

Abstract
Although the fundamentals of extracorporeal membrane oxygenation (ECMO) have not changed in 3 decades, the technical elements continue to improve and have evolved from an assemblage of individual components to more integrated systems with added features, enhanced safety, and improved maneuverability. The introduction of polymethylpentene (PMP) fiber technology has expanded the development of artificial membranes that have low resistance, are more biocompatible, and can be used for extended durations. Extracorporeal carbon dioxide removal techniques continue to be enhanced as stand alone technology and modified renal dialysis systems are introduced. Research continues in the development of compact and wearable artificial lungs that are intended to support patients for prolonged periods (eg, patients awaiting lung transplantation). The use of high-fidelity simulation training has become a standard and important method for reinforcing technical skills, refining troubleshooting sequences, and enhancing team interactions. Modifications to mannequins and ECMO systems coupled with clinical and physiologic scenarios will help achieve greater realism and enhance learning. ECMO technology continues to improve, with adaptability and versatility being essential attributes.
- extracorporeal membrane oxygenation
- polymethylpentene
- centrifugal pump
- respiratory dialysis
- decarboxylation
- high-fidelity simulation
Introduction
Extracorporeal membrane oxygenation (ECMO) has been a vital tool in the management of severe cardiorespiratory dysfunction across all patient ages for more than 3 decades. As of 2015, > 78,000 cases have been reported to the Extracorporeal Life Support Organization, and the number of centers reporting to this international database, now exceeding 300 globally, has steadily increased.1 The use of ECMO in adults with cardiac and respiratory conditions has been the category with the largest growth, with > 2,000 cases reported in 2015 and a 57% survival to hospital discharge.1 This growth is supported by ongoing research in techniques including low-flow extracorporeal CO2 removal and variations such as respiratory dialysis and wearable long-term thoracic artificial lungs.2 While the fundamentals of ECMO have not significantly changed, the components that comprise an ECMO circuit have become more integrated and streamlined, are relatively easy to assemble and prepare, and have advanced features and enhanced safety mechanisms.3 The availability of polymethylpentene (PMP) fiber technology has led to a new generation of efficient and low-resistance artificial gas-exchange membranes.4 The development of more integrated and realistic simulation equipment has enhanced interdisciplinary team training.5 The aim of this paper is to review the technical developments in ECMO technology, including devices and techniques that may transition from bench to bedside.
Artificial Gas Exchange
The extracorporeal exchange of oxygen and CO2 occurs by simple diffusion within an artificial lung or membrane oxygenator, which contains bundles of artificial capillaries or hollow fibers that serve as channels for blood, gas, and water.6 Fresh gas is directed into the lumen of the fibers, while blood passes externally and thermo-regulated water flows through adjacent channels.7 These hollow-fiber membranes have been used for several decades in both short-term cardiopulmonary bypass and long-term extracorporeal support. Hollow fibers have typically been constructed of polypropylene, but this material is microporous and, when used for extended periods, it has a tendency to become increasingly hydrophilic due to lipoprotein absorption. This can lead to plasma leakage (also known as plasma wetting), which is the seeping of plasma into the gas compartment of the membrane and can occur within 8 h of use and can affect membrane performance.4,8 Despite this limitation, some ECMO programs have incorporated microporous hollow-fiber membranes into their systems due to their low resistance and ease of preparation, developing troubleshooting steps to replace them when plasma leakage occurred.
Advances in hollow-fiber membrane engineering and design include the use of fibers constructed with PMP, a polymer that has an asymmetric pore structure and outer skin which permits gas permeability but inhibits plasma leakage.4 The brand of fibers principally used to construct today's hollow-fiber membranes is Oxyplus (Membrana, Wuppertal, Germany), now a division of the 3M Industrial Business Group.
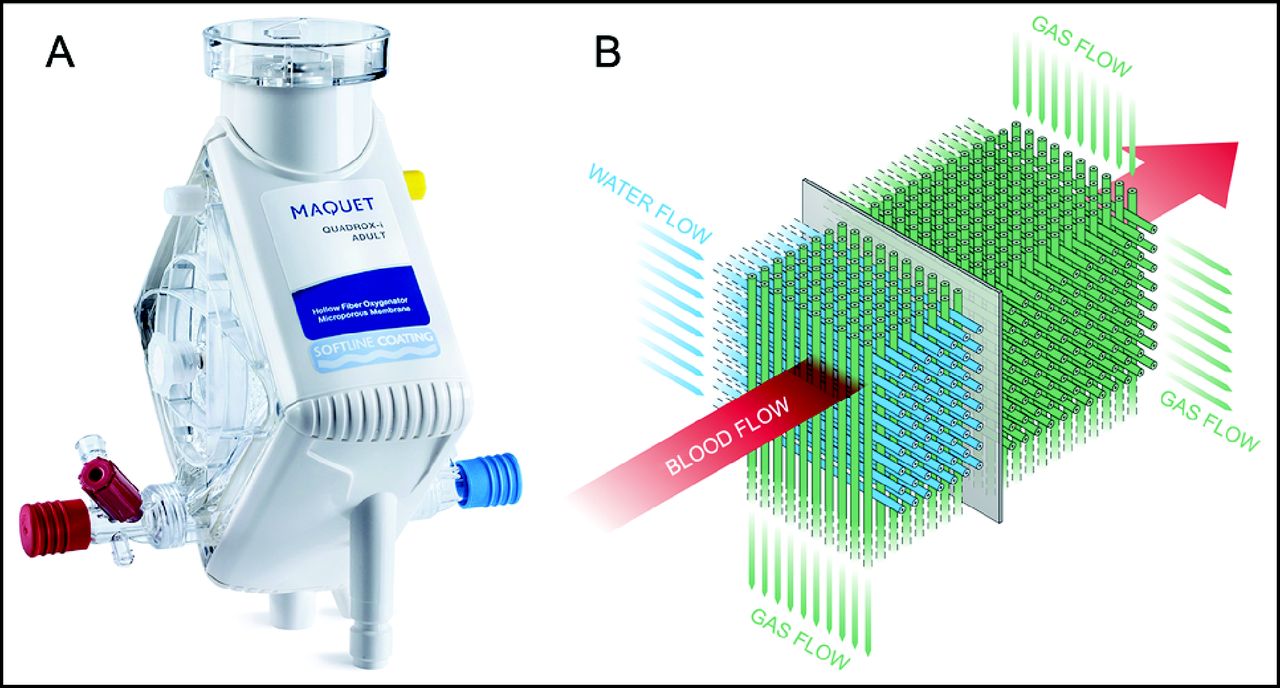
The Quadrox-iD (Maquet, Rastatt, Germany) was the first so-called plasma-tight membrane oxygenator made available in the United States, and it was quickly adopted by ECMO centers (Fig. 1). The architecture of the fiber bundles is a unique interwoven mat with channels for blood, gas, and water running perpendicular to each other. This arrangement of fibers differs from most oxygenators, in which fibers are configured in a winding or spiral pattern with channels running more parallel. Purported benefits of the Quadrox-iD, available in adult and pediatric sizes, include efficient gas and temperature transfer rates, low pressure gradient, ability to rapidly prime and de-air, and integral heat exchanger.

The Quadrox-iD (A) and cross-section of diffusion membrane showing blood, water, and gas flow through a mat of hollow fibers (B). Courtesy of Maquet.
Recently the Medos Hilite LT (Xenios, Heilbronn, Germany), one of the first PMP oxygenators used in Europe, became available in the United States (Fig. 2). This membrane comes in 3 sizes, has a cylindrical shape, and has attributes similar to the Maquet device. Additional devices with equivalent characteristics and gas transfer profiles are also available outside of the United States. Few studies have compared the clinical performance of these oxygenators, with device selection often based on availability and cost. In one study, the Medos Hilite LT was found to have greater oxygen transfer rates and CO2 removal relative to surface area compared to the Quadrox-iD Pediatric.9 This study was insufficiently powered to determine the superiority of a particular device. Other limitations included variable anticoagulation management or other subject factors that may have affected membrane performance.
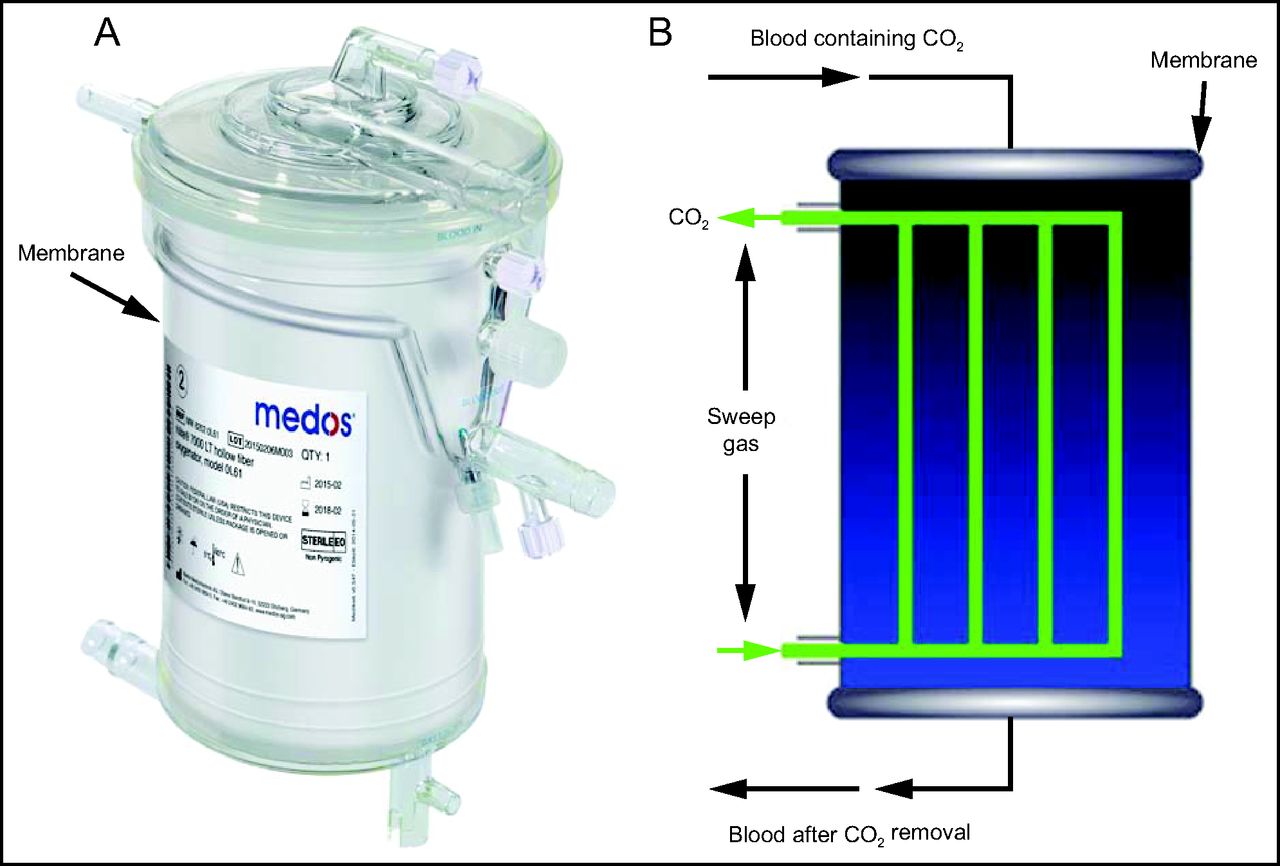
Image of the Medos Hilite LT (A) and diagram of flow through blood and sweep gas channels (B). Courtesy of Xenios.
Contemporary long-term oxygenators marketed as being plasma-tight have been a key advancement in ECMO technology. There is one case report of a plasma-tight membrane experiencing plasma leakage described by Gill et al,10 who observed a collection of fluid at the gas egress of a Medos Hilite LT oxygenator. As this fluid accumulated, an increase in fresh gas flow was required due to retained CO2 and presumed failing gas permeability. Once the membrane was replaced, the gas flow was reduced to previous levels and no further plasma wetting was noted. The oxygenator was investigated by the manufacturer and end users, who found no integrity issues with the fibers. The clinicians speculated that it was the patient's condition that altered the protein layer of the membrane and thus caused the leakage, and they suggested that the oxygenator is microporous under certain conditions.
Eash and colleagues8 conducted an in vitro experiment to determine the extent of plasma resistance and gas permeability in a variety of experimental skinned fibers as well as the clinically used Membrana (ie, Oxyplus). This experiment used techniques to force wetting-out and suggested that fibers which are more plasma-tight had reduced gas permeability, in particular to CO2. The Membrana fibers had the highest degree of wetting-out under these extreme conditions, but the authors concluded that all of the fibers tested had suitable plasma resistance for clinical use. It is not clear whether plasma leakage is a prevalent clinical concern during ECMO, but it should be recognized that while contemporary PMP membranes may be resistant to plasma leakage, they are not necessarily leak-proof.
ECMO Systems
Contemporary ECMO systems incorporate non-occlusive centrifugal pump technology due to the advantages of smaller priming volumes, streamlined circuitry, and potentially less risk of air emboli.11 This style of rotary pump has been used in 60% of pediatric applications despite the debate that it may be more hemolytic than historically-used occlusive roller pumps.11 Current centrifugal pump technology includes pump heads that rotate on a single pivot point, which results in less friction and a more free-floating mechanism with improved flow characteristics and purported minimal blood cell damage. Stand alone centrifugal pumps such as the Rotaflow (Maquet) have been routinely used in ECMO programs in the United States for well over a decade.12
The Cardiohelp (Maquet) is a state-of-the-art miniaturized ECMO system with a uniquely coupled centrifugal pump and PMP membrane (Fig. 3).13 This combined system contains integrated sensors and transducers that provide continuous monitoring of system pressures, temperature, flow, venous oxygen saturation, hemoglobin, and hematocrit. The component is secured to a relatively lightweight driver that controls pump speed, contains various configurations and safety features, and provides a continuous readout of all monitored parameters. The Cardiohelp was initially introduced to the United States market in 2012 and is increasingly being used by ECMO programs.

Cardiohelp, a compact and integrated extracorporeal membrane oxygenation system. Courtesy of Maquet.
In a cohort of 22 adults with respiratory failure, the Cardiohelp was found to effectively correct blood gas-exchange derangements and improve hemodynamics and overall subject stability.14 The authors suggested that the biocompatibility of the circuit would result in fewer thromboembolic complications and lessen the need for blood-product repletion. In 9 of the 22 subjects, the device was replaced due to clot burden in the circuit. Because of the integration of all elements into a single component, an entire circuit exchange is required, which may lead to increased program expenses; in addition, it was noted that the cost of a Cardiohelp device exceeded conventional, less integrated ECMO systems.
The Cardiohelp has been a welcomed advancement in the realm of inter-facility ECMO transport. Its compact size is its principle advantage, but its weight of approximately 9 kg and ease of maneuverability are beneficial features as well. Improved monitoring and safety features during ground and air transport were advantages noted by Philipp et al.15 In a retrospective comparison of the Cardiohelp versus a less integrated ECMO system, Alwardt and colleagues13 described a number of advantages of the Cardiohelp, including less adjunct equipment required, simplified circuitry, a user-friendly interface, and ease of preparation and deployment.
Advances in rotational pump design include diagonal pumps in which the impellers that move blood through the pump head do so in a diagonally streamed manner. One such device is the Deltastream DP3 (Xenios) (Fig. 4).16 Features of this technology include a low prime volume of 16 mL, a compact design, the capability to generate up to 10,000 revolutions/min, and flows to support the full range of patients with an upper limit of 8 L/min (Fig. 4). In a case series of 16 pediatric ECMO subjects, the DP3 was found to be safe and effective and with a low degree of hemolysis.16 The lightweight and compact design of this device has been found to be suitable for inter-facility ECMO transport by helicopter.17

The Deltrastream DP3 pump and driver with Medos Hilite LT hollow-fiber membrane. Courtesy of Xenios.
The versatility of the DP3 system was highlighted in a cohort of 233 pediatric subjects across 7 centers.18 In this series, the DP3 was used for a variety of mechanical circulatory support applications, including venous-venous ECMO, venous-arterial ECMO, and as a ventricular assist device, with indications equally distributed between cardiac and respiratory support. There was a 26% rate of equipment exchanges—membrane or complete system—across the 7 centers and with variable rationales ranging from routine to emergent. This case series demonstrated that the DP3 has multifunctional usefulness, was easy to prepare and handle, and was capable of supporting the full range of mechanical circulatory support indications. In another single-center case series, Speth et al19 supported 27 pediatric subjects and emphasized the device's safety features, such as the ability to prevent retrograde flow, and the system's adaptability.
An additional attribute of the DP3 is the availability of a pulsatile mode. In an in vitro study, the DP3 was shown to produce adequate pulsatile flow across small-bore cannulas typically used in neonates;20 in addition, despite the added resistance of a membrane and circuitry, the DP3 was found to generate adequate pulsatility over a wide range of flows.21 Similarly, pulsatile flow was found to be sufficient in a pediatric model, with greater hemodynamic energy created over the alternate non-pulsatile mode.22 Pulsatile flow may also be synchronized with the patient's electrocardiogram, similar to the mechanisms of an aortic balloon pump.23 An evaluation of this option suggested that the DP3 can produce sufficient pulsatile flow at various simulated heart rates, ratios, and arrhythmias.23 It is unclear whether a pulsatile feature would significantly improve outcomes in patients receiving long-term ECMO support, but when initiating extracorporeal cardiopulmonary resuscitation, it seems that a pulsatile feature could potentially improve coronary perfusion.21 There is also the potential for this mode to lessen the dampening of pulsatility produced by the native cardiac output and improve perfusion to end organs.21
Extracorporeal CO2 Removal
Extracorporeal CO2 removal, also referred to as arteriovenous CO2 removal, is the technique by which an artificial lung is placed between an arterial-to-venous connection typically established through femoral vessels.24 In this pumpless configuration, the patient's native cardiac output provides the driving pressure for blood, which flows through the membrane oxygenator by means of the arterial-to-venous shunt. The aim of this approach is to augment CO2 removal so that lung-protective ventilation can be assured. While pumpless extracorporeal CO2 removal has been shown to improve outcomes in a few case series, it has also been associated with limb ischemia because femoral vessels were principally used.
Pump-driven extracorporeal CO2 removal has emerged as another means of providing effective CO2 removal, and it is typically achieved with a dual-lumen cannula inserted in the right internal jugular or femoral vein.24 One system developed by Novalung (a subsidiary of Xenios) utilizes the DP3 and a PMP diffusion membrane minus the integral heat exchanger; this method is known as interventional lung assist or interventional assist membrane ventilator and is marketed as the Novalung iLA Active (Inspiration Healthcare, Crawley, United Kingdom). This approach was used in 12 adult subjects (6 with hypercapnic lung failure and the remaining with hypoxic respiratory failure) and was found to effectively remove CO2 and correct respiratory acidosis, thus permitting the use of lung-protective ventilation.25 There was a 60% survival rate in this preliminary study, with a pretreatment ventilator duration in excess of 2 weeks associated with non-survival. Generally, this study confirmed that pump-driven extracorporeal CO2 removal can efficiently reduce CO2 levels and lessen ventilator-induced lung injury, but that identification of the ideal candidate for this minimally invasive support will require further investigation.
The variables that control the rate of CO2 clearance during extracorporeal CO2 removal are the fresh gas or sweep gas supplied to the membrane and blood flows. In a small cohort of subjects, CO2 removal was greater when blood flow was held constant and sweep gas was increased as demonstrated by a drop in PaCO2.26 The sweep gas range used was 1–14 L/min, which corresponded to a decrease in the median PaCO2 from 66 mm Hg to 49 mm Hg without any appreciable effect on PaO2. When the sweep gas was held constant at a median rate of 4 L/min and blood flow was increased from 0.5 L/min to 2.0 L/min, there was a similar effect on CO2 removal but a greater effect on median PaO2, which increased from 67 mm Hg to 117 mm Hg. The authors suggested that the use of higher blood flows may require the use of high negative pressure generated on the drainage side of the circuit, which could lead to hemolysis.
One possible benefit of pump-driven extracorporeal CO2 removal is the prevention of intubation and mechanical ventilation and the avoidance of associated complications. In a feasibility and safety study, the Novalung was used in 25 subjects with COPD, of whom 14 did not require intubation.27 Eleven subjects progressed to intubation, 7 primarily due to hypoxemia and 4 for progressive respiratory failure. The extracorporeal CO2 removal cohort was paired with a control group of 25 subjects who received standard treatment. The goal of avoiding intubation was accomplished in half of the study group, and there were no significant differences between the 2 groups with respect to length of stay or mortality.
The Hemolung (ALung Technologies, Pittsburgh, Pennsylvania) is a recent innovation in the field of low-flow extracorporeal CO2 removal.28 This device couples gas exchange and blood flow in a single cartridge and is intended as an adjunct respiratory support for patients with acute hypercapnic respiratory failure (Fig. 5). Blood is distributed to a ring of bundled hollow fibers by means of a rotary pump situated in the core, and sweep gas is pulled through the system by a vacuum mechanism. The cartridge is situated in a driver, which is controlled by a user interface and is arranged as a stand alone device. The system is connected to the patient by a 15.5-Fr dual-lumen catheter that is placed in the internal jugular or femoral vein (Fig. 6). Low blood flows of 300–500 mL/min are used to further augment CO2 removal.29

Hemolung core with rotating pump and fiber bundle (A), cross-sectional diagram (B), and the console and monitoring platform (C). Courtesy of Alung Technologies.

Hemolung 15.5-Fr dual-lumen jugular (A) and femoral catheters (B). Courtesy of Alung Technologies.
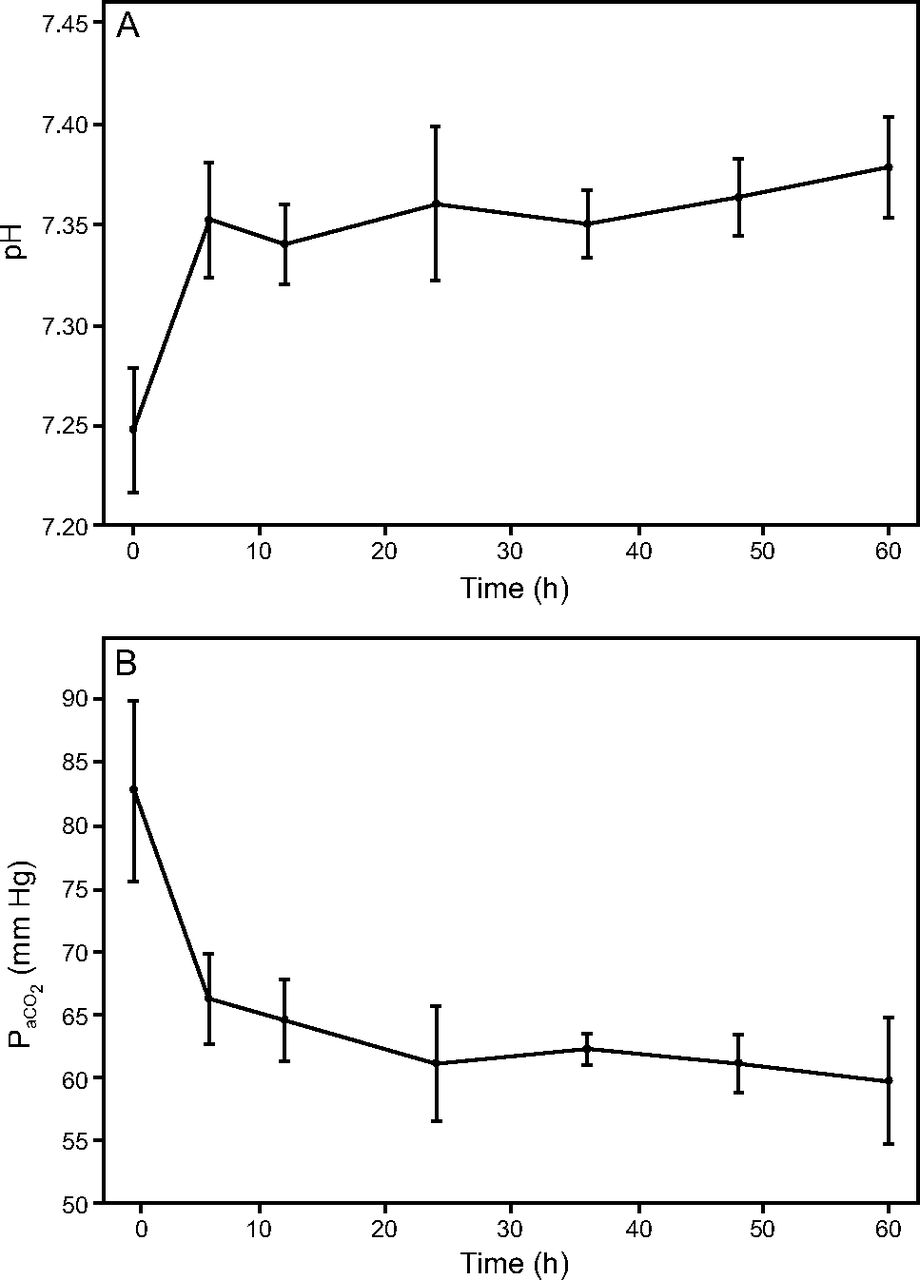
In a small study, 20 subjects with respiratory failure associated with COPD were supported with the Hemolung.30 Prior to initiation of support, the subjects were either receiving noninvasive ventilation, had a high probability of requiring intubation and invasive ventilation or already required invasive ventilation, and had persistent hypercapnic acidosis as determined by a pH < 7.25 and PaCO2 > 55 mm Hg. The dual-lumen catheter was placed in the right internal jugular vein in 13 subjects, and femoral access was used in the remainder. Within 1 h of starting support, PaCO2 levels decreased from a mean of 79 mm Hg to 66 mm Hg, and a corresponding improvement in pH from 7.28 to 7.34 was observed (Fig. 7). The Hemolung consistently removed 80 mL/min of CO2, and complications were mainly related to catheter placement. Intubation was not required in the subjects who were receiving noninvasive ventilation, and overall there was clinical improvement in this cohort. The results of this study confirmed the feasibility of utilizing low-flow extracorporeal CO2 removal with the Hemolung and demonstrated effective CO2 removal. The authors acknowledged that determining the optimal patient population for this modality will require ongoing research, including a randomized, controlled trial.

Changes in mean pH and PaCO2 in subjects with COPD exacerbation receiving noninvasive ventilation. From Reference 30, with permission.
In a small case series, the Hemolung was found to effectively augment CO2 removal in subjects with acute or acute-on-chronic hypercapnic respiratory failure.31 The range of blood flow was 450–550 mL/min and sweep gas was increased to 10 L/min, achieving CO2 removal of 90–100 mL/min. This permitted the reduction of ventilator support as demonstrated by a decrease in peak inspiratory pressure delivered by a ventilator and an improvement in minute ventilation.
Low-flow extracorporeal CO2 removal with the Hemolung was used in a series of adult subjects with moderate ARDS with the goal of achieving ultra-protective lung ventilation, which included the use of tidal volumes in the range of 4–6 mL/kg.32 In this 15-subject series, the Hemolung was connected to the dual-lumen catheter and initiated at a flow of 350–500 mL/min, but the sweep gas was left at 0 L/min. Tidal volumes were then reduced to 4 mL/kg after 2 h, and when hypercapnia occurred (ie, at pH < 7.25 and PaCO2 > 60 mm Hg), the sweep gas was titrated upward to 10 L/min. This strategy permitted the reduction of tidal volumes to 4 mL/kg by correcting the associated respiratory acidosis.
The use of a pump to provide low-flow extracorporeal CO2 removal with devices like the Novalung and the Hemolung has emerged as a viable, safe, and effective means of regulating CO2 removal in patients with hypercapnic respiratory failure such that lung-protective ventilation strategies can be employed. This has been demonstrated in case series, but additional research is needed to determine which population of patients will benefit most from this approach, when in the patients' course it should be used, and the risk-to-benefit ratio given that vascular access and anticoagulation are required.
Respiratory Dialysis
Extracorporeal CO2 removal devices like the Hemolung operate at blood flows similar to those used with hemodialysis and continuous renal replacement therapy (CRRT) systems, and they have been referred to as respiratory dialysis.33 This concept of respiratory dialysis has prompted experiments that utilize CRRT platforms to serve as the pump for the gas-exchange membrane (Fig. 8). Interposing an infant-size Medos Hilite LT membrane (Xenios) onto a standard CRRT device minus the hemofiltration cartridge, Godet et al34 demonstrated sufficient decarboxylation with a 46% reduction in PCO2 and concomitant increase in pH by 0.24. Results of this animal study suggest that CRRT devices may be more readily available and could be modified to provide pump-driven extracorporeal CO2 removal.

Schematic representation of a hollow-fiber membrane positioned in series with a hemofilter with a renal replacement therapy platform. Circles show system pumps and hexagons represent the required pressure sensors. Rep = replacement fluid pump; UF = ultrafiltration pump. From Reference 33, with permission.
Similarly, the Abylcap system, consisting of a Lilliput 2 hollow-fiber membrane (LivaNova, Italy) integrated into the Lynda dialysis system (Bellco Medtronic, Mirandola, Italy), was used to provide extracorporeal CO2 removal in 4 subjects with ARDS by means of a 13.5-Fr femoral catheter.35 Over a 5-d course, PCO2 had decreased by about 38%, permitting a reduction in the median tidal volume from 6.4 mL/kg to 4.8 mL/kg and in plateau pressure from 32 cm H2O to 19 cm H2O. Increasing blood flow from 200 mL/min to 400 mL/min enhanced CO2 clearance with sweep gas flows of 6 L/min. This device was further evaluated in a prospective study of 10 subjects with ARDS who were unresponsive to standard treatment.36 In this study ventilator settings were left at baseline while support was initiated so that short-term effects could be assessed; during this period, CO2 was reduced by about 20%. The device was used for a median duration of 6 d while lung-protective ventilation was provided.
The provision of extracorporeal CO2 removal concomitantly with CRRT has been investigated in the management of patients with multisystem organ failure by positioning a commercial hollow-fiber membrane oxygenator in parallel with the hemofilter of a CRRT system.33 Quintard et al37 applied this strategy in 16 subjects who were receiving CRRT for kidney dysfunction and developed hypercapnic respiratory acidosis. This was accomplished with the addition of a Medos Hilite LT membrane (Xenios) prior to the hemofilter of a Multifiltrate system (Fresenius, Bad Homburg, Germany). In this series, PaCO2 was reduced by 31–39% over a 12-h period, with a pH improvement of 0.23.
This approach was also piloted in a series of 10 subjects with combined respiratory and renal dysfunction utilizing the Polyflux 140 H system (Gambro, Hechingen, Germany) plus a D902 Lilliput 2 membrane (LivaNova, Italy) placed after the dialysis filter, which was described as lung-assisting renal replacement system.38 Blood flows were 250–500 mL/min with sweep gas flows of 4–6L/min, resulting in a 28% decrease in PaCO2 and a corresponding pH increase of 0.12. In addition, subjects had improved hemodynamics as demonstrated by the ability to wean them from vasoactive agents, and there were no technical issues related to the functioning of the CRRT system.
Wearable ECMO
ECMO systems with compact designs and integral components, along with the development of a bi-caval dual-lumen cannula, have extended the use of ECMO to patients awaiting lung transplantation.39 This paradigm shift to longer-term support has prompted a different approach to the clinical management of these patients including liberation from mechanical ventilation, ambulation, and other rehabilitative care.40 There are a number of successful accounts of this approach, which have stimulated interest in developing miniaturized systems that could better facilitate ambulation and movement, and thus potentially extend ECMO duration for other chronic respiratory conditions.41
The portable pediatric pump-lung is a compact, integrated, microporous, hollow-fiber membrane oxygenator and centrifugal pump that weighs approximately 280 g, has a blood surface area of 0.3 m2, and has a priming volume slightly over 100 mL.42 The fibers in the membrane are arranged in a unique circumferential-radial pattern, and the pump is a magnetically levitated rotating impeller driven by a motor. This device was used in a juvenile sheep model to determine whether support could be sustained for 30 d and to assess biocompatibility and gas transfer.42 The pediatric pump-lung was implanted in 8 sheep with the apparatus in a harness on the animal's back. The pump operated at around 2,500 revolutions/min to achieve blood flows of 1–1.5 L/min, and oxygen transfer rates were approximately 50–65 mL/min. Results from this preliminary study are encouraging as support was maintained for 30 d and there was minimal impact on hematologic and blood chemistry parameters. Developers of this device hope to provide an alternative for long-term mechanical circulatory support for infants and children with severe cardiorespiratory failure, as candidacy for organ transplantation is determined.
Additional experiments with the pediatric pump-lung were conducted in a sheep model of acute respiratory failure to further evaluate the gas-exchange capabilities.43 Respiratory failure was induced in 6 animals after placement of the pediatric pump-lung. As soon as hypoxemic and hypercapnic indices of respiratory failure were attained and changes in hemodynamic parameters occurred, blood and sweep gas flow to the pediatric pump-lung was initiated. When support with the pediatric pump-lung was established, blood gas derangements corrected, hemodynamics stabilized, and right ventricular work decreased.
Integrating hollow-fiber membranes with centrifugal pumps greatly reduces the size and priming volume of an ECMO system to a truly compact and wearable size. The paracorporeal ambulatory assist lung, a small device weighing 1.8 kg and with dimensions of roughly 13 × 13 × 13 cm, is being developed for this purpose (Fig. 9).44 The stack-type fiber bundles and the impellers with embedded magnets allow the miniaturized profile. In vitro and in vivo testing has demonstrated that the paracorporeal ambulatory assist lung generated flows of 3.5 L/min at rotational speed of 2,100 revolutions/min and provided sufficient O2 and CO2 transfer.

The paracorporeal ambulatory assist lung prototype. Courtesy of the University of Pittsburgh.
Two pumpless devices intended for long-term use are being developed at the University of Michigan: the M-lung and a compliant thoracic artificial lung.45 The M-lung contains blood and gas paths that pass through a series of fiber-bundle compartments arranged so that blood and gas flow run perpendicular to each other. Computational flow dynamics and in vivo testing of this low-resistance device demonstrated that the mixing of blood as it traversed the gated compartments augmented O2 transfer and sufficiently removed CO2 at a rated flow of 2 L/min.46 The compliant thoracic artificial lung consists of a flexible chamber containing a mat of hollow-fiber bundles through which blood is routed by means of inlet and outlet conduits, while fresh gas flows adjacently.47 Initial animal experiments with this device showed that the load on the right ventricle could be reduced with the device positioned between the pulmonary artery and left atrium, and flows > 7 L/min could be achieved. Additional studies demonstrated that the device could be maintained for 14 d without any appreciable increase in resistance, while maintaining normal physiologic function and with minimal thrombus formation.45 With further refinements and evaluated over longer durations, these thoracic artificial lung prototypes may be a viable alternative for the support of patients awaiting lung transplantation.
Simulation-Based Training
The use of simulation-based training has become a valuable tool in the preparation of medical and surgical teams, enhancing team functionality, safety, surgical technique, and knowledge.48–50 ECMO programs have incorporated simulation-based training into their curricula and as a mechanism for skills enhancement, team development, improving clinical outcomes, and maintaining competency.51–53 The success of simulation-based training is influenced by the technology used to create clinical and physiologic realism for routine and emergency ECMO scenarios.
Modifications to simulation mannequins have been one approach, such as the reusable model proposed by Thompson in which tubes positioned in the neck serve as surrogates for the internal jugular vein and carotid vessels, which are then overlaid with a simulated skin.54 This model was found to sufficiently replicate cannulation steps and bring greater fidelity to the simulation experience, which was perceived to improve team work and participant confidence. Another mannequin modification was reported by Allan et al,55 consisting of an imbedded skills trainer developed in conjunction with cardiovascular surgeons. The haptic trainer was designed to mimic skin and tissue layers such that vessel identification was representative of a real incision and dissection involved anatomic accuracy and bleeding (Fig. 10). Cardiothoracic surgeons participating in an ECMO cannulation skills program using this trainer were found to have improved skills and overall greater proficiency. Similarly, an open-chest model was developed and used to simulate scenarios such as cardiac tamponade and the effect on ECMO flow.56 This system was found to be beneficial to end-users, with enhancement in both skills and communication.

Imbedded haptic skills trainer kit (A) used for surgical placement of extracorporeal membrane oxygenation cannulae during simulation training (B). Courtesy of Dr Peter Weinstock, Boston Children's Hospital Simulator Program.
The modification of simulation mannequins is one step toward greater fidelity in ECMO simulation-based training. Further authenticity could be achieved with the ability to concomitantly alter mannequin physiology and ECMO circuit and system response. Ribeiro et al57 created a realistic model utilizing a harvested porcine heart, a ventricular assist device, and the Califia cardiopulmonary bypass simulator developed by Biomed Simulation (Poway, California). The porcine heart was prepared with surrogate inferior vena cava and aorta, which were mechanized with a ventricular assist device to mimic a beating heart. Additional lines were directed to the Califia simulator, which controlled pressurization of the heart. The heart was placed in the thorax of a mannequin to create an innovative and authentic platform for the cannulation and application of cardiopulmonary bypass.
The EigenFlow (Curtis Life Research, Indianapolis, Indiana) is a stand alone simulator used to create various conditions during ECMO, such as decreased venous drainage, air emboli, or changes to transmembrane pressure. The device is spliced into an ECMO circuit and is remotely controlled through wireless technology, which permits the user to readily alter flow and pressures to create a more dynamic experience with varying degrees of acuity simulated.
The use of mannequin-based simulation training has become prevalent in ECMO centers and is an important adjunct to training methods recommended by the Extracorporeal Life Support Organization.5 The development of ECMO-ready mannequins that can be surgically accessed and programmed to create physiologic and clinical realism remains an unmet need. Devices like the Califia, while aimed at cardiopulmonary bypass simulation exercises, may have a role in creating physiologic variations associated with ECMO and might create a more authentic experience for learners. The coalescence of a mannequin and programmable ECMO system that can be remotely altered may achieve greater realism during troubleshooting sequences and clinical management of an ECMO patient.
Summary
Technical improvements to ECMO components such as plasma-tight PMP diffusion membranes and pump-membrane combinations, along with the development of integrated systems, have allowed for expanded indications and improved safety. It is intriguing to think that less invasive technology can be developed, perhaps into a single compact platform, to which cartridge-type components may be added to manage specific organ dysfunction, such as the combined renal-pulmonary dialysis concept. Ongoing research is needed to determine whether wearable thoracic artificial lungs can move from bench to bedside, along with parallel studies to determine optimal biocompatibility. Identifying target populations through rigorous studies is also needed to determine which technological advancements will enhance wellness and improve outcomes. Enhanced and more realistic simulation-based training can be established with ongoing innovation so that the specialists who manage new devices and the clinical teams who manage the patients will gain even greater proficiency.
Footnotes
- Correspondence: Peter Betit MBA RRT RRT-NPS FAARC, Boston Children's Hospital, Respiratory Care / ECMO Program,300 Longwood Ave, Boston, MA 02115. E-mail: peter.betit{at}childrens.harvard.edu.
The author has disclosed no conflicts of interest.
- Copyright © 2018 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}