

Abstract
BACKGROUND: COPD is a leading cause of morbidity and mortality worldwide. Spirometry is the most common lung function test for diagnosing COPD with a post-bronchodilator FEV1/FVC < 0.70 confirming the presence of the disease. However, diagnosticians appear reluctant to use bronchodilators, which have been linked to the misdiagnosis of COPD. Therefore, we investigated whether the threshold for diagnosing COPD should be modified when diagnosing COPD based on pre-bronchodilator spirometry.
METHODS: Data from 23,433 participants were merged from the National Health and Nutrition Examination Survey (NHANES) 2007–2012. Participants were excluded for having no post-bronchodilator spirometry, for being below the age of 40, and for having asthma or lung cancer. These exclusion criteria resulted in 680 participants being included in the present study. Participants with COPD were defined as those with a post-bronchodilator FEV1/FVC < 0.70. The threshold for diagnosing COPD based on pre-bronchodilator FEV1/FVC was varied while calculating accuracy, sensitivity, specificity, positive predictive value, and negative predictive value.
RESULTS: Diagnosing COPD based on pre-bronchodilator FEV1/FVC < 0.70 contributes to the misdiagnosis of COPD through poor classification rates. By adjusting the threshold and diagnosing COPD based on a pre-bronchodilator FEV1/FVC < 0.66, the overall classification rates increase noticeably, resulting in a 15% increase in accuracy.
CONCLUSION: We suggest a slight adjustment using pre-bronchodilator FEV1/FVC < 0.66 when diagnosing COPD based on pre-bronchodilator spirometry. This approach could prevent cases of misdiagnosed COPD, which can lead to potentially harmful treatment of people who do not have COPD and foregone treatment in patients with COPD.
Introduction
COPD is a chronic lung disease that is characterized by persistent air-flow limitation. COPD is progressive and is caused by a blend of small-airway disease and parenchyma destruction, commonly referred to as emphysema.1 Worldwide, COPD has an estimated prevalence of 210 million.2 It is a leading cause of morbidity, and COPD has even been estimated as the third leading cause of death in 2010.1,3
The most commonly used lung function test in COPD diagnosis and monitoring is spirometry.1,4 According to the Global Initiative for Chronic Obstructive Lung Disease, a post-bronchodilator FEV1/FVC < 0.70 confirms the presence of COPD and is an essential element in COPD diagnosis.1 Post-bronchodilator spirometry is not only required in the diagnosis of COPD; it is also required to assess the severity of COPD because the classification of severity of air-flow limitation in COPD is based on post-bronchodilator FEV1.1 Even though spirometry is known as a simple and inexpensive test that is widely used,1 employing spirometry to diagnose COPD is challenging. COPD misdiagnosis and misclassification has been linked to the threshold for defining obstruction and is widely discussed.5–12 Moreover, COPD misdiagnosis and misclassification may be caused by the use of pre-bronchodilator spirometry instead of post-bronchodilator spirometry. A false positive diagnosis of COPD can lead to harmful treatment for a patient without COPD as well as unawareness of and therefore no treatment for other possible reasons causing the underlying air-flow obstruction. A false negative diagnosis can cause undertreatment in patients with COPD. Such undertreatment may hinder the chance of slowing the progression of the disease at an early stage.13 Thus, it is important that post-bronchodilator spirometry be performed when diagnosing and assessing the severity of COPD in accordance with existing guidelines.1
Although spirometry is the key element in COPD diagnosis, it is still greatly underused.14,15 This is supported by Arne et al,15 who found that post-bronchodilator data were only available for 45% of the newly diagnosed COPD subjects. Moreover, 34% of the subjects with available post-bronchodilator data had a post-bronchodilator FEV1/FVC > 0.70.15 These results are similar to those in a study by Miravitlles et al16 that found that post-bronchodilator spirometry was only performed in 32% of their subjects.
Because a significant number of diagnosticians appear reluctant to use bronchodilators, it is important to establish guidelines for diagnosing COPD based on pre-bronchodilator FEV1/FVC to potentially improve the diagnosis of COPD. Moreover, post-bronchodilator spirometry is not always available, which emphasizes the call for improved guidelines for pre-bronchodilator diagnosis. This study aims to quantify the classification rates when diagnosing COPD based on a pre-bronchodilator FEV1/FVC < 0.70. Additionally, we aim to propose an adjustment to the pre-bronchodilator FEV1/FVC threshold for diagnosing patients with COPD to reduce the misclassification error.
QUICK LOOK
Current knowledge
COPD is commonly diagnosed with spirometry, where a post-bronchodilator FEV1/FVC < 0.70 confirms the presence of the disease. However, COPD misdiagnosis has been linked to bronchodilators being underused. As the use of bronchodilators appears problematic for some diagnosticians, it is important to establish guidelines when diagnosing COPD based on pre-bronchodilator spirometry.
What this paper contributes to our knowledge
This work presents a quantification of the classification rates when diagnosing COPD based on a pre-bronchodilator FEV1/FVC < 0.70. Additionally, an adjustment of the spirometry threshold is proposed using pre-bronchodilator FEV1/FVC < 0.66 for diagnosing patients with COPD to reduce the misclassification error and increase accuracy by 15%.
Methods
The study population is based on data from the National Health and Nutrition Examination Survey (NHANES). The objective of the NHANES survey was to assess the health status and the nutritional status among both children and adults in the United States using a combination of physical examinations and interview-based questions.17 These examinations included a respiratory evaluation with spirometry. NHANES participants whose baseline spirometry results showed a pre-bronchodilator FEV1/FVC ratio below the lower limit of normal (determined from age, sex, weight, height, and race/ethnicity) and/or < 0.70 were asked to repeat spirometry after inhaling a β2 adrenergic bronchodilator medication to open their airways.18
In the present study, data from 23,433 participants were merged from NHANES between 2007 and 2012. As Figure 1 illustrates, 21,869 participants were excluded for having no post-bronchodilator FEV1/FVC (n = 1,564). Age is a known risk factor for COPD; the disease develops predominantly past the age of 4019; thus, 807 participants <40 years of age were excluded (n = 757). Seventy-six participants with asthma (as defined as a “yes” in response to the question “Ever been told you have asthma?”) were excluded (n = 681). Additionally, one participant was excluded for having lung cancer, and thus data from 680 participants were used in the present study.
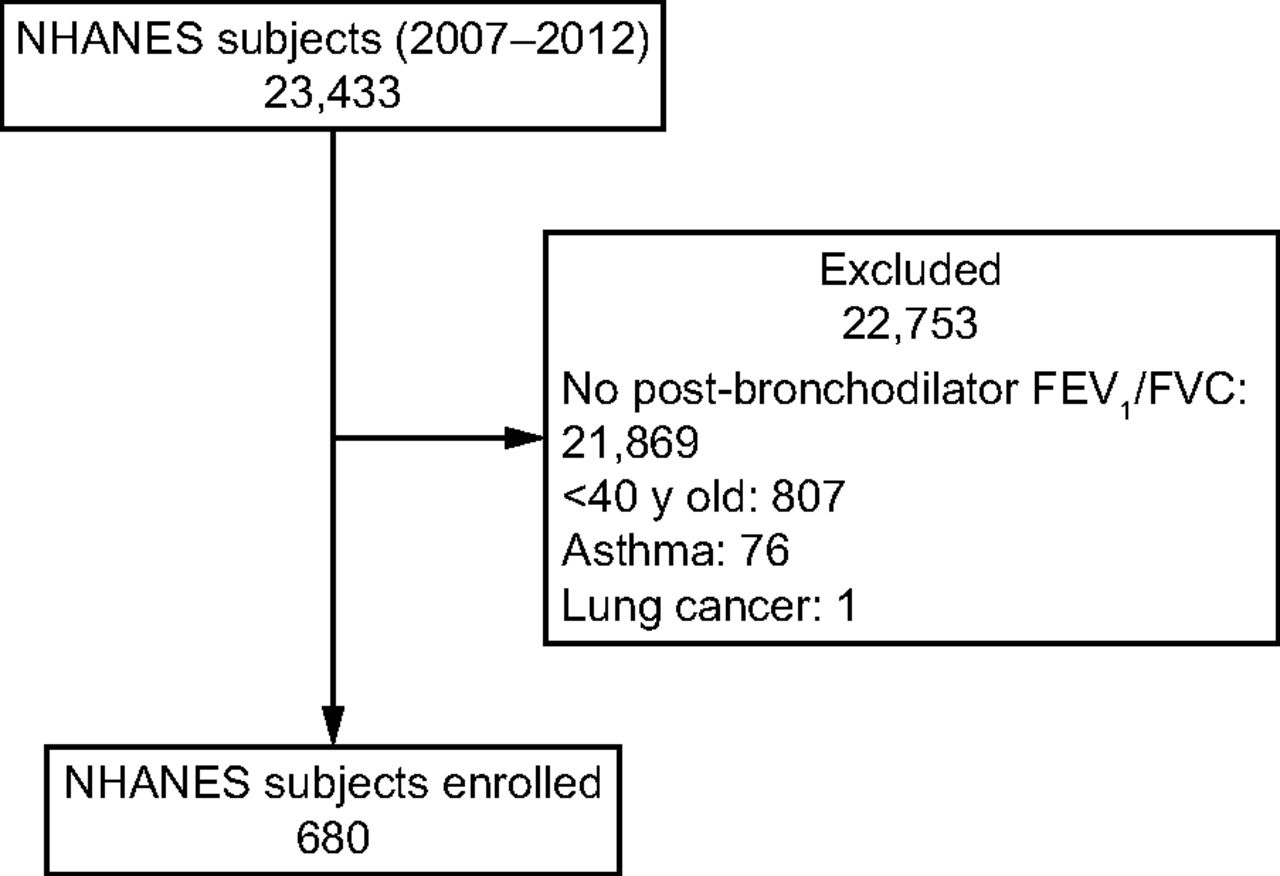
Flow chart. NHANES = National Health and Nutrition Examination Survey.
NHANES developed a comprehensive spirometry manual in which the standardized procedures for execution of spirometry in NHANES were described. This standardization included both the examination protocol itself and quality control and safety procedures. NHANES required that spirometry testing should continue until 3 acceptable tests were approved in which reproducibility criteria were met. The criteria for an acceptable spirometry test included no hesitation/false start, volume of back-extrapolation <5% of FEV1 or 0.15 L, no cough in the first second, exhaled breath lasting a minimum of 6 s, presence of a visible plateau in the volume-time spirogram, and no evidence of leaks, mouthpiece obstruction, etc. The criteria for reproducibility were defined as agreement within 150 mL between the 2 largest FVC and FEV1 values. The test was concluded after a maximum of 8 tests or if the subject was unable to continue.
Participants were diagnosed with COPD using pre-bronchodilator FEV1/FVC and assessed by percent predicted FEV1 based on Knudson et al.20 This diagnosis was then verified as being either true or false using post-bronchodilator FEV1/FVC, the accepted standard in diagnosing COPD.1 To assess the classification rates, the threshold of diagnosis based on the pre-bronchodilator FEV1/FVC was varied while calculating the accuracy, sensitivity, specificity, positive predictive value, and negative predictive value. The threshold for pre-bronchodilator FEV1/FVC for diagnosing COPD was suggested based on the receiver operating characteristic that generated the best combination of sensitivity and specificity.
Results
Table 1 presents the characteristics for the participants included in the present study. Based on the 680 participants, selected from 23,433 participants merged from NHANES between 2007 and 2012, the sensitivity and specificity are higher using a threshold of 0.66 compared with 0.70 (Fig. 2). The accuracy can be increased from 0.64 to 0.79 by diagnosing COPD based on pre-bronchodilator FEV1/FVC < 0.66 instead of 0.70 (Table 2). Sensitivity would then decrease from 1.00 to 0.75, and negative predictive value would decrease from 0.96 to 0.69. Similarly, specificity would increase from 0.10 to 0.86, and positive predictive value would increase from 0.62 to 0.89. For the 680 participants included in the present study, diagnosing COPD based on pre-bronchodilator FEV1/FVC < 0.70 would result in 433 correctly diagnosed cases and 247 misdiagnosed cases (407 true positives, 26 true negatives, 246 false positives, and 1 false negative), whereas diagnosing COPD based on pre-bronchodilator FEV1/FVC < 0.66 would result in 539 correctly diagnosed cases and 141 misdiagnosed cases (305 true positives, 234 true negatives, 38 false positives, and 103 false negatives) (Table 3).
Baseline Characteristics
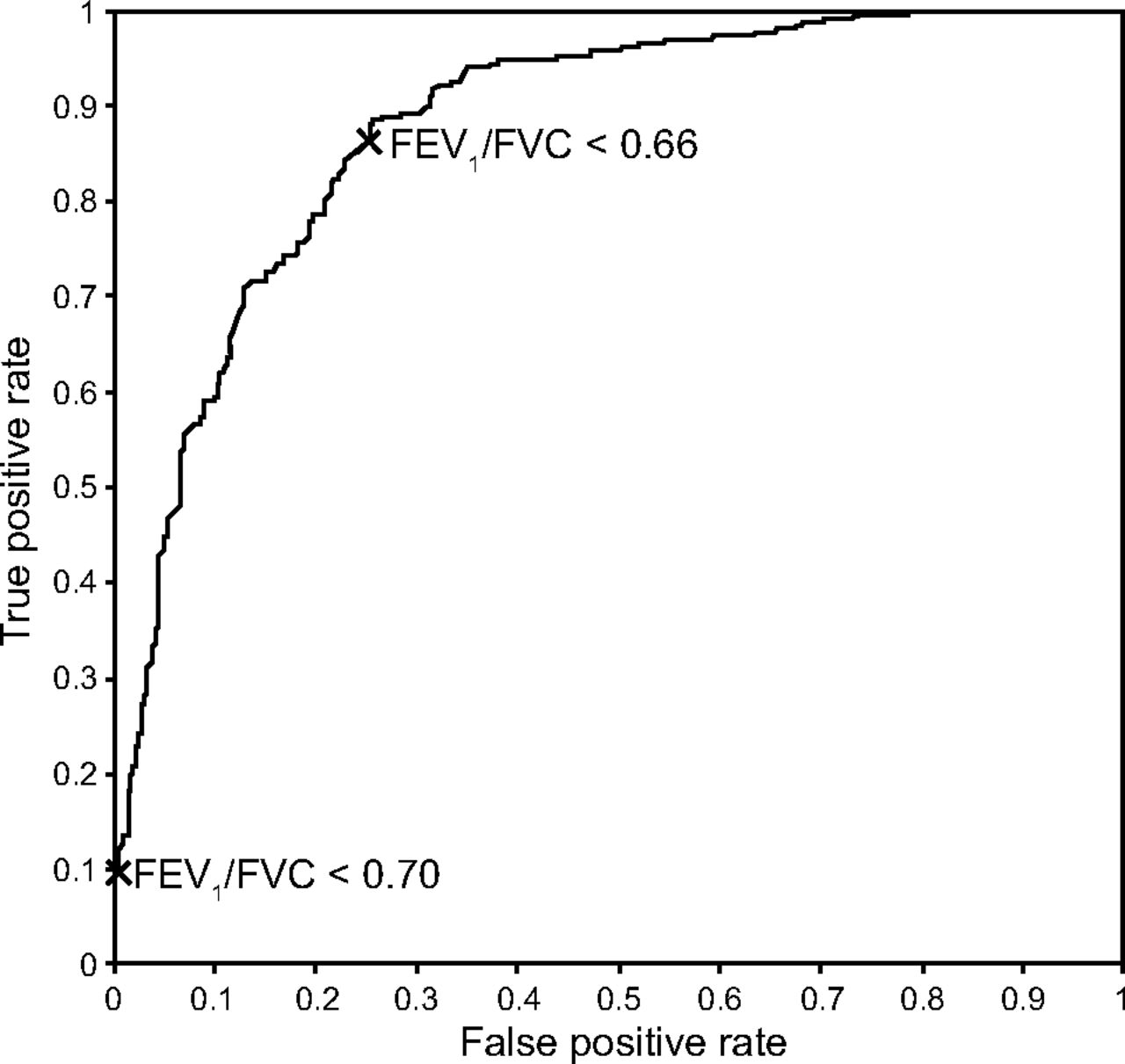
Receiver operating characteristics curve based on varying the threshold of pre-bronchodilator FEV1/FVC when diagnosing COPD. Crosses indicate the thresholds of 0.70 and 0.66.
Classification Rates for a Threshold of 0.70 and 0.66
Confusion Matrices for Diagnosing COPD Based on Pre-Bronchodilator Spriometry
Discussion
The aim of the present study was to quantify the classification rates when diagnosing COPD based on pre-bronchodilator spirometry FEV1/FVC < 0.70 and, additionally, to propose an adjustment of the threshold to reduce misclassification error. Based on the results of the present study, a high sensitivity and negative predictive value of diagnosing COPD based on pre-bronchodilator FEV1/FVC < 0.70 comes at the cost of low specificity and a mediocre positive predictive value, resulting in an accuracy of 64%. A threshold of 0.66 for pre-bronchodilator FEV1/FVC appears to increase diagnostic accuracy. With a slight decrease in sensitivity and negative predictive value, the overall classification rates increase, resulting in an accuracy of 79%, a 15% increase.
As stated initially, COPD is heavily misdiagnosed as a result of the limited use of post-bronchodilator spirometry. The results of the present study clearly support COPD misdiagnosis with low specificity and a mediocre positive predictive value when diagnosing based on pre-bronchodilator spirometry FEV1/FVC < 0.70. The specificity causes a high false positive rate and results in many cases of misdiagnosed COPD. The upside is that all true cases of COPD, as confirmed by post-bronchodilator spirometry FEV1/FVC < 0.70, will be diagnosed using pre-bronchodilator spirometry FEV1/FVC < 0.70 because the sensitivity is 100%.
Using pre-bronchodilator spirometry FEV1/FVC < 0.66 to diagnose COPD, sensitivity was decreased by 25%, and the negative predictive value is decreased by 27%. However, specificity, positive predictive value, and accuracy increased by 76, 27, and 15%, respectively. This approach would result in 15% more correctly classified cases overall (106 cases of the 680 participants included in the present study) and would noticeably decrease the amount of misdiagnosed cases of COPD. The downside is introducing cases of undiagnosed COPD. Of the 103 false negatives, 84 had mild COPD and 17 had moderate COPD based on FEV1. The FEV1 among the false negatives had a mean ± SD of 0.95 ± 0.17, and the lowest observed value of post-bronchodilator FEV1/FVC was 0.63. Therefore, no severe or very severe cases of COPD remained undiagnosed.
Several studies have explored the use of bronchodilator spirometry in COPD diagnosis and assessment. Mannino et al21 concluded that both pre- and post-bronchodilator lung function predict mortality with similar accuracy. These results mirror the findings of Hoesein et al,22 who did not find any significant difference in diagnostic property using pre- or post-bronchodilator, respectively. Johannessen et al23 found that post-bronchodilator testing affected COPD prevalence estimates substantially. However, the predictors of COPD remained unchanged regardless of post-bronchodilator testing. Schermer et al7 found that using pre-bronchodilator testing leads to overestimation of air-flow obstruction. These results are comparable with those of a study by Waheed et al,24 who also found that using pre-bronchodilator testing overestimates air-flow obstruction. Post-bronchodilator testing is proposed to minimize this overestimation. Moreover, Probst-Hensch et al25 concluded that pre-bronchodilator testing may lead to misclassification of COPD. The current study contributes to this discussion by adjusting the pre-bronchodilator threshold rather than comparing pre- and post-bronchodilator prevalence and predictors.
The evidence for using post-bronchodilator testing to assess COPD severity seems inconclusive. Chen et al26 concluded that pre-bronchodilator FEV1 is inferior to post-bronchodilator FEV1 when assessing COPD severity. In line herewith, Fortis et al27 concluded that post-bronchodilator spirometry may be a more accurate predictor of a variety of COPD features and outcomes. Future work should therefore include evaluating the COPD severity stages based on pre-bronchodilator FEV1 before using this in assessment of the disease severity.
The threshold for defining COPD has been discussed extensively.5,6,13,28–33 There seems to be a general agreement that the fixed threshold leads to overdiagnosis of older subjects and underdiagnosis of younger subjects. In their most recent recommendations, the Global Initiative for Chronic Obstructive Lung Disease34 acknowledges the fact that the fixed threshold may lead to more frequent diagnosis of older subjects and less frequent of younger subjects. Lower limit of normal is often recommended as an alternative to the fixed threshold.5,6,28–32,35 However, the fixed threshold remains widely used despite the issues of misdiagnosis. One may assume that this is partly because the fixed threshold is simple to use and easy to understand. Adjusting the fixed threshold to 0.66 for pre-bronchodilator testing may therefore be regarded as a makeshift solution rather than an ideal solution.
There are a number of limitations to this work. NHANES participants until the age of 79 were eligible for the spirometry testing18; participants below the age of 40 were excluded in the present study. Therefore, the results may not apply to individuals who are below the age of 40 or above the age of 79. Data analysis revealed that only 11 participants had a post-bronchodilator FEV1/FVC < 50% predicted. It is reasonable to believe that patients with severe and very severe COPD, with challenges in daily activities, will not volunteer for or are not capable of participating in a comprehensive study, such as NHANES. However, patients with severe COPD have, by definition, a low FEV1 and are therefore expected to have a pre-bronchodilator FEV1/FVC < 0.66 as a result of heavy restriction in the airways.1 The study was also limited by diagnosing COPD solely based on spirometry, as COPD should be considered in any patient who has dyspnea, chronic cough or sputum production, and/or history of exposure to risk factors for the disease.1 However, we did not find NHANES sufficient for differentiating between participants with post-bronchodilator FEV1/FVC < 0.70. Another limitation can be cases with COPD-asthma overlap. These patients represent an important subgroup who are poorly characterized and with worse clinical features than COPD alone.36 Patients with asthma were excluded from this group to minimize confounding the results. NHANES emphasizes that the samples are representative of the United States civilian non-institutionalized population. Therefore, we assume that the results are representative of this population, and one should therefore take precaution when extrapolating the results to populations with different demographics.
Conclusions
Based on the results of the present study, a pre-bronchodilator FEV1/FVC < 0.70 contributes to COPD misdiagnosis and has poor classification rates. Our study suggests adjustment of the threshold using a pre-bronchodilator FEV1/FVC < 0.66 when diagnosing COPD based on pre-bronchodilator spirometry.
Footnotes
- Correspondence: Thomas Kronborg, Fredrik bajers vej 7C, Room C1-219, 9220 Aalborg Ø, Denmark. E-mail: tkl{at}hst.aau.dk.
The authors have disclosed no conflicts of interest.
- Copyright © 2019 by Daedalus Enterprises









{kind=link}
{kind=link}