

Abstract
BACKGROUND: A normal heart rate reflects the balance between the sympathetic and parasympathetic autonomic nervous system. When the difference between heart rate at the end of an exercise test and after 1 min of recovery, known as the 1-min heart rate recovery, is ≤ 12 beats/min, this may indicate an abnormal delay. We sought to compare physical activity patterns and subjects' functional status with COPD with or without delayed 1-min heart rate recovery after the 6-min walk test (6MWT).
METHODS: 145 subjects with COPD (78 men, median [interquartile range (IQR)] age 65 [60–73] y, body mass index 25 [21–30] kg/m2, FEV1 45 ± 15% predicted) were underwent the following assessments: spirometry, 6MWT, functional status, and physical activity in daily life (PADL). A delayed heart rate recovery of 1 min was defined as ≤ 12 beats/min.
RESULTS: Subjects with delayed 1-min heart rate recovery walked a shorter distance in the 6MWT compared to subjects without delayed heart rate recovery (median [IQR] 435 [390–507] m vs 477 [425–515] m, P = .01; 81 [71–87] vs 87 [79–98]% predicted, P = .002). Regarding PADL, subjects with delayed heart rate recovery spent less time in the standing position (mean ± SD 185 ± 89 min vs 250 ± 107 min, P = .002) and more time in sedentary positions (472 ± 110 min vs 394 ± 129 min, P = .002). Scores based on the self-care domain of the London Chest Activity of Daily Living questionnaire and the activity domain of the Pulmonary Functional Status and Dyspnea questionnaire were also worse in the group with delayed heart rate recovery (6 ± 2 points vs 5 ± 2 points; P = .039 and 29 ± 24 points vs 19 ± 17 points; P = .037, respectively).
CONCLUSIONS: Individuals with COPD who exhibit delayed 1-min heart rate recovery after the 6MWT exhibited worse exercise capacity as well as a more pronounced sedentary lifestyle and worse functional status than those without delayed heart rate recovery. Despite its assessment simplicity, heart rate recovery after the 6MWT can be further explored as a promising outcome in COPD.
Introduction
Heart rate dysfunction in COPD has been a target of increasing scientific interest in recent years.1–4 A normal heart rate reflects the balance between the sympathetic and parasympathetic autonomic nervous system. Within this context, when there is a dysfunction in the parasympathetic system, an abnormal delay of heart rate recovery after exercise may occur.2 When the difference between heart rate at the end of an exercise test and after 1 min of recovery, known as the 1-min heart rate recovery, is ≤ 12 beats/min, this may indicate an abnormal delay.2
The 1-min heart rate recovery is commonly evaluated after cardiopulmonary exercise tests.2,3 It has also been evaluated after the 6-min walk test (6MWT) as a simpler way to identify abnormal heart rate recovery in patients with COPD because some physiologic variables, such as heart rate, can also be obtained before, during, and after the test recovery period.1,4
The 6MWT is widely used to evaluate functional exercise capacity in the context of pulmonary rehabilitation.5 In addition, it is easy, practical, inexpensive, and reproducible in clinical settings.6 The 6-min walk distance (6MWD) is commonly used to evaluate prognosis and treatment responses in chronic respiratory diseases.5 Recent literature has suggested that the 1-min heart rate recovery after the 6MWT is an independent predictive factor of exacerbations in COPD.4 Moreover, Shiroishi et al1 analyzed its association with variables such as anthropometric, spirometric, and health-related questionnaires. Delayed 1-min heart rate recovery was associated with reduced functional capacity, quality of life, and percutaneous oxygen saturation recovery.1 However, it is still unknown whether patients with COPD and delayed heart rate recovery demonstrate similar physical activity patterns and functional status compared to patients with normal heart rate recovery.
Individuals with COPD spend less time walking and have reduced levels of physical activity in daily life (PADL) compared to healthy elderly individuals.7,8 Recently, the objective measurement of PADL using motion sensors has gained increasing visibility in the scientific literature, especially in individuals with COPD,9 because the PADL level is known to be the main predictor of mortality in this disease,10 in addition to its close relationship with health status and physical deconditioning.7
Similarly to PADL level, delayed 1-min heart rate recovery is an independent predictor of mortality and cardiovascular diseases in individuals with COPD.2,3 Therefore, it was hypothesized that individuals with abnormal heart rate recovery would exhibit worse functionality and PADL level compared to those with normal heart rate recovery. We aimed to compare the physical activity pattern and functional status of individuals with COPD with or without delayed 1-min heart rate recovery after the 6MWT.
QUICK LOOK
Current knowledge
Heart rate recovery after exercise tests is an independent predictor of mortality and cardiovascular diseases in individuals with COPD. Alternatively, this variable has also been evaluated after a simpler test such as the 6-min walk test (6MWT). Recent literature has suggested that a 1-min heart rate recovery after the 6MWT is an independent predictive factor of exacerbations and is associated with functional capacity and quality of life.
What this paper contributes to our knowledge
Individuals with COPD who had delayed 1-min heart rate recovery after the 6MWT presented reduced exercise capacity, more marked sedentary lifestyle, and worse self-reported functional status compared to individuals without delayed heart rate recovery.
Methods
Study Design and Sample
This was an observational, cross-sectional, retrospective study, with a convenience sample of subjects with COPD who were recruited during inclusion in a pulmonary rehabilitation program at the Laboratory of Respiratory Physiotherapy Research in Londrina, Brazil.11 Individuals included in the study were diagnosed with COPD according to Global Initiative for Chronic Obstructive Lung Disease (GOLD).12 Inclusion criteria were absence of exacerbation with hospitalization in the last 3 months, absence of severe and/or unstable cardiac disease that could interfere with testing5, and not having participated in a pulmonary rehabilitation program in the previous year. Patients were excluded if they interrupted the 6MWT or were unable to perform the proposed tests, as were subjects with missing data. The institution's research ethics committee approved this study (no. 123/09 and 173/2012), and all participants signed an informed consent form.
Assessments
Exercise capacity was assessed with the 6MWT according to international guidelines.5 A trained staff applied the test in a 30-m corridor, with standardized encouragement. Two tests were performed with an interval of 30 min between them, and the longest walked distance was considered for analysis.6 Heart rate, peripheral oxygen saturation (SpO2), blood pressure, and dyspnea and fatigue symptoms (modified Borg scale) were monitored before and after the test. Reference values for Brazilian population were used.13 Heart rate was measured during the 6MWT, immediately after the test, and 1 min after the end of the test (ie, in recovery) with a portable pulse oximeter (Moriya M1001, São Paulo, Brazil). The longest 6MWD was recorded, and the recovery heart rate was calculated based on this value. Individuals were divided into 2 groups according to the 1-min heart rate recovery. Those who had a 1-min heart rate recovery ≤ 12 beats/min were considered as having an abnormal delay in 1-min heart rate recovery, whereas individuals who had heart rate recovery > 12 beats/min were identified as having no delay in heart rate recovery, as previously described.2
The individuals also underwent pulmonary function evaluation with spirometry using a portable spirometer (Spiropalm, COSMED, Italy). The technique was performed according to international guidelines,14 and the reference values used were those specific for the Brazilian population.15
Concerning PADL, all subjects were evaluated using the DynaPort MoveMonitor (McRoberts, The Netherlands). The Dynaport is a physical activity monitor containing a triaxial accelerometer, validated for individuals with COPD, that is placed on the individuals' lower back to perform a long-term PADL assessment. It discerns and quantifies movement patterns and body positions, providing the following variables: time spent walking, time spent standing, time spent sitting, time spent lying down (all of them in min/d), and movement intensity when walking (m/s2).16,17 The monitor was used 12 h/d for 2 consecutive days, and the average values of these 2 days were used for analysis.18
Individuals were also assessed with the following questionnaires: the modified Medical Research Council scale, a validated Portuguese language instrument that is used to assess the degree of dyspnea in daily life19; the St George Respiratory Questionnaire, a specific quality-of-life questionnaire for individuals with COPD validated in Portuguese language20; and the London Chest Activity of Daily Living scale (LCADL)21 and Pulmonary Functional Status and Dyspnea Questionnaire – modified version (PFSDQ-M),19 which are instruments to assess functional status (ie, self-reported performance in daily living activities). Furthermore, the presence of comorbidities was investigated with a self-reported questionnaire, which included conditions such as stable cardiac disease, vascular disease, systemic hypertension, and others. In this study, a stable cardiac disease was considered as any self-reported cardiac disease that was clinically controlled.
Statistical Analysis
For the statistical analysis, GraphPad Prism software version 6.0 (GraphPadPrism, La Jolla, California) was used. Data distribution was analyzed using the Kolmogorov-Smirnov test. According to normality in the data distribution, the non-paired t test or the Mann-Whitney test were used to compare the individuals' characteristics with and without 1-min heart rate recovery delay, whereas the chi-square test was used for the comparison of categorical variables. Pearson or Spearman coefficients were used to analyze the correlation among the studied variables, again according to the normality in data distribution. Statistical significance was set as P < .05.
Results
A total of 162 subjects diagnosed with COPD were evaluated, but 17 individuals were excluded (5 subjects due to incomplete heart rate data and 12 due interrupted 6MWT caused by lower limb fatigue or severe dyspnea or desaturation during the test). Thus, data from 145 subjects were included in the final analysis. None of the individuals reported participating in a pulmonary rehabilitation program before.
In this sample, 19 subjects were using β blockers (9 from the group without delay in the 1-min heart rate recovery, and 10 from the group with a delay in heart rate recovery). Results did not change when these individuals were excluded from the analysis, so they were maintained in the sample.
Subjects' mean (range) age was 65 (60–73) y, and the degree of air-flow obstruction was classified ranging from moderate to severe (Table 1). The median (IQR) number of comorbidities reported per individual was 2 (1–3), and 112 (77%) subjects had at least 1 comorbidity. The most common comorbidities among subjects were systemic hypertension (53%) and vascular disease (34%) (Table 2). In addition, there were no differences in the proportion of comorbidities among the individuals who presented delay in heart rate recovery versus those who did not (P = .38) (Table 2).
Individuals' Characteristics Included in the Study Without and With Delay in the 1-Min Heart Rate Recovery
Subject Comorbidities
The median (IQR) 6MWD for the total sample was 465 (412–510) m, which corresponds to 85 [77–94]% of the predicted distance. Baseline heart rate (ie, before the 6MWT), was 86 ± 14 beats/min, and the median (IQR) 1-min heart rate recovery for all subjects was 16 (7–24) beats/min.
Regarding PADL, the total sample exhibited a median (IQR) time spent walking and time spent standing of 55 (37–81) min/d and 209 (147–276) min/d, respectively. The median (IQR) times spent in sedentary postures were 107 (25–183) min/d in lying positions, 317 (248–386) min/d in sitting positions, and 443 (341–514) min/d in combined sedentary postures (lying and sitting positions).
Table 1 describes the characteristics of the total sample included in the study and presents the comparison of the anthropometric, demographic, and spirometric variables of individuals classified without and with delay in 1-min heart rate recovery. There were no significant differences between these groups regarding the aforementioned outcomes.
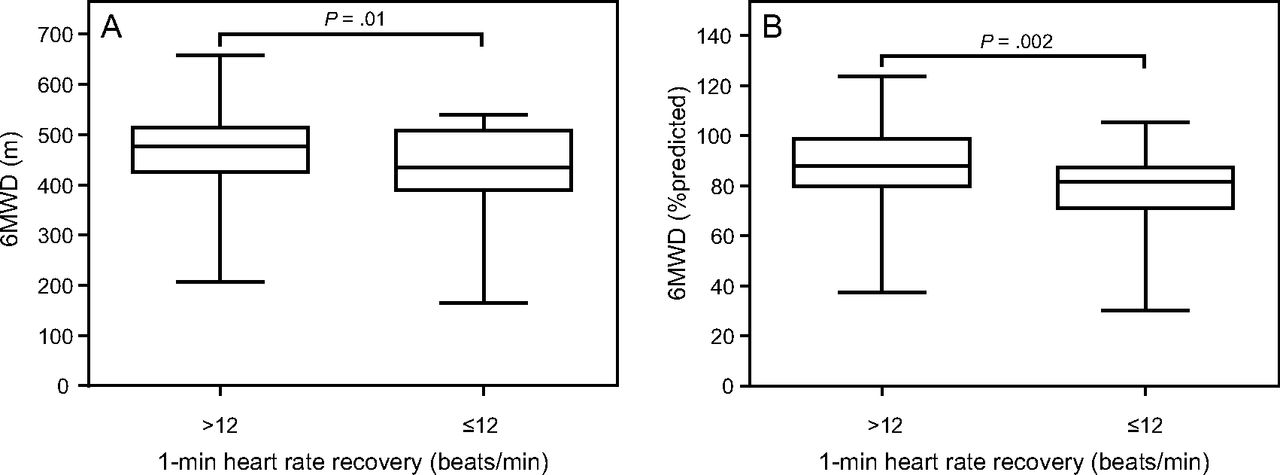
Subjects with delayed 1-min heart rate recovery walked a shorter 6MWD compared to individuals without a delay in heart rate recovery: 435 (390–507) m vs 477 (425–515) m (P = .01). This was accompanied by a lower percentage of predicted distance: 81 (71–87)% vs 87 (79–98)% (P = .002), as shown in Figure 1. When the 6MWD was stratified by disease degree, individuals without delay in the 1-min heart rate recovery and classified as GOLD I and II (n = 39) walked farther than those classified as GOLD III and IV (n = 53; GOLD I and II 500 [455–540] m vs GOLD III and IV 465 [417–495] m, P = .005). On the other hand, there was no difference in the comparison of individuals with delayed heart rate recovery classified as GOLD I and II (n = 19) versus GOLD III and IV (n = 34) (GOLD I and II 445 [413–523] m vs GOLD III and IV 426 [360–501] m, P = .08). Similarly, in the PADL variables obtained by the DynaPort MoveMonitor, individuals with delayed 1-min heart rate recovery spent less time standing (185 ± 89 min/d vs 250 ± 107 min/d, P = .002) and more time in sedentary postures (lying down + sitting position) compared to individuals without heart rate recovery delay (472 ± 110 min/d vs 394 ± 129 min/d, P = .002) (Fig. 2).
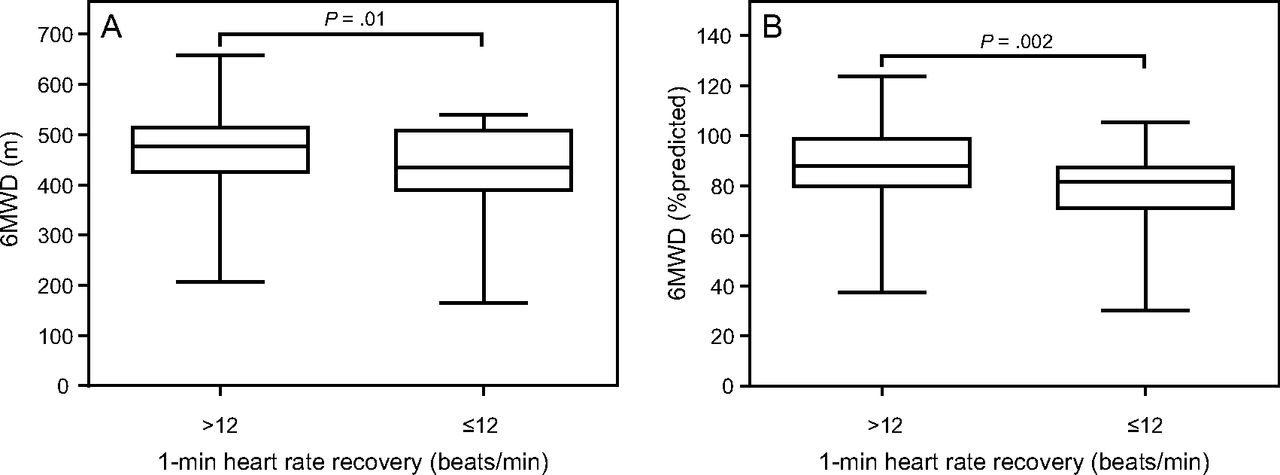
Box and whisker plots of the comparison of the distance covered (A) in the 6-min walk test (6MWT) and the percentage of predicted values (B) reached in the test between individuals without and with delay in 1-min heart rate recovery after the end of the 6MWT. Lines denote the median and the 25th percentile and 75th percentile interquartile range, and whiskers show minimum and maximum values.
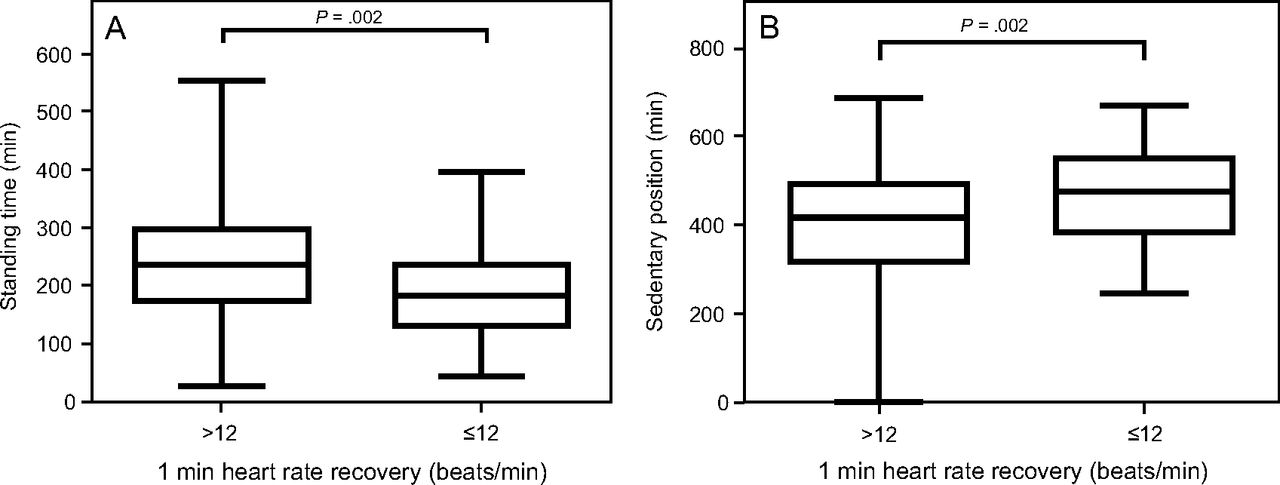
Box and whisker plots of the comparison of standing time (A) and time in sedentary (combined lying and seated) position (B) between individuals without and with delay in the 1-min heart rate recovery after the end of the 6-min walk test. Lines denote the median and the 25th percentile and 75th percentile interquartile range, and whiskers show minimum and maximum values.
Regarding functional status, the score obtained in the self-care domain of the LCADL questionnaire was higher in the group with delayed 1-min heart rate recovery (6 ± 2 points vs 5 ± 2 points, P = .039) as well as in the activity domain of the PFSDQ-M questionnaire (29 ± 24 vs 19 ± 17, P = .037) compared to individuals without heart rate recovery delay, indicating a worse functional status for these individuals (Fig. 3). No significant differences were found in the other studied variables.

Box and whisker plots of the comparison of the London Chest Activities of Daily Living scale (LCADL) self-care domain questionnaire score (A) and the Pulmonary Functional Status and Dyspnea questionnaire – modified version (PFSDQ-M) activity domain score (B) between individuals without and with delay in 1-min heart rate recovery after the end of the 6-min walk test. Lines denote the median and the 25th percentile and 75th percentile interquartile range, and whiskers show minimum and maximum values.
Analysis of the relationship between the 1-min heart rate recovery in the 6MWT and other variables such as anthropometric data, exercise capacity, and questionnaires showed significant but weak correlations between 1-min heart rate recovery and 6MWT, both in meters and in percentage predicted (r = 0.23, P = .004 and r = 0.26, P = .001, respectively). Heart rate recovery was also significantly but weakly correlated with standing time (r = 0.23, P = .02), LCADL self-care domain (r = −0.19, P = .01), PFSDQ-M activity domain (r = −0.20, P = .01), PFSDQ-M dyspnea domain (r = −0.17, P = 003), and PFSDQ-M fatigue domain (r = −0.20, P = .01). No other significant correlations were found.
Discussion
In this study, individuals with delayed 1-min heart rate recovery displayed reduced functional exercise capacity in comparison to individuals without delayed heart rate recovery. Similarly, objectively assessed physical activity and self-reported functional status were worse among individuals with delayed heart rate recovery.
This is the first study to evaluate 1-min heart rate recovery delay after the 6MWT together with objectively measured PADL variables. Although it is not possible to identify causality of these impairments, individuals with delayed heart rate recovery presented a more pronounced sedentary lifestyle. It should be highlighted that the deleterious effects of sedentary behavior are unquestionable among individuals with COPD. A previous study showed that sedentary behavior is a predictor of mortality in individuals with COPD regardless of the exercise capacity or moderate to vigorous physical activity.22 Similarly, it is well known that the delay in 1-min heart rate recovery is an independent predictor of cardiovascular disease and mortality in individuals with COPD.2,3,23
There is a variety of heart rate recovery cutoff points available in the scientific literature to determine the delay in 1-min heart rate recovery. In the study by Lacasse et al,3 the cutoff point used to characterize the delay in heart rate recovery was ≤ 14 beats/min, but most studies used the cutoff point of ≤ 12 beats/min.1,23,24 Moreover, the most widely used way to assess delayed 1-min heart rate recovery is through a maximum exercise test performed on a cycle ergometer or treadmill.2,3,24 However, Shiroishi et al1 recently evaluated the heart rate recovery delay following the 6MWT and found a relationship between distance covered in the test and oxygen saturation recovery in subjects with COPD. Hence, the 6MWT may be a more affordable option because it is a simple and practical field test.
In this study, there was no difference in the comparison of the anthropometric and spirometric variables between the groups with and without delayed 1-min heart rate recovery. These results corroborate the findings of Shiroishi et al,1 who also found no differences between these groups. On the other hand, Seshadri et al24 found different results, presenting an association between abnormal heart rate recovery and disease severity (predicted FEV1% odds ratio 1.93 95% CI 1.12–2.91). This finding may be explained by the fact that this study included subjects with a variety of chronic respiratory diseases and not solely COPD.24
In this study, there was a difference in exercise capacity between those with and those without delay in 1-min heart rate recovery. In fact, autonomic cardiac function is independently associated with exercise capacity in individuals with COPD.1 However, it is not possible to determine how much of the heart rate recovery is attributed to autonomic dysfunction in this sample because more details about the subjects' cardiovascular function would be necessary. Similarly, the difference in PADL between the 2 groups may have occurred because subjects with delayed heart rate recovery exhibit lower exercise capacity, and it is known that PADL is related to the 6MWT.8 Moreover, it has been shown that heart rate variability is related to a reduced level of PADL.25
Our finding that a delayed 1-min heart rate recovery indicated worse functional status is similar to results found in the study by Camillo et al.25 They demonstrated a correlation among heart rate variability, worse functional status, and worse quality of life for subjects with COPD. From these results it is possible to obtain information about functional status and quality of life for these subjects through a simple evaluation of the delayed heart rate recovery. This information may be helpful in developing appropriate interventions to improve these variables.
The delay in 1-min heart rate recovery correlated only weakly with 6MWT variables, with the percentage of predicted in the test, and with variables obtained by questionnaires such as LCADL in the self-care domain and PFSDQ in the activity, dyspnea, and fatigue domains. Similarly weak correlations were found between the 1-min heart rate recovery and body mass index, St George Respiratory Questionnaire 6MWD, and dyspnea in the study by Shiroishi et al.1 Due to the weak nature of these correlations, it is not possible to clearly indicate that the greater the difference in heart rate recovery, the milder the functional impairment; nevertheless, this information can provide additional knowledge to explain the results found in our study. Indeed, the cross-sectional design of our study does not allow one to draw a cause and effect conclusion, suggesting that future studies may contribute to a better understanding of these associations. On the other hand, these conclusions may serve as an interesting initial step in this poorly explored topic related to patients with COPD.
Finally, it is suggested that the use of β-blocker medications alters cardiac chronotropism and may cause adverse reactions or bronchospasm in individuals with COPD.26 However, we kept individuals who used this medication in our study sample because exercise capacity remained unchanged during β-blocker use in a study by Thirapatarapong et al.26 In their study, individuals with COPD with and without β-blocker medications were compared in a maximum exercise test, and no difference was found in exercise capacity and ventilatory demand among the groups.26 Other studies also included individuals using this medication in their heart rate analysis and demonstrated that there is no influence of β blockers on analyzed outcomes.1,23 Thus, the clinical applicability of our results can be considered more generalizable.
Some limitations are found in this study, such as a small number of individuals classified as GOLD 1 in the analyzed sample, which does not allow the results to be generalized to the entire COPD population. However, these individuals are usually asymptomatic and not many are engaged in rehabilitation services. Moreover, comorbidity assessments were self-reported; although such self-reporting has been widely used, it does not enable a deeper investigation, especially regarding cardiovascular function. Another limitation is the use of pulse oximetry as the method used to evaluate heart rate. There are other ways to analyze heart rate, such as by electrocardiogram, but this modality is more costly and is not found in every rehabilitation clinic. Additionally, although it is known that the recovery heart rate is a predictor of exacerbation in individuals with COPD,4 frequent exacerbators were not included in our sample. Thus, future studies are necessary to verify the behavior of heart rate recovery in those who suffer frequent exacerbations. Despite these limitations, some strengths are also observed, such as the proposition to use a simple field test (6MWT) for heart rate assessment and determination of 1-min heart rate recovery delay. Another strength is the novelty of including objectively measured variables of PADL as a potential factor associated with heart rate recovery, because no previous studies has investigated this to date.
Conclusions
Based on these results, we conclude that individuals with COPD who have a heart rate recovery ≤ 12beats/min in the first minute after the end of the 6MWT have worse exercise capacity, a more sedentary lifestyle, and worse functional status compared to individuals with a recovery > 12 beats/min. Therefore, despite the simplicity of this assessment, heart rate recovery after the 6MWT should be further explored as a promising outcome in COPD.
Acknowledgments
We thank our colleagues from the Laboratory of Respiratory Physiotherapy Research who contributed to this work. Specially, we thank Felipe Machado, Lucas Fava, and Giovana Guzzi for their help in data collection.
Footnotes
- Correspondence: Karina C Furlanetto PhD, Research Center in Health Sciences, University of Northern Paraná, Rua Marselha 591, Jd Piza, CEP: 86041-140, Londrina, Paraná, Brazil. E-mail: ka_furlanetto{at}hotmail.com.
Ms Silva presented a version of this paper at the XVIII Simpósio Internacional de Fisioterapia Cardiorrespiratória e Fisioterapia em Terapia Intensiva, held June 8–11, 2016, in Belo Horizonte, Brazil.
The authors have disclosed no conflicts of interest.
- Copyright © 2018 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}