

Abstract
BACKGROUND: The sit-to-stand (STS) test is a feasible tool for measuring peripheral muscle strength of the lower limbs. There is evidence of increasing use of STS tests in patients with COPD. We sought to evaluate in subjects with COPD the minimum clinically important difference in 30-s STS test after pulmonary rehabilitation.
METHODS: Stable COPD subjects undergoing a 30-s STS test and a 6-min walk test (6MWT) before and after pulmonary rehabilitation were included. Responsiveness to pulmonary rehabilitation was determined by the change in 30-s STS test results (Δ 30-s STS) before and after pulmonary rehabilitation. The minimum clinically important difference was evaluated using an anchor-based method.
RESULTS: 96 subjects with moderate-to-severe COPD were included. At baseline, 30-s STS test results were significantly related to distance covered in a 6MWT (6MWD) (r = 0.65, P < .001), FVC (r = 0.46, P < .001), PaCO2 (r = −0.42, P < .001), FEV1 (r = 0.39, P < .001), and age (r = −0.31, P = .002). After pulmonary rehabilitation, a significant improvement in 30-s STS test results was observed (mean difference +2 repetitions, P < .001). The Δ30-s STS was positively related to Δ6MWD (r = 0.62, P < .001), transitional dyspnea index (r = 0.67, P < .001), and baseline residual volume (r = 0.27, P = .007). The receiver operating characteristic curves method identified a Δ 30-s STS cut-off of 2 repetitions as the best discriminating value (area under the curve: 0.892, P < .001) to identify the minimum clinically important difference for Δ6MWD (30 m). In a multivariate logistic regression model, baseline 30-s STS (odds ratio 2.63; 95% CI 1.09–6.35, P = .031) and diffusing capacity of the lung for carbon monoxide (< 53% predicted) (odds ratio 2.49, 95% CI 1.04–5.98, P = .041) predict the risk to have a Δ 30-s STS ≥ 2 repetitions.
CONCLUSIONS: Our study indicates that in stable subjects with moderate-to-severe COPD, the 30-s STS test was a sensitive tool to assess the efficacy of pulmonary rehabilitation. A Δ 30-s STS of ≥ 2 repetitions represented the minimum clinically important difference, which may be predicted by the baseline ability in the 30-s STS test and lung function in terms of diffusing lung capacity (ClinicalTrials.gov registration NCT03627624).
- COPD
- sit-to-stand test
- minimum clinically important difference
- pulmonary rehabilitation
- physical ability
- diffusing lung capacity
Introduction
Skeletal muscle dysfunction is a clinically relevant extrapulmonary manifestation of COPD1,2; accordingly, resistance training of peripheral muscles has been strongly recommended during a pulmonary rehabilitation (PR) program.3 Resistance training has a greater potential to improve muscle mass and strength than endurance training.4,5 In addition, strength training induces less dyspnea during the exercise period than aerobic training, making this rehabilitative strategy suitable for patients with moderate-to-severe COPD, even during exacerbation.6,7
The sit-to-stand (STS) test is a feasible tool for measuring peripheral muscle strength of the lower limbs. The STS test has been developed for elderly people with different chronic diseases because the maneuver of standing up from a seated position is an essential activity of daily living.8 This ability to stand up from a chair is an important component of maintaining independence among the elderly because this movement depends on stability and balance.9 The STS test can be performed in any health care setting because it requires minimal equipment (eg, a conventional chair and a stopwatch), and it is easy and quick to perform for most subjects.
Variations of the STS test procedure include the maximum number of times a patient can stand up and sit down on a regular chair in a given period of time, usually 30 s or 1 min,10–12 or the time taken to perform a given number of sit-to-stand maneuvers (usually 5 repetitions).13 Moreover, to improve the interpretability and clinical usefulness of field tests such as the STS test, relevant reference values and reference equations have been established.14–17 Previous research reported that scores on the 30-s STS test and the 1-min STS test correlate well with the 6-min walk test (6MWT) and the 1-repetition maximum strength test, which are considered the accepted standard for assessing muscle strength in non-laboratory situations.10–13,18 The minimum clinically important differences for the 1-min STS test and the 5-repetition STS test after PR have been established in stable subjects with COPD.19–21 No study has specifically investigated the minimum clinically important difference of the 30-s STS test after PR. Therefore, we sought to evaluate the responsiveness of the 30-s STS test and to assess the minimum clinically important difference in a large cohort of subjects with moderate-to-severe and clinically stable COPD who were undergoing a PR program.
QUICK LOOK
Current knowledge
The ability to stand up from a chair is an important component of maintaining independence among the elderly because this movement depends on stability and balance. The sit-to-stand (STS) test is a feasible tool for measuring peripheral muscle strength of the lower limbs. The STS test has been developed for different chronic diseases and elderly people. There is evidence of increasing use of the STS test in patients with COPD.
What this paper contributes to our knowledge
The 30-s STS test was a sensitive tool to assess the efficacy of pulmonary rehabilitation in subjects with stable COPD. A change of at least 2 repetitions represented the minimum clinically important difference of 30-s STS test after pulmonary rehabilitation. This minimum clinically important difference may be predicted by baseline ability in the 30-s STS and lung function tests in terms of overall lung capacity.
Methods
Study Design
Stable patients with COPD who were undergoing the 30-s STS test and the 6MWT before and after PR were included. Responsiveness to PR was determined by changes in the results of the 30-s STS test before and after PR. The minimum clinically important difference was retrospectively evaluated using an anchor-based method. Accordingly, on day 1 of the study, we performed a medical evaluation including medical history, physical examination, pulmonary function tests, and blood gas analysis. The next morning, subjects performed a 6MWT and, in the afternoon, a 30-s STS test. Before discharge, subjects repeated these functional assessments. Differences between initial and final values were calculated.
The study was approved by the institutional review board of the Malcantonese Hospital, 6980 Castelrotto, Switzerland. The procedures were performed from September 1, 2016, to August 31, 2017. No additional or external funding was used to support this study.
Subjects
We enrolled 100 subjects with COPD who attended an in-hospital PR program. The majority of subjects were sedentary and homebound. All subjects had a diagnosis of COPD according to Global Initiative for Chronic Obstructive Lung Disease criteria. Patients who had experience an exacerbation within the previous 4 weeks were excluded. Patients who did not complete the PR program due to COPD exacerbation or any unstable medical condition were also excluded. Contraindications for participation in the PR program included musculoskeletal disorders, malignant diseases, unstable cardiac condition, and lack of adherence to the program. All subjects had smoking history ≥ 10 pack-years and received regular treatment with inhaled bronchodilators and inhaled steroids according to current guidelines for their disease stage. Each subject signed an informed consent form.
Pulmonary Function Tests and Arterial Blood Gas Analysis
FVC, FEV1, total lung capacity (TLC), and residual volume (RV) were measured with a flow-sensing spirometer and a body plethysmograph connected to a computer for data analysis (Masterlab, Jaeger, Wurzburg, Germany). The transfer coefficient of the lung for carbon monoxide (KCO) was measured with the single-breath method using a mixture of carbon monoxide and methane (Sensor Medics, Yorba Linda, California). FVC, FEV1 TLC, RV, and KCO were expressed as a percentage of predicted values, which were obtained from regression equations by Quanjer et al and Cotes et al.21,22 FEV1/FVC and RV/TLC ratios were taken as indices of airway obstruction and lung hyperinflation, respectively.
PaO2 and PaCO2 were measured immediately after sampling from a puncture of the radial artery with the ABL 90 Flex gas analyzer (Radiometer, Copenhagen, Denmark).
Sit-to-Stand Test
A straight-backed armless chair with a hard seat was stabilized by placing it against a wall. The height from floor to seat was 47 cm. Seated participants were asked to come forward on the chair seat until the feet were flat on the floor and to fold their upper limbs across the chest. Participants were then instructed to stand up all the way and sit down once without using the upper limbs. Subjects started seated in the chair and, upon command, stood up and returned to sitting as many times as possible in 30 s.
Walking Capacity
Walking capacity was evaluated by means of the distance covered during a 6MWT (6MWD) according to the American Thoracic Society statement.23 The 6MWT was performed by all subjects in a 30-m, level, indoor corridor in the hospital, under the supervision of a physiotherapist, according to American Thoracic Society guidelines. All subjects received the same instructions before the walk and were encouraged by the physiotherapist, who repeated set phrases every minute during the walk. A practice 6MWT was not performed. The 6MWD was recorded in meters. Subjects were allowed to stop and rest during the test but were instructed to resume walking as soon as they felt able to do so.
Pulmonary Rehabilitation Program
According to international recommendations,3 the PR program was completely tailored to suit the needs of the individual. The program consisted of 15 sessions over a 3-week period. To be included in the study, subjects had to complete at least 12 supervised sessions. Lower-limb endurance training was the main component of the PR program. All subjects completed sessions of 30–40 min, using a treadmill or cycle-ergometer, depending on the clinically based choice of the physiotherapist and on the subject's preference. Exercise intensity was based on the initial 6MWT, and subjects started their training at 60–70% of the maximum heart rate achieved on the 6MWT.24 Exercises were then adjusted based on subject tolerance (at least weekly) with the aim of achieving a Borg dyspnea score of 3–5 (moderate to severe). To optimize training load, we provided supplemental oxygen to subjects with chronic respiratory failure and interval training for those who were compromised. Transcutaneous arterial oxygen saturation, blood pressure, and heart rate were monitored during every exercise session. Each session also included supervised upper-limb training; subjects used arm ergometer or performed calisthenic exercises holding a light weight. In relation to the subject's needs, the PR program could also include other components, such as airway-clearance techniques, pursed-lip breathing, and forced expiratory technique, as well as inspiratory muscle training using threshold-loading devices. Finally, each subject participated in educational activities on an individual basis at least 2 times regarding self-management, airway-clearance techniques, adherence to therapy, and nutritional support. The total daily duration of activities was 2–3 h, and the entire program was conducted in the hospital.
Statistical Analysis
A Shapiro-Wilk test was used to analyze whether data were normally distributed. Data were described as median (first quartile, third quartile) for continuous variables with non-normal distribution, and as mean ± SD were used for normally distributed data. Categorical variables were compared using the chi-square test or the Fisher exact test, and continuous variables were compared with the t test or the nonparametric Mann-Whitney test.
Univariate and multivariate regression logistic models (stepwise) were performed to predict the probability of having a Δ 30-s STS ≥ 2 repetitions as the dependent variable. The variables included in the univariate analysis were age, gender (male/female), body mass index, modified Medical Research Council dyspnea scale score (≥2), FEV1 (≤ 50% predicted), the RV/TLC ratio (< 58%), baseline dyspnea index (> 6 points), PaO2 (< 71 mm Hg), PaCO2 (< 39 mm Hg), diffusing capacity for carbon monoxide (DLCO < 53% predicted), baseline 6MWD (< 350 m), and baseline 30-s STS test (< 12 repetitions). For RV/TLC, baseline dyspnea index, PaO2, PaCO2, DLCO, and baseline 30-s STS, median values were used to define categories according to better or worse characteristics.
To evaluate the minimum clinically important difference, Δ 30-s STS after PR was anchored against changes in other outcome measures of PR efficacy.25 The receiver operating characteristic (ROC) curve method26 was used to plot the true positive rate (sensitivity) as a function of the false positive rate (1-specificity) for different cut-off points of the 30-s STS repetitions. The minimum clinically important difference for 6MWD (≥ 30 m) and transitional dyspnea index (≥ 1) were considered as the threshold values.27,28 The 30-s STS cut-off point, which maximized sensitivity and specificity, was chosen as the minimum clinically important difference.
Variables that showed a significant result (P < .10) were included in the corresponding multivariate regression stepwise model. Variables presenting high collinearity (Pearson r > ± 0.30) were excluded from the multivariate analysis. Odds ratios and 95% CI were then calculated. P < .05 was considered significant for all analyses. The analyses were performed with IBM SPSS Statistics 25.0 (Armonk, New York).
Results
96 subjects with moderate-to-severe COPD completed the procedures and were included. Characteristic of the subjects at baseline are reported in Table 1.
General Characteristics of Study Cohort
The main parameters linked with 30-s STS repetitions at baseline were as follows: 6MWD (r = 0.65, P < .001), FVC (r = 0.46, P < .001), PaCO2 (r = −0.42, P < .001), FEV1 (r = 0.39, P < .001), and age (r = −0.31, P = .002).
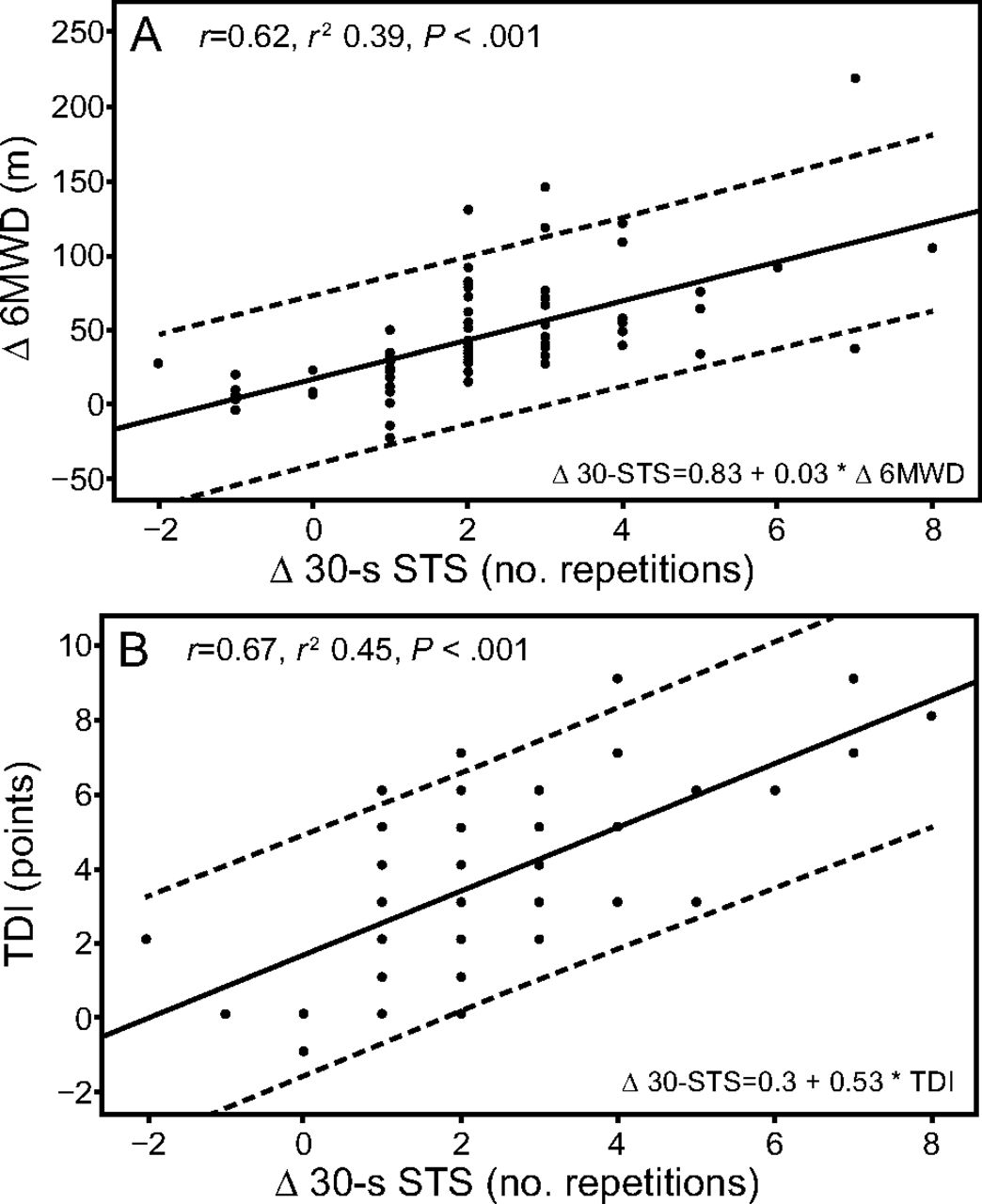
All subjects showed a significant improvement in 30-s STS test results, 6MWD, and transitional dyspnea index after PR (Fig. 1). Notably, a mean difference of 2 repetitions (P < .001) was observed for the 30-s STS tests. The change in 30-s STS test results was positively related to the change in 6MWD (r = 0.62, P < .001), transitional dyspnea index (r = 0.67, P < .001), and baseline RV (r = 0.27, P = .007) (Fig. 2). The ROC curves to identify the best change in 30-s STS test results to distinguish between those achieving the minimum clinically important difference for Δ 6MWD and transitional dyspnea index are shown in Figure 3. According to the ROC curve method, the plots of the true positive rate as a function of the false positive rate for different cut-off points of 30-s STS repetitions with respect to Δ 6MWD ≥ 30 m and transitional dyspnea index ≥ 1, as threshold values, showed 0.907 and 0.885 area under curve values, respectively. The Δ 30-s STS cut-off point, which maximized sensitivity and specificity, was ≥ 2 (0.929 sensitivity and 0.800 specificity, and 0.734 sensitivity and 0.882 specificity, respectively).

Change in A: 6MWD (Δ mean + 42 m); B: BDI/TDI (mean + 3.35 points); C: 30-s STS (Δ mean + 2.07 repetitions) before and after pulmonary rehabilitation. * P value calculated versus value 0 (ie, no change from BDI). 6MWD = 6-min walk distance, PR = pulmonary rehabilitation, BDI = baseline dyspnea index, TDI = transitional dyspnea index, 30-s STS = 30-s sit-to-stand test.

A: Correlation between change (Δ) in 6MWD and 30-STS test before and after pulmonary rehabilitation. B: Correlation between change before and after pulmonary rehabilitation (Δ) in TDI and 30-s STS test. 6MWD = 6-min walk distance, TDI = transitional dyspnea index, 30-s STS = 30-s sit-to-stand.
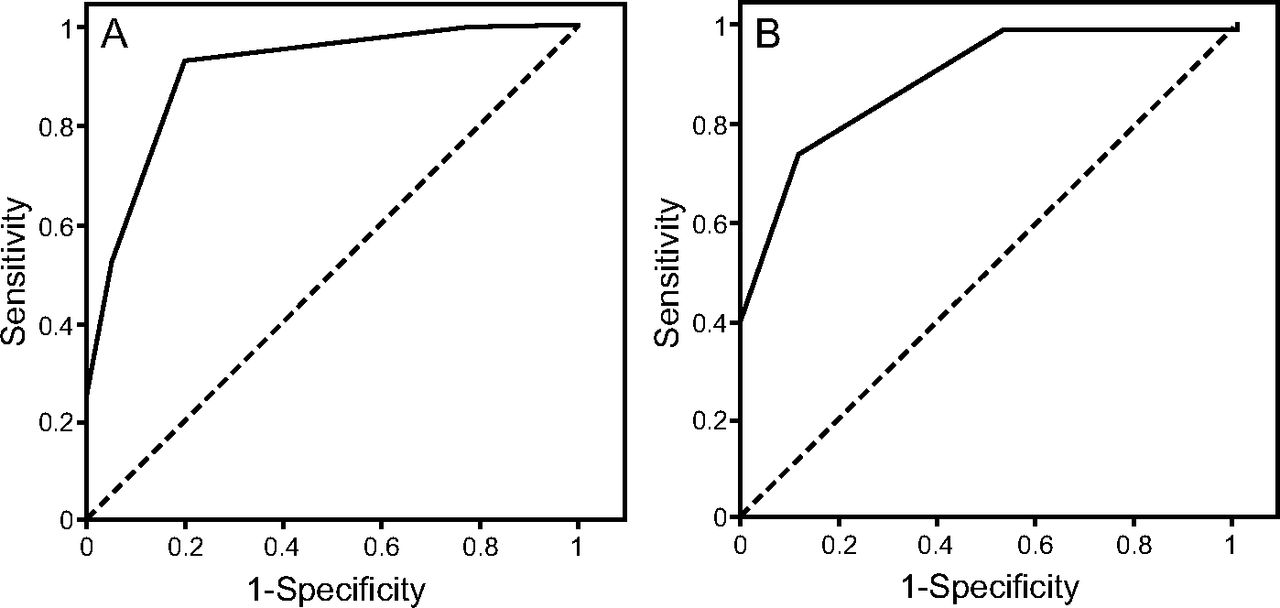
Receiver operating characteristic curves performed with state variables Δ 6MWD (> 30 m) and transitional dyspnea index (> 1 point) to anchor the value of Δ 30-s STS. A: Area under the curve for Δ 6MWD = 0.907, standard error 0.031, 95% CI 0.845–0.968, P < .001, Δ 30-s STS = 1.5, sensitivity 0.929, specificity 0.800. B: Area under the curve for transitional dyspnea index = 0.885, standard error 0.041, 95% CI 0.806–0.965, P < .001, Δ 30-s STS = 1.5, sensitivity 0.734, specificity 0.882.
According to the proposed minimum clinically important difference for Δ 30-s STS, 60 of 96 subjects (62%) improved after PR, showing a Δ 30-s STS ≥ 2. Compared with unchanged subjects in 30-s STS, the improved subjects showed significantly worse respiratory function (air-flow obstruction and diffuse lung capacity), symptoms (dyspnea), and peripheral muscle strength of the lower limbs (30-s STS) at baseline (Table 2). The distribution of subjects with Δ 30-s STS ≥ 2 or < 2, according to the different cut-off of Δ 6MWD (ie, ≤ 30 m or > 30 m) and transitional dyspnea index (≤ 1 point or > 1 point), are shown in Figure 4.
General Characteristics of Study Cohort According to the Cut-Off of 2 Repetitions in the Δ30-s STS Test

Distribution of subjects with Δ 30-s STS (≥ 2 repetitions or < 2 repetitions) according different cut-offs of Δ 6MWD (≤ 30 m or > 30 m) and TDI (≤ 1 point or > 1 point). 6MWD = 6-min walk distance, PR = pulmonary rehabilitation, TDI = transitional dyspnea index, 30-s STS = 30-s sit-to-stand test.
Table 3 shows the results of the univariate and multivariate analyses, taking a Δ 30-s STS ≥ 2 repetitions after PR as the dependent variable, and taking the modified Medical Research Council dyspnea scale score (≥ 2), FEV1 (≤ 50% predicted), 30-s STS baseline (< 12 repetitions), 6MWD baseline (< 350 m), and DLCO (< 53% predicted) as independent variables. Univariate analyses shows that the change in 30-s STS was significantly associated with all of the independent variables, whereas only 30-s STS and DLCO at baseline were associated with Δ 30-s STS in multivariate analyses.
Univariate and Multivariate Analysis Predicting the Probability of a Δ 30-s STS ≥ 2 Repetitions
In a multivariate logistic regression model, < 12 repetitions at baseline 30-s STS (odds ratio 2.63, 95% CI 1.09–6.35, P = .031), and DLCO (< 53% predicted) (odds ratio 2.49, 95% CI 1.04–5.98, P = .041) predict the probability of having Δ 30-s STS ≥ 2 repetitions.
Discussion
In this retrospective study, we investigated the role of a 3-week PR program in improving peripheral muscle strength of the lower limbs as evaluated with the 30-s STS in 96 stable subjects with COPD. As expected, a significant improvement in 30-s STS repetitions in all subjects was found after PR. In addition, we determined a minimum clinically important difference for 30-s STS of at least 2 repetitions, which is able to discriminate between improved and unchanged subjects with COPD, suggesting the potential utility of this parameter in clinical settings. Furthermore, we found that improved subjects, as assessed with the 30-s STS, were characterized by worse respiratory function at baseline and higher changes in 6MWD and transitional dyspnea index after PR.
The STS test was first introduced by Csuka and McCarty29 as a measure of lower-limb strength, and this test remains an important marker of an independent lifestyle. The original version of the STS test required a subject to perform 10 STS repetitions from a standard chair, and the time required to perform 10 repetitions was recorded. Over the years, different versions of the test have been used in different populations. Jones et al30 introduced a version of the STS test conducted over 30 s, which was designed to measure lower limb strength in older adults. Unlike STS tests that involve a 1-min period or 5 repetitions, the 30-s STS test in patients with COPD has not been extensively investigated. In particular, the study by Butcher et al31 reported the validity of this test as a surrogate to evaluate muscle strength by presenting good correlations between the 30-s STS test and quadriceps strength. That study aimed to examine links between muscular performance using different modalities of contraction and functional performance (ie, concentric, eccentric, and isometric contractions).31 In a previous study, we found significant correlations between the 30-s STS test (ie, number of repetitions) and the 1-repetition maximum strength test (ie, the greatest amount of weight lifted in a single repetition), which is considered the accepted standard for muscle strength assessment in the clinical setting.18 We also reported a good correlation between the 30-s STS and 6MWT, which suggests that the 30-s STS test may also be an alternative to the 6MWT to measure functional exercise performance in subjects with COPD.18 Furthermore, we reported a significant improvement in 30-s STS test performance after PR; this is clinically relevant because strength training has a greater potential to improve muscle mass and strength with lower dyspnea grade than endurance training.18
In this study, we confirmed the responsiveness of the 30-s STS test to PR, with a mean difference of 2 repetitions, and we provided the first indication of a minimum clinically important difference in performing the 30-s STS test after PR in subjects with COPD. We reported a minimum clinically important difference that was comparable with the results of Vaidya et al19 and Crook et al,20 which indicated a minimum clinically important difference for 1-min STS; this was interesting considering the difference in the test time.
In addition, we confirmed a significant relationship between lung function and the 30-s STS test results at baseline. Subjects with better preserved pulmonary function had higher lower-limb strength performance. Previous studies showed discordant results. No correlation between pulmonary function, expressed as FEV1, and lower-limb strength performance, as evaluated with a 1-min STS test or a 5-repetition STS test, was reported.10,13 On the other hand, Bernard et al32 found that quadriceps strength, measured during dynamic contractions against a hydraulic resistance, correlated positively with FEV1 expressed as percentage of predicted. Moreover, Seymour et al33 reported that the highest prevalence of quadriceps weakness, evaluated as isometric quadriceps maximum voluntary contraction strength, was found in subjects with COPD with the most severe air-flow obstruction.
When we divided our subjects into 2 groups (ie, improved subjects and unchanged subjects according to the minimum clinically important difference for the 30-s STS test), we noted that those who improved had significantly worse lung function (ie, air-flow obstruction, hyperinflation, diffuse lung capacity) and baseline ability in the 30-s STS test compared to those who were unchanged. Moreover, the improved group obtained a greater change in 6MWD and transitional dyspnea index after PR than the unimproved group. It is possible that subjects with poor baseline lung function are at risk to enter a downward spiral of dyspnea, sedentariness, demotivation, and, finally, deconditioning.34 It is of note that our results showed that these subjects may have a larger improvement after PR compared to subjects with more preserved lung function and exercise capacity.
Regarding the use of various modalities of the STS test, the different procedures do not necessarily reflect the same physical aptitudes, and they are not completely interchangeable. It is reasonable that the shorter versions (ie, 5-repetition STS test, 30-s STS test) are more relevant as an estimate of physical activities that are performed over a short time period, such as strength and speed. In this way, because anaerobic exercise performance is predominant, they provide a measure of deficit in muscle strength and, more precisely, quadriceps weakness.13,31,35,36 In longer versions of STS tests (eg, 1 min or longer), aerobic processes are also involved, making them more suitable to evaluate exercise capacity and tolerance, with a physiological response comparable to that of the 6MWT.20,36 Recently, Morita et al37 compared the 5-repetition, the 30-s STS, and the 1-min STS test protocols and evaluated their correlations with clinical and functional outcomes in a small sample of subjects with COPD. Although all 3 tests were able to identify individuals with low exercise capacity or preserved exercise capacity, the study reported that the 1-min STS test correlated better with clinical outcomes in subjects with COPD, even if it generated higher hemodynamic demands.37 In line with these findings, we reported in a previous study that the 1-min STS test induced a higher fatigue perception and greater oxygen desaturation in subjects with COPD compared to the 1-repetition maximum strength test.18
Despite reporting original findings with potential clinical importance, this study has some limitations. We acknowledge that the STS test does not necessarily evaluate lower-limb strength performance, but it may be an indicator of balance, postural control, mobility, or even cognitive and psychological status as observed in older people.9 Moreover, the retrospective design might limit the validity of the results obtained. Thus, further prospective studies are required.
Conclusion
We report that in stable subjects with moderate-to-severe COPD, the 30-s STS test was a sensitive tool to assess PR efficacy. Furthermore, a change of at least 2 repetitions in the 30-s STS test results represented the minimum clinically important difference, which may be predicted by baseline ability in the 30-s STS and lung function tests in terms of overall lung capacity.
Footnotes
- Correspondence: Andrea Zanini MD, Clinica di Riabilitazione Ente Ospedaliero Cantonale, Via Drive E Schwarz 6, 6986 Novaggio, Switzerland. E-mail: andrea.zanini2{at}eoc.ch.
The authors have disclosed no conflicts of interest.
- Copyright © 2019 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}
{kind=link}