

Abstract
Pediatric ARDS continues to be a management challenge in the ICU with prolonged hospitalizations and high mortality. Thromboembolic pulmonary embolism and in situ pulmonary artery thrombosis might represent underappreciated thrombotic processes for a subset of these patients. Although well described in the adult literature, descriptions of pulmonary thromboses with pediatric ARDS are limited to case reports. However, many risk factors for pulmonary thromboses are present in children with ARDS (eg, coagulopathy, endothelial injury, central venous catheters, concomitant inflammatory diseases), suggesting a much higher incidence is plausible. Based on an interpretation of animal, pediatric, and adult data, we propose a diagnostic algorithm to facilitate a timely and accurate diagnosis. Observing an alveolar dead space fraction ≥ 0.25, or either a 50% increase in physiologic dead space/tidal volume or a central venous saturation ≤ 60% over 24 h, triggers the algorithm. Together with targeted heparin treatment and right ventricular afterload reduction, clinical outcomes might improve if this particular patient subgroup can be identified early. While anticoagulation is recommended in adults with confirmed pulmonary embolism and low early mortality risk, data for children are limited.
Introduction
In 1967, Ashbaugh and colleagues first documented ARDS through a case series of 12 adult patients with acute tachypnea, hypoxemia, and loss of pulmonary compliance.1 Although they noted clinical and pathologic similarities to respiratory distress in infants, pediatric-specific definitions of ARDS were only recently proposed.2 Despite this limitation, our understanding of pediatric ARDS has evolved over the past 50 years and has increased our respect for this challenging condition.
Recommendations for lung-protective mechanical ventilation strategies,3 monitoring,4 and non-pulmonary support5 are well established for pediatric ARDS; however, it continues to be associated with high mortality and significant long-term morbidity.6 Given the broad phenotype and heterogeneity of lung disease in pediatric ARDS, other factors should be considered to improve outcomes. Pulmonary thromboses secondary to thromboembolic pulmonary emboli (PE) or in situ pulmonary artery thrombosis are noted pathophysiologic sequelae of ARDS, and they are associated with pulmonary vascular dysfunction7–9 and higher mortality.10 Thromboembolic PE describes classic thromboembolic events from distant non-pulmonary sources, while in situ pulmonary artery thrombosis develops from local pulmonary pathophysiological processes.11 A paucity of literature reports these thrombotic patterns in children.
After reporting the case of an 18-month-old boy with ARDS and pulmonary thromboses,12 we sought to review the literature and propose a diagnostic strategy for recognition and treatment of early thromboses. For clarity, thrombi are defined as intravascular blood clots versus thromboses as the presence or formation of thrombi.
Epidemiology of Pediatric ARDS and Pulmonary Emboli
The determination of epidemiologic data for pediatric ARDS is limited in part by the paucity of large studies, the heterogeneity of definitions in the literature, and its broad etiology and clinical phenotype. Hence, wide ranges in incidence from 2 to 12.8 per 100,000 children are reported for developed countries.13–17 Pediatric ARDS also accounts for 1.4–3.2% of pediatric ICU admissions13–17 and approximately 8% of mechanically ventilated children.16,18 The burden of illness might be higher in developing countries,19 reflecting differences in infectious etiologies, pre-hospital infrastructure, availability of life-sustaining technologies, and baseline health and nutritional status.
PE in children is a rare condition associated with significant morbidity and mortality. North American data from all-comers suggests an annual incidence of 5.7 per 10,000 admissions20 and annual diagnosis rates of 0.9–4.6 per 100,000 children.20,21 However, the diagnosis of thromboembolic PE can be challenging due to subtle and nonspecific clinical presentation as well as a lack of reliable screening protocols and investigations. Accordingly, pediatric autopsy studies suggest a much higher incidence ranging of 0.05–4.2%, with only half of the patients demonstrating clinical signs and symptoms of thromboembolic PE.22,23
The pediatric ARDS patient might be particularly vulnerable to thromboembolic PE. Multiple major risk factors (eg, systemic infection, ICU admission, central venous catheter, mechanical ventilation, prolonged hospitalization, trauma, cardiopulmonary bypass, inflammatory disease, and malignancy)24 are often present during a typical pediatric ICU admission for ARDS. This is supported by postmortem evaluations of adults that indicate thromboemboli in 95% of subjects with ARDS.25 However, such supportive data are not available for pediatric patients.
In Situ Pulmonary Artery Thrombosis
The differentiation between thromboembolic PE and in situ pulmonary artery thrombosis is not clearly elucidated in the pediatric ARDS literature. In adult ARDS, in situ pulmonary artery thrombosis is characterized as micro- and macrothrombi, with balloon-occlusion angiography studies demonstrating arterial filling detects in 42–48% of patients.10,26,27 Postmortem adult studies show even greater involvement, with 86% of patients demonstrating macrothrombi.25
The relationship between in situ pulmonary artery thrombosis and pediatric ARDS emerges from burgeoning pathophysiologic evidence of endothelial damage and dysfunction in lung vasculature, with resultant pulmonary intravascular thrombi. Adult studies suggest that the underlying condition (eg, infection, trauma, malignancy) promotes the pro-inflammatory milieu that results in ARDS, but significant endothelial cell injury occurs concurrently with subendothelial collagen and tissue-factor exposure. Activation of factor VII leading to initial thrombin generation then promotes a more general activation of the coagulation cascade and platelets.28–30 Other potential contributing factors include hypoxic vasoconstriction and extrinsic vascular compression.28–30 Despite more recent advances, pediatric data remain sparse, and the pathophysiologic context of the immature cardio-respiratory, hematologic, and hemostatic systems is largely unknown.
Procoagulant and antifibrinolytic changes are reported in adult patients with ARDS. Bronchoalveolar fluid and plasma samples demonstrate elevated tissue factor, increased factors VII, VIII, and X activity,31,32 elevated plasminogen activator inhibitor-1,33,34 elevated thrombomodulin,33 and decreased protein C.34–35 Furthermore, these changes are associated with increased mortality and morbidity.33–36 Similar associations are confirmed in the pediatric population. Sapru et al37 demonstrated a dose-response relationship between the levels of plasminogen activator inhibitor 1 and mortality as well as ventilator-free days in children with ARDS. Decreased antithrombin III levels are also associated with mortality in pediatric ARDS.38 Biomarkers of endothelial injury such as thrombomodulin,39 von Willebrand factor,40 angiopoietin 2, and soluble receptor for advance glycation end products41 are also associated with increased mortality and decreased ventilator-free days in pediatric ARDS. These biomarkers suggest that coagulopathy and endothelial injury are important pathophysiologic features, and they support a biologic plausibility for in situ pulmonary artery thrombosis in pediatric ARDS. Furthermore, coagulopathy biomarkers and microvascular thromboses are also established in pediatric pneumonia,42 sepsis,43 and multiorgan failure,44 which are conditions that can overlap with an ARDS diagnosis.
Pathophysiologic Consequences of Pulmonary Thromboses
The pathophysiologic consequences of pulmonary thromboses are increased alveolar dead space, a resultant V̇/Q̇ (ventilation/perfusion) mismatch, and increased pulmonary vascular resistance (PVR). However, these changes must be interpreted within the context of expected V̇/Q̇ mismatches from ARDS, which are caused by changes to pulmonary microcirculation, pulmonary vascular dysfunction, and potentially alveolar hyperinflation. Subtleties cannot be appreciated without the routine use of arterial blood gas monitoring and capnography as well as interpretation of newer and more sophisticated mechanical ventilator waveform analysis and dead space quantification.4
Sudden or significant changes to alveolar dead space can represent a sentinel warning sign for large thromboembolic PE. Volumetric capnography can measure acute changes in breath-to-breath alveolar dead space and commonly includes the interpretation of ventilation dead space with tidal volume (VD/VT) and mixed expired air.45,46 However, the literature also reports calculated dead space values (ie, primarily end-tidal alveolar dead space fraction: [PaCO2 − PETCO2]/PaCO2, or AVDSf), making comparisons between studies challenging. With severe PE, VD/VT rapidly increases by nearly 50% in adults47 and ADVSf increases by 100% in porcine models.48 Following pulmonary thromboendarterectomy in intubated adults, VD/VT decreases by nearly 50% the following day.49
Detecting in situ pulmonary artery thrombosis remains problematic because its gradual yet progressive trajectory might correlate temporally with evolving pediatric ARDS. Increased alveolar dead space has been demonstrated in adult50,51 and pediatric52–54 subjects with ARDS. Its association with increased mortality suggests the possibility of underlying pulmonary microvascular alterations.52,54 In adults, treatment with activated protein C decreases dead space, suggesting that the increased dead space might reflect microvascular obstruction.55 An AVDSf ≥ 0.25 at pediatric ARDS onset is associated with a significantly higher mortality rate.54 A high AVSDf that has not improved within 24 h from its baseline measurement is also a poor prognostic indicator.53
Bedside screening for the presence or magnitude of right heart strain secondary to increased PVR is non-specific and non-sensitive. Adult data suggest that a change in mixed venous oxygen saturations (Sv̄O2) following severe PE is the most sensitive predictor of PE compared to all other standard hemodynamic variables (including systolic arterial pressure, cardiac index, pulmonary artery pressure, urine output, and lactate).56 In pediatric patients, central Sv̄O2 are typically obtained instead,57 with thresholds ≥ 70% associated with improved outcomes in conditions with abnormal hemodynamics such as septic shock.58
Proposed Diagnostic Pathway for Pulmonary Thromboses in ARDS
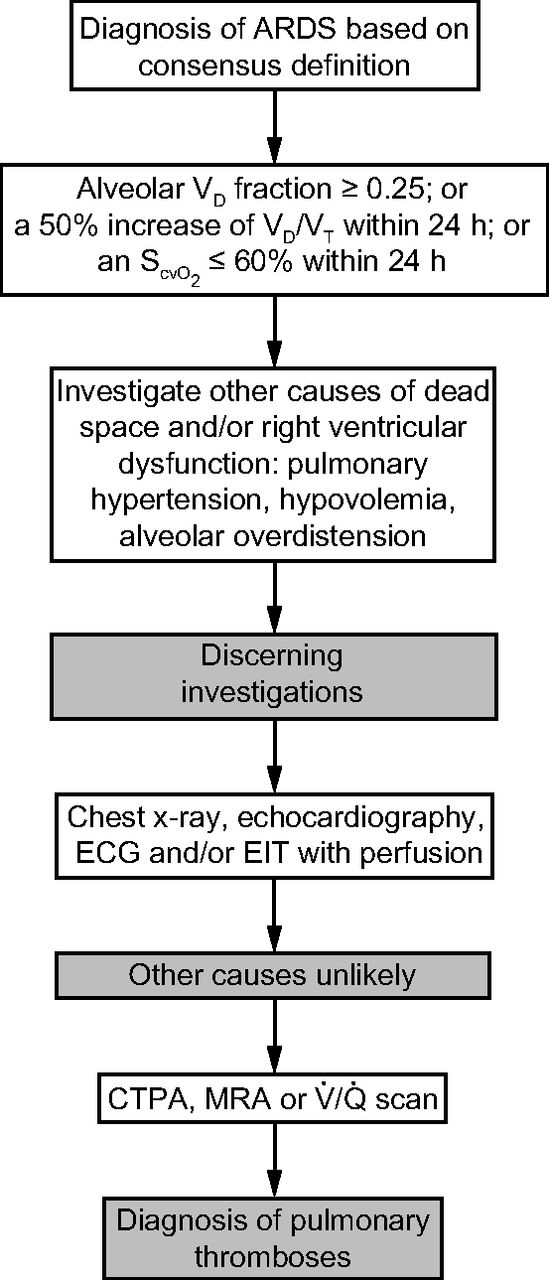
The diagnosis of pediatric ARDS is made by the application of clinical criteria utilizing consensus definitions. Earlier observations by Ashbaugh et al1 gradually led to the Berlin definition for ARDS in 2012,59 which has since been validated in both adults and children. More recently, the Pediatric Acute Lung Injury Consensus Conference also developed pediatric specific definitions.2 With no recommendations regarding the diagnosis of pulmonary thromboses and pediatric ARDS,60 we propose an algorithm based on the best available evidence (Fig. 1).

Proposed diagnostic pathway for pulmonary thromboses with pediatric ARDS. VD/VT = dead space/tidal volume; ECG = electrocardiogram; EIT = electrical impedance tomography; CTPA = CT pulmonary angiogram; MRA = magnetic resonance angiography.
While clinically important pulmonary thromboses are thought to be rare in pediatric ARDS, the evidence suggests that the concomitant lung disease either conceals or results in this under-diagnosis. Unfortunately, clinical signs and symptoms of pulmonary thromboses, as well as the utilization of d-dimer or probability scoring systems, are low-yield when investigating such diagnoses in children.61 In the event that a pulmonary thromboses diagnosis is made, a significant lag (1–7 d) from symptom onset often exists.62 Hence, actual incidence cannot be appreciated unless the clinician begins with a high index of suspicion for all pediatric ARDS patients.
Diagnostic variables for alveolar dead space and elevated PVR have not been validated in pediatric patients with ARDS and pulmonary thromboses. Nevertheless, we propose the following three thresholds to initiate our diagnostic algorithm based on the summative data presented earlier: (i) an AVDSf ≥ 0.25; (ii) a 50% increase of VD/VT within 24 h; or (iii) a central Sv̄O2 ≤ 60% within 24 h.
The proposed changes to dead space and central Sv̄O2 should prompt subsequent investigations to rule out causes other than pulmonary thromboses. Although chest radiography has a low sensitivity and specificity for pulmonary thromboses, it might be helpful to exclude clinical mimickers. Electrocardiograms should be obtained; however, evidence of the classic S1Q3T3 finding is only reported in 12% of acute thromboembolic PE in children, and other abnormalities such as right axis deviation and right bundle branch block are not very reliable.63,64 Bedside Doppler echocardiography is not systematically used in pediatric ARDS, but it might be useful in evaluating ARDS severity with the suspected continuum of alterations in pulmonary circulation and right ventricular function.65 In adults, a recent meta-analysis suggests that transthoracic echocardiography consistently demonstrates a high specificity and low sensitivity in the diagnosis of PE,66 but its generalizability to children is uncertain.63,67 Finally, improvements in electrical impedance tomography might be the future for evaluating bedside pulmonary perfusion for critically ill patients.68 Its advantages include safety, portability, real-time assessment without radiation, and burgeoning research detecting small changes in ventilation and perfusion impedance induced by large thromboembolic PE.69–72 However, clinical validation is lacking, and further effort is required to improve the detection of small perfusion-impedance signal changes.68 Once optimized, electrical impedance tomography has the potential to detect smaller pulmonary artery filling defects that could be secondary to smaller pulmonary thrombi.
Diagnostic imaging for thromboembolic PE has predominantly included computed tomography with pulmonary angiography and V̇/Q̇ scans. Concordance studies between these modalities have not been conducted in children, and their respective sensitivity and specificity are difficult to determine because many thromboembolic PE are diagnosed postmortem.11 V̇/Q̇ scanning presents major logistical challenges to the ventilated child with the requirement of aerosol inhalation, often limiting the investigation to perfusion studies only. Pulmonary angiography is another alternative, but it is invasive, is time-consuming, introduces potential complications, and is not always available.73 For in situ pulmonary artery thrombosis, optimal imaging modalities are difficult to discern because a strict differentiation from thromboembolic PE has not been made consistently.11 Newer modalities such as pulmonary magnetic resonance angiography are promising, but they might present several practical challenges in critically ill children due to long examination times and difficulties with patient monitoring.
Pulmonary Thromboses Treatment
Despite the identified pathophysiologic risk of thromboses with pediatric ARDS, the current treatment strategies with these patients target ventilator adjustments with disease evolution.3 It is unclear how often respiratory deteriorations are secondary to pulmonary thromboses, as is whether treatment with anticoagulation should be initiated with only a high index of clinical suspicion. A recent meta-analysis of randomized, controlled trials in adults suggests adjuvant treatment with low-molecular-weight heparin was associated with reducing 7-d and 28-d mortality and improved oxygenation among subjects with acute lung injury/ARDS.74 Promising new anticoagulation therapies in adults have not been successful in large ARDS clinical trials, but smaller and selective patient subgroups who might have benefitted were never delineated a priori.75
Initial anticoagulation with unfractionated heparin or low-molecular-weight heparin should be considered in pediatric pulmonary thromboses.11,76 Unfractionated heparin offers the advantage of rapid reversibility by discontinuing the infusion or by administering protamine in the situation of significant bleeding. Disadvantages include the need for a dedicated line for infusion and the requirement for frequent monitoring, ideally with both an activated partial thromboplastin time and anti-Xa level for correlation. Unfractionated heparin also strongly binds plasma proteins, including inflammatory cytokines (invariably present in pediatric ARDS), which can result in potential undershooting of the activated partial thromboplastin time range despite apparently normal starting doses. Finally, unfractionated heparin (relative to low-molecular-weight heparin) places the patient at higher risk for heparin-induced thrombocytopenia, a condition that can paradoxically worsen the thrombotic event.
By comparison, low-molecular-weight heparin offers the advantage of a subcutaneous injection 1–2 times per day with generally less frequent required monitoring of anti-Xa levels.77 Furthermore, low-molecular-weight heparin does not affect the activated partial thromboplastin time, so monitoring of thromboplastin times is not required. A major disadvantage to low-molecular-weight heparin is the suboptimal reversibility relative to unfractionated heparin in case of bleeding. Systemic thrombolytic therapy is reserved for thrombi that create life-threatening hemodynamic instability. Local installation of thrombolytic therapy through the pulmonary artery via catheterization is another potential alternative, although its efficacy in children is unknown.
The risk of major hemorrhage with anticoagulation and thrombolysis is reported in 21.8% and up to 40% of children, respectively;78 therefore, initiation of empiric anticoagulation in suspected but not proven pulmonary thrombosis is debatable. Furthermore, monitoring frequency and target ranges for anticoagulation therapy have not been evaluated in large prospective trials. However, if anticoagulation is initiated, the current recommendations are to target anti-Xa levels of 0.35–0.7 units/mL and 0.5–1.0 units/mL for unfractionated heparin and low-molecular-weight heparin, respectively.77 Significant variation in duration of anticoagulation therapy is noted11 and should be directed by thrombosis consultants.
Mechanical Ventilation Considerations With Pulmonary Thromboses
Optimal ventilatory support for children with pulmonary thromboses has not been clearly described. Although noninvasive positive-pressure ventilation might be considered with milder pediatric ARDS,79 pulmonary thromboses usually heralds worsening gas exchange and will typically require intubation. For these patients, ARDS guidelines suggest open lung strategies with moderately elevated PEEP values and small VT for conventional ventilation modes.3 Recommended alternatives for poor pulmonary compliance and hypoxemic respiratory failure are prone ventilation and high-frequency oscillation ventilation.3 Specific caveats for pulmonary thromboses within the guidelines have not been made.
Additional principles to address for optimizing gas exchange impeded by thromboses are reducing right ventricular afterload and promoting pulmonary circulation. Echocardiographic data from < 72 h after acute PE demonstrate right ventricular dysfunction in 25% of pediatric cases.63 Therefore, PVR can be mitigated by avoiding atelectatic and over-distended alveoli, but finding the appropriate balance can be challenging. Both inhaled nitric oxide80 and milrinone81 are reported for management of acute pulmonary thromboses in adults, and these could be considered for children. In addition to pulmonary vasodilation, milrinone exerts both positive inotropic and lusitropic effects to support the right ventricle.
Outcomes
The paucity of outcome data on pediatric pulmonary thromboses and ARDS is likely related to present limitations related to quantifying thromboses and differentiating procoagulant processes with nonthrombotic vascular dysfunction. If pulmonary thromboses are associated with raised PVR, poorer outcomes could be related to either right ventricular failure or exacerbation of lung injury.7 Although right ventricular dysfunction has been independently associated with increased morbidity and mortality in adults with pulmonary vascular dysfunction and ARDS,8,9 and elevated PVR might indicate disease severity and progression,7 causal conclusions concerning thrombotic outcomes cannot be made.
As a surrogate, separate pediatric outcome data from ARDS and thromboembolic PE could be considered. Mortality from pediatric ARDS ranges from 15% to 50%, reflecting differing etiologies, patient comorbidities, ventilatory strategies, pediatric ICU care, and time of study.6 Some mortality risk factors might exacerbate the procoagulant, antifibrinolytic phenotype of pediatric ARDS (eg, disseminated intravascular coagulation,82 non-pulmonary sepsis,13 multiorgan failure83) and pulmonary vascular dysfunction (eg, immunosuppression,13,84 high VT85), or they may encourage thromboembolic events (eg, hematologic malignancies85,86). Children who survive pediatric ARDS require hospital admissions for > 20 d15 and can develop chronic obstructive and restrictive pulmonary disease.6 A recent pediatric review estimated mortality at 26% (n = 15 studies) and < 20% (n = 9 case series) from thromboembolic PE and in situ pulmonary artery thrombosis, respectively.11 While pediatric ARDS might not have evolved in many of these cases (ie, thrombi secondary to congenital heart disease, pulmonary artery anomalies), the coupling of thromboses with pediatric ARDS likely represents a more severe presentation with poorer outcomes.
In our case report,12 inhaled nitric oxide did not improve oxygenation, but a milrinone infusion did. The patient was treated with a heparin infusion, and within 72 h a significant improvement in his dead space ventilation was noted. His ventilator support was gradually weaned, and he was successfully extubated on day 18 of his pediatric ICU admission. He continues to be followed by both respirology and cardiology specialists, and long-term sequelae have yet to be documented.
Summary
The most recent major recommendation by the Subcommittee on Pediatric and Neonatal Thrombosis and Hemostasis outlines the need to improve awareness and education for the prompt investigation and diagnosis of pulmonary thromboses in children.87 Thromboembolic PE and in situ pulmonary artery thromboses are likely under-recognized in pediatric ARDS cases, and their current role in patient outcomes is unknown. Awareness of patients at risk for pulmonary thrombosis within the heterogeneous context of pediatric ARDS should be coupled with diagnostic pathways that might include changes in the ventilatory dead space fraction and emerging bedside technologies. Together, earlier diagnosis with timely and targeted treatment might attenuate right heart strain and pulmonary artery dysfunction, and it may improve patient morbidity and mortality. Whether our proposed diagnostic pathway will increase thrombi detection is unknown, and we will evaluate its efficacy by incorporating electrical impedance tomography once perfusion software is available.
Footnotes
- Correspondence: Gregory Hansen, Pediatric Intensive Care Unit, 103 Hospital Drive, Saskatoon, SK, Canada S7N 0W8. E-mail: gregory.hansen{at}usask.ca.
The authors have disclosed no conflicts of interest.
- Copyright © 2019 by Daedalus Enterprises
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.
- 71.
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵









{kind=link}
Jump to section
- Article
- Abstract
- Introduction
- Epidemiology of Pediatric ARDS and Pulmonary Emboli
- In Situ Pulmonary Artery Thrombosis
- Pathophysiologic Consequences of Pulmonary Thromboses
- Proposed Diagnostic Pathway for Pulmonary Thromboses in ARDS
- Pulmonary Thromboses Treatment
- Mechanical Ventilation Considerations With Pulmonary Thromboses
- Outcomes
- Summary
- Footnotes
- References
- Figures & Data
- Info & Metrics
- References