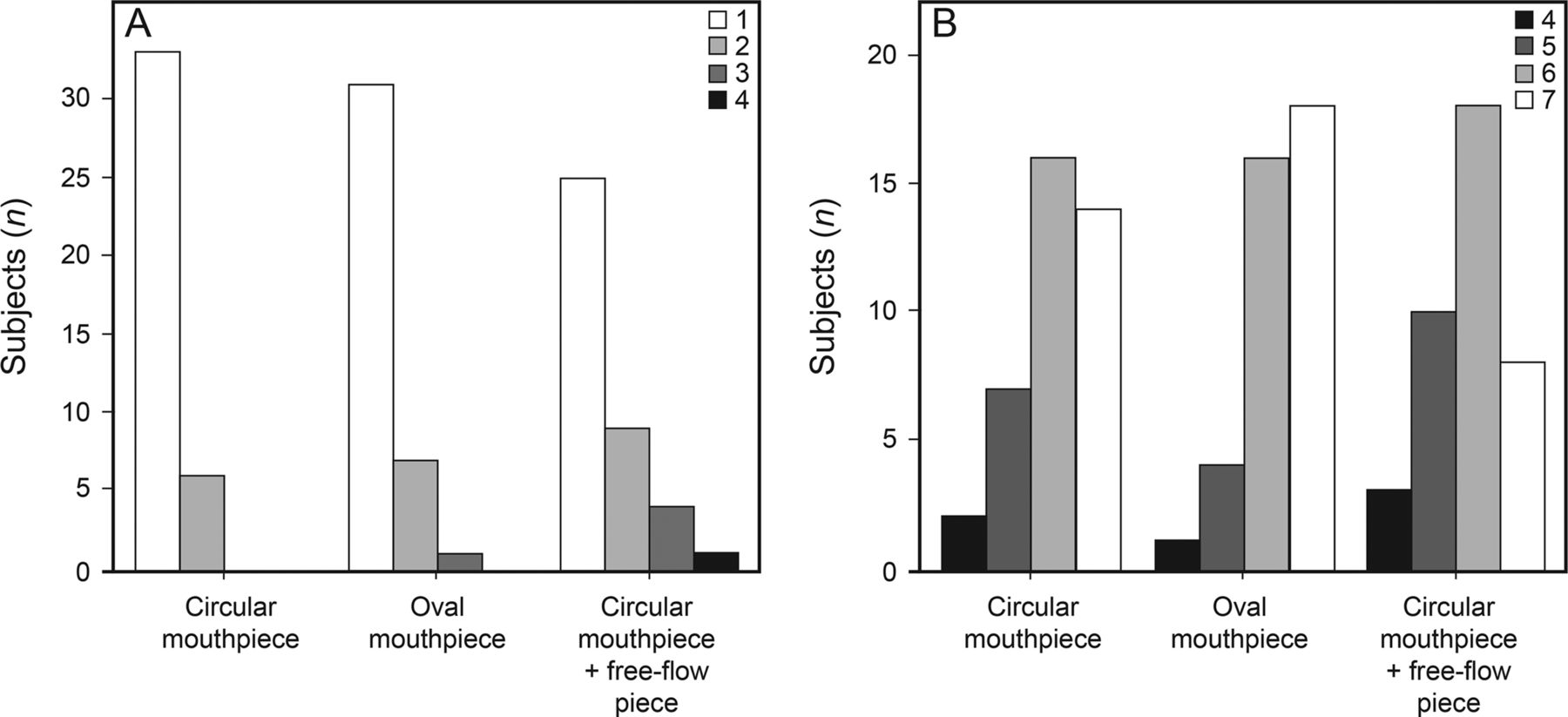
Regarding data from subjective evaluations, differences were found in the ease of understanding the instructions, but no difference was found in the degree of discomfort (Figure 3). In terms of subject preference for mouthpieces, 10 preferred the filter heat exchanger with a circular mouthpiece (B1), 15 preferred the filter heat exchanger with an oval mouthpiece (B2), and 14 preferred the circular mouthpiece coupled with a free-flow piece (B3).

Volunteer perceptions of ease and discomfort. Facility to conduct the evaluation (A) and degree of discomfort (B). 1 = extreme discomfort, 7 = no discomfort.
At the end of each evaluation, subjects were asked to report any mouthpiece complaints. The filter heat exchanger with a circular mouthpiece (B1) received 4 complaints about its use, the filter heat exchanger with an oval mouthpiece (B2) received 7 complaints, and the circular mouthpiece coupled with a free-flow piece (B3) received 9 complaints. The complaints about a filter heat exchanger with a circular mouthpiece (B1) and a filter heat exchanger with an oval mouthpiece (B2) concerned difficulties in positioning the tongue and completely sealing the lips. Some subjects reported a dry mouth sensation; 2 subjects described nausea. Complaints about a circular mouthpiece coupled with a free-flow piece (B3) mainly involved difficulties opening the mouth and wrapping the lips over the flaps; after the initial mouth positioning, however, subjects reported that they felt more confident during the test because they could relax their lips, which fit the flaps and helped seal against air leakage, while their tongue remained relaxed under the depressor. Excessive salivation, swallowing, and nausea were among the complaints reported for a circular mouthpiece coupled with a free-flow piece (B3), although none of these interrupted the tests. Despite the complaints about the use of a circular mouthpiece coupled with a free-flow piece (B3), 10 subjects reported a greater sense of security with a circular mouthpiece coupled with a free-flow piece (B3) and expressed that this sense of security made the test run more smoothly. There was no similar report for a filter heat exchanger with a circular mouthpiece (B1) and a filter heat exchanger with an oval mouthpiece (B2).
Discussion
In this study, the predicted impulse oscillometry values for resistance at 5 Hz and 20 Hz were calculated with Launch SentrySuite (version 2.11, Jaeger) using the standard equation (ie, parameters include age, height, and weight), and predicted values differed from the obtained values for all evaluated mouthpieces. One reason for this difference is related to the reference values, which are based on a sample of the German population,2,10–14 and we consider that the use of this equation deserves caution.
Values of normality have already been described in specific populations, such as adults2,11–13 and children14–19 of different nationalities. It is necessary to note that the age of the groups included in the reference equations, which is 1 parameter used to calculate the predicted values, included no overlaps with the age range of the subjects of this study (18–30 y). Only Newbury et al2 carried out a study with subjects who were between 25 and 74 y old; all other equations use subjects > 30 y old.11–13 In addition, no study has been conducted to establish the normal value range for the adult Brazilian population. We did not find comparisons between the equations for adults, but a recent study for the pediatric age group showed significant differences between the available equations.18
The comparison between the different mouthpieces showed lower values for R5, reactance area, and Fres when using a circular mouthpiece coupled with a free-flow piece (B3) when compared to a filter heat exchanger with a circular mouthpiece (B1), and lower values for R5 when using a circular mouthpiece coupled with a free-flow piece (B3) compared to a filter heat exchanger with an oval mouthpiece (B2). Taken together, these results suggest an advantage for using a circular mouthpiece coupled with a free-flow piece. Even small changes in resistance can be considered significant, and it is worth highlighting studies that showed a positive response to bronchodilator variations (R5 changed from 3.19 to 2.91 cm H2O)20 and inspiratory variations (R5 changed from 0.29 to 0.26 kPa/L/s).21 We believe that the difference in the findings between a circular mouthpiece coupled with a free-flow piece (B3), which was considered the best mouthpiece for the test, and the other mouthpieces lies in the use of the free-flow piece, as subjects reported greater confidence in their tongue positioning when using this mouthpiece.
The obtained values in this study showed a greater standard deviation than the predicted values. Despite these differences, data from the literature reported similar or even higher standard deviations in subjects without respiratory diseases. Nikkhah et al22 evaluated 87 subjects and found a R5 mean value of 0.40 ± 0.30 kPa/L/s. Crim et al23 conducted a study with 233 subjects and found a R5 mean value of 0.33 ± 0.10 kPa/L/s and a R20 mean value of 0.26 ± 0.07 kPa/L/s. Wollmer et al24 reported values of 0.30 ± 0.11 kPa/L/s for R5, using data obtained from 82 subjects. Another study carried out in Brazil evaluated 31 subjects and found mean values of 4.3 ± 1.1 and 3.7 ± 1.0 cm H2O/L/s for R5 and R20, respectively.25
Some studies that use impulse oscillometry as an evaluation method do not describe the mouthpiece model used to perform the test.26,8,27 These studies only report that Oostveen's recommendations were followed.3 There is, however, no description of a specific mouthpiece in Oostveen's recommendations for impulse oscillometry, only a description of the use of the nasal clip, the need to use hands to support the cheeks, and guidelines to avoid swallowing or closing the glottis during the test,3 similar to the recommendations for spirometry. According to American Thoracic Society, the recommended instructions for spirometry standardization include using a nasal clip and sealing one's lips around the mouthpiece (open circuit) to avoid obstructing air flow, but there is no description of mouthpiece models or shapes, nor is there information on how the use of different mouthpieces may influence the applicability of the technique.28
Other authors have demonstrated the importance of using a mouthpiece that is suitable for adults and children to achieve the level of contraction of the facial muscles needed for good attachment of the lips to the mouthpiece (thereby avoiding leaks), yet no reports have defined or described the model of the mouthpiece they used.4,29 The authors acknowledge that differences in current assessment techniques using the forced-oscillation technique and different mouthpiece models might create some degree of uncertainty between expected normal values for resistance and reactance parameters in adults and children.4,29
A study that sought to provide an overview of the impulse oscillometry application in children with airway diseases used the free-flow mouthpiece and also instructed subjects to support their cheeks with their hands.30 Other authors developed their methodologies for impulse oscillometry based on this study.6,31
Goldman et al32 demonstrated that improperly positioning the tongue uniformly increased resistance in all frequencies tested. In our study, subjects were instructed to avoid inappropriate positioning of the tongue, and to try to keep their tongue on the floor of the mouth; however, even with these instructions, the impedance values obtained were higher when subjects did not use the free-flow piece. The difference was statistically significant for R5 as well as for reactance area and resonant frequency. We believe that the difference between the mouthpiece used in a circular mouthpiece coupled with a free-flow piece (B3), considered the best mouthpiece for the test, and the other mouthpieces is its coupling with the free-flow piece, as this piece created a greater confidence regarding tongue positioning. In all likelihood, the differences were small in this study because the subjects were oriented to the correct positioning of the tongue, which did not occur in the Goldman et al study.32
To try to eliminate a different source of variability, all evaluations were performed in a single session and in the same period of the day (between 11:00 am and 1:00 pm). Studies in the literature have demonstrated a day-to-day variability for impulse oscillometry parameters of 5–15% in adults and 16–17% in children. This degree of variability indicates that obtaining similar repeated measures is not difficult and that impulse oscillometry is a fairly reproducible test.33
The complaints presented by the study subjects concerned difficulties in positioning the tongue and completely sealing the lips around the circular and oval mouthpieces. Some subjects reported dry mouth; 2 subjects described mild nausea. On the other hand, the complaints regarding the free-flow mouthpiece mostly involved difficulties opening the mouth and wrapping the lips over the flaps; after the initial mouth positioning, however, subjects reported that they felt more secure and could relax their lips because the mouthpiece provided a better fit and helped seal against air leaks. Of note, this reported difficulty in opening the mouth might make this free-flow piece unviable in smaller individuals or children.
It is important to assess supply costs. The filter heat exchanger with a circular mouthpiece (B1) and filter heat exchanger with an oval mouthpiece (B2) have similar prices, and the free-flow piece carries an additional cost. While the combined components of a circular mouthpiece coupled with a free-flow piece (B3) means that a circular mouthpiece coupled with a free-flow piece (B3) costs more, the free-flow piece can be sterilized and reused, thus improving the cost-benefit ratio.
As a limitation, our study was performed with adults, and we did not measure the degree or effort of opening the mouth for the mouthpieces; the restriction of the opening could make it difficult to position the mouthpiece for some participants. Likewise, dental alignment was not evaluated, which may influence the connection between mouth and mouthpiece. Future studies should investigate the influence of dental alignment, especially given that no study to date has yet included dental alignment as a possible source of variability. Additionally, future studies could repeat this study in other age groups.
Conclusions
The results suggest that a circular mouthpiece coupled with a free-flow piece (B3), a circular mouthpiece coupled with a free-flow piece, is the most suitable mouthpiece to use when using impulse oscillation for airway assessment. Although the difference is not clinically important, the use of a circular mouthpiece coupled with a free-flow piece (B3) produced the lowest impedance values, and subjects referred to it as the mouthpiece that provided them with the greatest confidence.
Footnotes
- Correspondence: Ada Clarice Gastaldi PT PhD, Department of Physiotherapy, Ribeirão Preto Medical School, University of São Paulo, Ribeirão Preto, Brazil. E-mail: ada{at}fmrp.usp.br.
Supplementary material related to this paper is available at http://www.rcjournal.com.
The authors have disclosed no conflicts of interest.
- Copyright © 2018 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}