

Abstract
Ventilator-associated pneumonia (VAP) is a well-known complication of invasive mechanical ventilation in critically ill patients. The presence of an endotracheal tube (ETT) is one of the major culprits for VAP development: air flow moves pathogens toward the distal airways, while clearance of the trachea is blunted due to reduced tracheal ciliary movement and impaired cough. Several measures are recognized as being useful to prevent VAP, and these are usually grouped in a VAP bundle (ie, avoiding intubation or re-intubation whenever possible; head of bed elevation; hand hygiene; shortening ventilation through sedation interruptions, spontaneous breathing trials, or thromboembolic prophylaxis). However, other interventions have been proposed to reduce VAP rate; some of these interventions have been reported in large clinical trials to be effective, some have been evaluated in small observational studies, and still others at a pre-clinical stage. Some strategies aim to improve the ETT design via a subglottic drainage system, with treatment of the ETT surface to reduce pathogen activity, or by modification of the cuff shape or cuff material to provide a better seal. Another proposed strategy is improving airway care through control of cuff pressure, cleaning the ETT, or use of closed suction systems. Other interventions target a patient's position in the bed to reduce aspiration of digestive content in the airways, or the use of probiotics to modulate gastric flora. Some of these measures are supported by strong evidence, but the impact on relevant outcomes such as duration of ventilation or mortality, as well as cost-benefit ratio, is still unclear, resulting in lack of widespread use.
- ventilator-associated pneumonia
- endotracheal tube
- airway care
- secretion removal
- cuff
- coating
- preventive measure
- biofilm
Introduction
Ventilator-associated pneumonia (VAP), conceptually defined as pneumonia occurring after 48 h of invasive ventilation, is a common complication after intubation of critically ill patients.1 Knowledge of VAP prevention measures is increasing, and reported rates of VAP are decreasing; however, some investigators believe that such a decline is due to inadequate reporting, and that VAP incidence remains stable.2,3 Moreover, a unique VAP definition is not available because pneumonia itself is difficult to define, and the VAP diagnostic criteria are still under debate.4 In 2013, new criteria for complications related to invasive ventilation were established, relying on the concept of ventilator-associated events, distinguishing between VAP and other forms of ventilator-associated conditions.5
The presence of an endotracheal tube (ETT) is probably the most relevant factor responsible for VAP development. Pathogens are moved in the trachea either by microaspiration around the ETT cuff or by biofilm build-up on the ETT internal lumen; air flow and gravity tend to move pathogens toward the distal airways, and host defense mechanisms such as tracheal cilia movement and cough reflex are blunted by the ETT itself.6 Because the presence of the ETT is often unavoidable in critically ill patients, VAP prevention is based on limitation of the complications associated with medical treatment.
Several measures are generally accepted and widely applied to prevent VAP: avoiding intubation or re-intubation when possible; head of bed elevation; hand hygiene; and shortening ventilation through sedation interruptions, spontaneous breathing trials, or thromboembolic prophylaxis.7–9 Other measures widely used, such as stress ulcer prophylaxis or oral care with chlorhexidine, are still debated.10,11 Some authors suggest reducing gastric acid suppression to limit orodigestive pathogen colonization, and others propose mouth care with chlorhexidine concentration up to 2% to effectively decontaminate the oropharyngeal space.12,13
Grouping several measures in a VAP-prevention bundle is associated with a reduction in VAP incidence; moreover, VAP occurrence is inversely associated with adherence to a bundle.14–16 Whereas VAP bundles appear effective in reducing early-onset VAP (occurring within 5–7 d), late-onset VAP seems associated with patient severity and is thus more difficult to prevent.17
The occurrence of VAP has been associated with several pathophysiological mechanisms, but a simplified paradigm is based on the presence of pathogens penetrating the lungs from within the ETT and around the ETT cuff, mainly from the digestive tract.18 Preventive measures are usually based on the reduction of pathogen burden from one or both of the two reservoirs. In the present review we will focus on specific non-pharmacologic interventions for VAP prevention.
Methods
We performed an online query of PubMed for records published from January 1, 2016, to April 22, 2019 using the following key words: ventilator-associated pneumonia prevention (448 records), VAP prevention (242 records), preventing ventilator-associated pneumonia (72 records), microaspiration pneumonia (34 records), endotracheal tube biofilm (34 records), endotracheal tube cuff leakage (12 records), for a total of 842 records. After duplicates were removed, there was a total of 541 screened records. We limited the research to articles in English and focused on specific nonpharmacologic VAP-prevention measures; review articles, retrospective studies, educational or epidemiological studies, reports of bundles effects, and pediatric studies were excluded. At the end of the screening process, 41 studies were identified. A summary of the available measures and literature update corresponding to the search criteria is provided in Table 1.
Summary of Available Measures and Literature Update Corresponding to the Search Criteria
Modified ETT Design
The presence of an ETT is a major cause of alteration of airway physiology. Therefore, modifications of the ETT design have been studied to prevent VAP, mainly focused on the presence of a subglottic secretion drainage system, treatments of the surface of the ETT, and modified cuff shape or materials.
Subglottic Secretion Drainage System
Secretions hailing from the oropharynx or the digestive tract tend to accumulate in the glottis above the cuff. Because the cuff seal is not perfect, secretions can leak into the trachea and may contribute to pathogen transport within the lungs. Recent evidence suggests that subglottic secretions containing mucin impair neutrophil activity against bacteria, exposing the host to an increased risk of infection.19 Subglottic secretion drainage systems are designed to remove subglottic secretions through a dedicated port just above the cuff, preventing drainage of orogastric secretions into the trachea. In a multi-center study, > 300 subjects were randomly intubated with or without an ETT equipped with a subglottic secretion drainage system; the VAP incidence was reduced in the treatment group compared to controls, and prevention was effective for both early-onset and late-onset VAP.20 Another randomized trial involving 352 subjects showed a nearly 10% reduction in the rate of VAP in the group treated with an ETT equipped with a subglottic secretion drainage system, despite the use of a VAP bundle in both groups; instead, the incidence of ventilator-associated conditions did not differ between the two groups.21 In smaller studies, the use of an ETT equipped with a subglottic secretion drainage system alone or combined with either frequent cuff pressure monitoring or a tapered cuff shape was associated lower incidence of VAP.22–24 Other small studies have failed to show a reduction in VAP incidence with subglottic secretion drainage, possibly due to insufficient statistical power.25–27 A meta-analysis confirmed the association between the use of a subglottic secretion drainage system and reduced VAP occurrence; the effect may be mediated by lower incidence of Gram-positive VAP.28,29 A small clinical study reported that continuous subglottic aspiration may carry a possible advantage over intermittent aspiration.30
A different design for secretion drainage is the mucus slurper, an ETT equipped with several holes on its tip connected to vacuum to remove secretions coming from the glottis or the trachea or secretions that have accumulated close to the ETT tip.31 Data on the clinical efficacy of the mucus slurper system are lacking.
Treatment of ETT Surface
ETTs are usually made of polyvinyl chloride (PVC) and, soon after intubation, its internal surface is covered by a layer of biofilm composed of a glycocalyx matrix and different microbial species.32 The surface of the ETT surface can be treated in an effort to prevent biofilm formation by reducing microbial adhesion or growth. Different types of antimicrobial coatings have been studied in vitro, although silver is the most studied antibacterial agent in the clinical scenario.33 A large randomized clinical trial reported that silver-coated ETTs were effective in preventing VAP; a smaller clinical trial showed reduced ETT colonization and thinner biofilm using ETTs coated with silver sulfadiazine.34,35 A recent preclinical study reported reduced colonization in ETTs coated with a hydrogel film eluting ceragenin CSA-131, a non-peptide small molecule mimicking innate immune defense antimicrobial peptides.36
Another approach to prevent biofilm growth without the use of coatings is to alter the PVC surface of the ETT's internal lumen. ETTs are modified creating grooves or roughness on their inner surface; the hypothesis is that altered PVC physical properties could lead to reduced microbial adhesion or could facilitate secretion movement. In a preclinical study, the PVC surface of an ETT was micropatterned with ribs of micrometric size; the use of a diamond-shape micropattern texture inspired by the skin of a shark (Fig. 1)37 reduced the amount of biofilm within the ETT.38 Similarly, the biochemical formation of nano-roughness on the ETT surface prevented growth of bacteria such as Staphylococcus aureus or Pseudomonas aeruginosa in bench studies.39,40 The use of nanoparticles on the ETT surface (either eluting titanium or eugenol) showed antibacterial activity in a recent in vitro study, but clinical use still requires further investigation.41,42 While micro- and nano-modified ETTs are still under development, the use of silver-coated ETTs for VAP prevention is supported by evidence, albeit limited, and might be cost-effective.43,44

Scanning electron micrograph of Sharklet micro-patterned acrylic material. The scale bar in the micrograph represents 20 μm. From Reference 37, with permission.
Cuff Shape and Material
The main function of the ETT cuff is to seal the trachea and thus allow adequate ventilation and prevent leakage of orodigestive fluid from the glottis. The surface of a standard, PVC, high-volume, low-pressure cuff forms small folds when it comes in contact with the tracheal wall after inflation. An adequate seal depends on the interaction between the cuff and the trachea; the more the cuff adapts to the trachea without folds, the better the seal.
Standard cuffs showed leakage of fluid below the cuff in several bench studies; application of PEEP and proper cuff inflation, as well as use of a lubricant before intubation to reduce the formation of folds, might improve cuff sealing.45,46 A postmortem study showed that a standard mouth cleaning maneuver is not associated with leak of antiseptic solutions in the trachea, but a small amount of fluid gathers above the cuff and cannot be removed by oral suction, and may possibly move downward with time.47 Therefore, improved cuff design and materials were studied to improve sealing of the trachea.
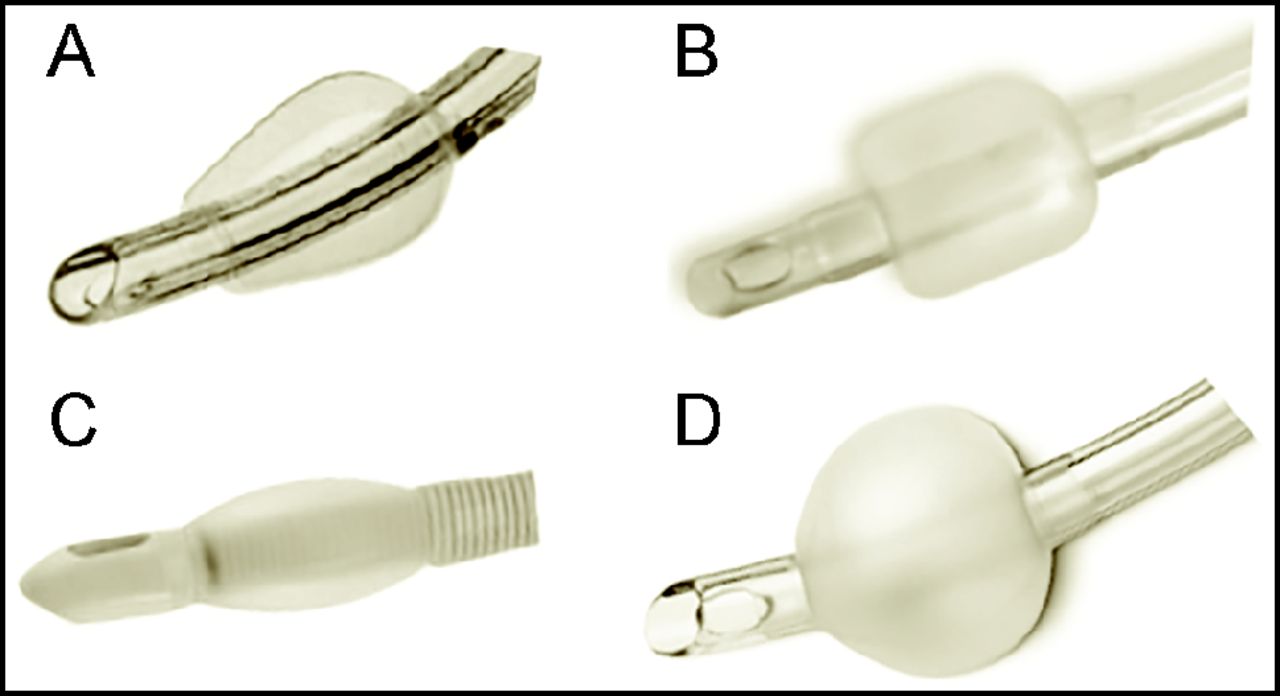
The standard cuff shapes are spherical or cylindrical (Fig. 2); other cuff designs, intended to improve the seal (eg, tapered, double-cuff, double layer) have been studied.48 An in vitro study comparing several ETTs with different cuff shapes and materials showed that cuff length and outer diameter, as well as cuff pressure (see below), were the only determinants for proper sealing.49 The most studied cuff shape is the tapered one, which has exhibited better sealing in an animal study carried out ex vivo on tracheal-lung blocks.50 However, several clinical studies failed to show any benefit from a tapered cuff in VAP prevention; a recent randomized study comparing spherical or tapered cuff tubes, which enrolled 109 postoperative vascular surgery subjects, did not report differences in pepsin microaspiration or in VAP rate.51 A large randomized trial by Philippart et al52 included 604 subjects in 4 parallel groups to study both the effects of the tapered design and the use of polyurethane (see below) cuffs; the tapered cuff design did not reduce tracheal colonization or VAP rates. Another recent, large, clinical trial failed to show reduction of gastric content aspirations or VAP rate in the group of subjects intubated with a tapered cuff ETT; however, tracheal colonization was lower than in the control group.53 Finally, 2 meta-analyses did not support the use of tapered cuffs for VAP prevention.54,55

Different shapes of the endotracheal tube cuff: (A) tapered, (B) cylindrical, (C) pressure-limited, (D) spherical.
Standard cuffs are made of PVC; the use of different materials specifically studied to prevent the formation of folds, such as polyurethane, Lycra, or silicone, showed less leakage in bench tests.56 The use of a polyurethane cuff produced less tracheal injury in a preclinical study; moreover, several clinical studies showed that polyurethane cuff use was associated with less leakage of fluid from the glottis, reduced microaspirations, and lower rates of postoperative pneumonia.57–60 However, the aforementioned large randomized trial by Philippart et al52 failed to show any benefit in VAP prevention when using polyurethane cuff ETTs, as did a small randomized trial in postoperative subjects.61 A complex theoretical and bench study described the optimal cuff dimensions and material properties to be used for human tracheal sealing without wall injury.62 The use of a very compliant material such as silicone allowed the design of a pressure-limited cuff, sometimes referred to as a low-volume low-pressure cuff, to be inflated at high intracuff pressures but limiting the external pressure on the tracheal mucosa, based on the original design described by Young et al63 over 20 years ago. The silicone pressure-limited cuff showed no leakage in bench studies, but in some cases the external pressure slightly exceeded the limit of 30 cm H2O at the recommended inflating pressure.64,65 No leak of blue dye was recorded with the silicone pressure-limited cuff in anesthetized subjects, and leakage was present but lower than controls after intentional manipulation of the ETT.66 A randomized trial in cardiac surgery subjects showed a reduced rate of VAP using an ETT equipped with a pressure-limited cuff and a subglottic secretion drainage system; endotracheal tube colonization tended to be reduced in the treatment group.67,68 A different approach to seal the trachea is the use of no-cuff ETTs, based on the original concept described by Kolobow et al69: the seal is achieve with several thin plastic discs (ie, gills) attached in series close to the ETT tip; an ex vivo animal study exhibited a better seal with the “baffled” ETT than with standard ones.69,70
Airway Care
Cuff Pressure
If the seal in the trachea is not optimal with properly inflated standard cuffs, the probability of fluid leakage from the glottis is even higher when the cuff is not properly inflated (ie, internal pressure < 20 cm H2O).71 Current guidelines recommend manual adjustment of cuff pressure to prevent underinflation, without a definite timing for monitoring. A recent large randomized trial failed to show any benefit from frequent (ie, ≥ 3 times/d) monitoring of cuff pressure as compared to infrequent monitoring (only when clinically indicated).72 Because standard care is not adequate to maintain a tracheal seal, electronic devices have been developed to continuously control cuff pressure, resulting in less time spent with an underinflated or overinflated cuff.73–75 The use of a device for continuous control of cuff inflation pressure was associated with reduced gastric microaspirations, tracheal colonization, and VAP rate; a small meta-analysis replicated these findings.76,77
An alternative approach to maintain cuff pressure as low as possible while preventing aspiration is based on the measurement of minimal CO2 leaks from the trachea in the subglottic space. The system is designed to operate with a modified ETT equipped with a specific port ending in the subglottic space for CO2 sampling, and it is associated with an improved subglottic secretion drainage system. In animal models, leakage of CO2 across the cuff of < 2 mm Hg measured in the subglottic space was associated with an optimal seal, while higher CO2 levels were associated with leakage of dye in the trachea; in the clinical scenario, inflating the cuff with a CO2 leakage of 2 mm Hg was associated with lower filling pressures compared to standard care.78 In two recent randomized feasibility trials, the CO2-based system prevented under- and overinflation without significant adverse events.79,80 Whether the use of a CO2-based cuff monitor results in VAP prevention remains to be elucidated.
ETT Cleaning
Shortly after intubation, secretions gather within the ETT forming a biofilm, thicker toward the tip of the tube, possibly leading to spread of bacteria in the lungs due to airway flow and to other consequences such as increased resistance or total ETT obstruction.81 Few devices were studied to maintain the ETT clear of secretions and limit biofilm growth; the first prototype described was the mucus shaver, an inflatable balloon used in a Fogarty-like maneuver (ie, inserting a catheter with a deflated balloon on its tip, inflating the balloon, and then retracting the catheter) within the ETT.82 A small randomized clinical trial showed lower ETT colonization and reduced biofilm thickness in the treatment group.83 The clinical use of similar devices resulted in lower ETT resistance in vivo84,85 and preserved ETT patency at extubation.84,86 The use of the mucus shaver might also prevent the loss of antimicrobial activity of tube coatings, as demonstrated by preclinical data; however, a recent small clinical trial conducted with a similar cleaning device failed to show any benefit.87,88 In summary, current evidence support the use of an ETT cleaning device to preserve patency and possibly facilitate weaning by reduced airway resistance; a direct impact of VAP rate is still to be demonstrated.
Closed Suction Systems
Tracheal suction is necessary to prevent biofilm from blocking the ETT. The standard open suction maneuver requires the patient to be disconnected from the ventilatory circuit, whereas the use of closed suction systems allows suction without disconnection. Because disconnection from the ventilator may result in the contamination of patient's airways, the use of closed systems might prevent the development of pneumonia. A meta-analysis suggested a possible VAP-preventive effect when closed systems are used, but the evidence was not strong enough to provide a definitive recommendation.89 However, the closed systems offer many advantages other than possible VAP prevention, such as the possibility to remove secretions while PEEP is maintained, and therefore their use appears reasonable in the critical care scenario.
Other Interventions
Position
Ventilated patients are usually maintained in a semi-recumbent position (> 30 degrees) in the bed. The rationale for elevating the head of the bed is the prevention of vomiting and thus the reduction of gastric content leak within the airways of an intubated patient. A recent Cochrane review90 confirmed that the semi-recumbent position is superior to the supine position (0 degrees) for prevention of clinically suspected VAP, although there is a lack of evidence regarding microbiologically documented VAP. A randomized trial showed reduced VAP incidence using a special bed able to rotate a patient's thorax laterally, continuously alternating the rotation side; the measure appeared to be cost-effective in a recently published analysis.91,92 Alternative positions such as the lateral-Trendelenburg position were proposed to prevent VAP because when the head of the patient is lower than the airways, vomiting does not result in the leak of gastric material within the airways and tracheal secretion clearance is improved. A randomized clinical trial93 showed a reduced VAP rate in the lateral-Trendelenburg group; however, the trial was prematurely stopped due to lower overall VAP incidence and increase of adverse events in the treatment group. Moreover, an animal study showed increased brain injury in the Trendelenburg position, raising concerns about its safety.94 An ancillary study of a large randomized trial on the use of prone position for ARDS treatment showed no difference in VAP rate between the prone and the semi-recumbent position.95 Therefore, current evidence does not support any position other than the semi-recumbent position for the ventilated patient.
Probiotics and Nutrition
Because one of the recognized VAP pathways is the inoculation of lungs with pathogens hailing from the oropharynx, the reduction of pathogen colonization within the orogastric space has been proposed to reduce VAP rate. The modulation of orogastric flora by administration of probiotics containing nonpathogenic bacterial species was associated with lower VAP incidence in a randomized clinical trial involving > 200 critically ill subjects,96 as confirmed in a recent meta-analysis;97 however, mortality and duration of ventilation were not affected. A recent double-blind randomized trial showed an association with lower VAP rate in the probiotic group.98 Larger randomized trials are needed to provide definitive recommendations regarding the use of probiotics in critically ill patients. An ancillary analysis of a randomized trial comparing enteral and parenteral nutrition showed high rates of microaspiration in both groups, with no difference in VAP rates.99
Simulated Cough
To overcome the absence of the cough reflex due to the presence of an ETT, an artificial cough maneuver known as rapid flow expulsion is used to clear secretions from the subglottic space: during expiration, the cuff is quickly deflated and a resuscitation bag is squeezed to increase the total gas flow.100 In in vitro experiments, no aspiration was noted, and the maneuver showed good feasibility at the bedside. An automated system based on quick cuff deflations and inflations to simulate cough was recently proposed, but its use in the clinical scenario remains to be evaluated.101
Textiles
A recent crossover double-blind study involving chronic ventilator-dependent subjects showed reduced fever days and antibiotic administration when using textiles impregnated with copper oxide.102 Whether copper textiles can be effective specifically for VAP prevention remains to be shown.
Summary
VAP is a relevant issue in ventilated patients, and its prevention is difficult because of the many factors involved and the lack of a unique definition. Some of the advanced measures proposed to reduce VAP rates are supported by solid evidence, such as the use of subglottic secretion drainage systems and control of ETT cuff pressure. Other measures, such as coated ETTs and probiotic administration, are promising but not recommended because larger studies are still lacking. Other techniques also require further investigation. However, even measures of proven efficacy are still not widely used, probably because mortality is unaffected and a clear cost-benefit advantage is lacking.
Footnotes
- Correspondence: Giacomo Bellani MD PhD, Department of Emergency and Intensive Care, San Gerardo Hospital, University of Milan-Bicocca, Via Pergolesi 33, Monza, Italy 20900. E-mail: giacomo.bellani1{at}unimib.it.
Dr Coppadoro has disclosed a relationship with BIOVO. The other authors have disclosed no conflicts of interest.
- Copyright © 2019 by Daedalus Enterprises
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.
- 24.↵
- 25.↵
- 26.
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.
- 59.
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵









{kind=link}
{kind=link}