

Abstract
BACKGROUND: The Berlin definition of ARDS does not account for nonpulmonary organ failure, which is a major determinant of outcome. We examined whether an increasing severity of hypoxemia across the Berlin definition classifications also corresponded with evidence of multiple organ dysfunction on the day of ARDS onset. We also examined the representation of major etiologies for ARDS across the Berlin definition classifications.
METHODS: This single-center, retrospective study examined 15 years of data from a quality assurance program that monitored the use of lung-protective ventilation in ARDS. We analyzed 1,747 subjects without chronic kidney disease or severe chronic liver disease at ARDS onset. The most abnormal laboratory values at ARDS onset were analyzed as cutoff values to assess organ dysfunction. Data were analyzed by using non-parametric analysis of variance (Kruskall-Wallis test) and the Dunn post test. Categorical variables were compared by using the Fisher exact test. Alpha was set at 0.05. Factors independently associated with mortality were assessed by multivariate logistic regression modeling.
RESULTS: Nonpulmonary organ dysfunction was present in at least 1 system at ARDS onset that increased with severity: 80% (mild), 83% (moderate), and 90% (severe). ARDS etiologies varied as severity increased: trauma-associated lung injury steadily decreased, whereas lung injury associated with aspiration and pneumonia steadily increased. Hospital mortality also increased significantly with the Berlin definition classifications: mild (22%), moderate (30%), and severe (47%). Multivariate logistic regression modeling revealed that the Berlin definition of severe ARDS was independently associated with mortality, as were cutoff values for renal and hepatic function as well as acidemia. Normal hematologic function and the absence of standard exclusion criteria used for therapeutic clinical trials in ARDS were protective.
CONCLUSIONS: Nonpulmonary organ dysfunction was present at ARDS onset in most subjects and was more pronounced as ARDS severity increased. The Berlin definition classification of ARDS provided an elegant scheme for studying the syndrome because it coincided with increasing multiple organ dysfunction.
Introduction
The 2012 Berlin definition of ARDS1 was developed to update and address limitations associated with the landmark 1994 American-European Consensus Conference definition of acute lung injury.2 The Berlin definition Task Force's focus was to determine thresholds of pulmonary-specific variables that could be used to distinguish syndrome severity as well as possessing both face and predictive validity, thus, a pragmatic tool by which past and future ARDS therapies could be evaluated.1 As such, the task force intentionally did not consider other variables that would likely improve the predictive validity (such as age and severity of nonpulmonary organ failure) because these were not specific to the definition of ARDS.1 Because feasibility and consistency with the previous American-European Consensus Conference definition2 were essential features that drove the Berlin definition, the results of statistical modeling behooved the conference to use cutoffs in the ratio of PaO2/FIO2 to demarcate ARDS as being mild, moderate, or severe.1 From a broader, scientific perspective, having a practical tool such as the Berlin definition is essential for advancing epidemiologic and therapeutic research into ARDS, yet, it opens areas of interest that, to our knowledge, have not been well explored.
Because mortality from ARDS is disproportionately due to multi-organ dysfunction syndrome rather than hypoxemia,3,4 our interest was examining the relationships between nonpulmonary organ dysfunction at ARDS onset across Berlin definition classifications.1 We were motivated by curiosity over our previous multivariate logistic modeling of ARDS,5 wherein the Berlin definition and PaO2/FIO2 were excluded from the final model because Simplified Acute Physiology Score (SAPS II),6 total bilirubin, physiologic dead-space fraction, and oxygenation index were more powerful in assessing mortality risk.
These results were similar to our previous findings during traditional tidal volume ventilation in ARDS.7 This also raised the question of whether increasing mortality with increasing ARDS severity by the Berlin definition might also have been influenced by variations in the distribution of etiologies. The present study, therefore, examined the relationship between the Berlin definition of ARDS1 severity and (1) the presence of organ dysfunction and/or illness severity at ARDS onset, (2) the distribution of etiologies commonly measured in ARDS, and (3) hospital mortality across both Berlin definition classifications and primary ARDS etiologies. Our intention was to provide a more detailed description of nonpulmonary organ dysfunction at ARDS onset based on the Berlin definition1 and whether any differences might provide more insight into the higher mortality that coincides with decreasing oxygenation.
QUICK LOOK
Current knowledge
Mortality in ARDS primarily results from progressive multiple organ failure rather than refractory hypoxemia. As such, ARDS is perceived as signifying the pulmonary manifestation of multiple organ dysfunction. The newest iteration for classifying ARDS (the Berlin definition) is based solely on cutoff values in PaO2/FIO2, which showed significantly increased mortality with increasing severity in oxygenation dysfunction, irrespective of concurrent derangements in other organ systems.
What this paper contributes to our knowledge
Nonpulmonary organ dysfunction was pervasive at ARDS onset, the prevalence and severity of which increased with increasing severity of hypoxemia. This phenomenon largely preceded substantial exposure to lung-protective ventilation. In addition, primary ARDS etiologies differed across severity classifications. Trauma-associated ARDS, with the lowest mortality rate, decreased in prevalence with increasing syndrome severity; whereas aspiration-associated ARDS, with the second highest mortality rate, increased in prevalence with increasing severity. This study also confirmed previous findings that a blood urea nitrogen to creatinine ratio >20 (a signifier for catabolism in critical illness) was independently associated with mortality.
Methods
This study analyzed data from 1,962 subjects who were mechanically ventilated between June 2002 and June 2017, and who met the American-European Consensus Conference criteria for acute lung injury and ARDS2; these subjects were subsequently reclassified according to the Berlin definition.1 Data about these subjects were entered into a quality assurance database at San Francisco General Hospital and Trauma Center used to monitor the adoption of the National Heart, Lung and Blood Institute's ARDSnet ARMA8 ventilator protocol and later incorporated aspects of the ARDSnet ALVEOLI trial protocol.9 However, it also included all the subjects with ARDS, regardless of strict adherence to those protocols. This database consists primarily of information gathered from the day of ARDS onset, including mechanical ventilation and gas exchange data, initial illness severity scores, and other demographic data and hospital mortality. One investigator (RHK) screened the subjects according to the primary source of lung injury as well as sepsis as a co-diagnosis. Acute Physiology and Chronic Health Evaluation (APACHE II),10 and SAPS II6 scores were calculated on the day of ARDS onset. Basic demographic and outcome information was also collected. Approval to use our quality assurance data was granted by the University of California, San Francisco Institutional Review Board.
Of the 1,962 patients we excluded 215: 59 due to incomplete data, 59 for chronic renal disease, and 97 for severe chronic liver disease defined as Child C (Fig. 1). Our database did not capture less-severe liver disease (ie, Child A and B). The assessment of nonpulmonary organ dysfunction on the day of ARDS onset used the most abnormal values gathered for calculating the APACHE II score and SAPS II as well as the lowest platelet count and highest base deficit. We then used pre hoc cutoff values for mean arterial pressure of <65 mm Hg,11 and pronounced acidosis, which we defined as either a pH < 7.20 or a base deficit of >10 mEq/dL.12 For renal dysfunction, we used a creatinine (Cr) level of > 1.9,13 urine output of <0.5 mL/kg/h),14 blood urea nitrogen of > 46 mg/dL (twice the upper normal limit), and a blood urea nitrogen to Cr ratio (BCR) of >2015 as signifiers of acute kidney injury. For coagulation disorder, we used platelet count thresholds for both thrombocytopenia and severe thrombocytopenia (<150,000 and < 50,000/mm3, respectively),16 whereas, for hepatic injury, we used a total bilirubin of >2.17 However, the tallying of organ system dysfunction was based only on cutoff values for mean arterial pressure, Cr, platelet count (<150 × 103/mm3), and total bilirubin mg/dL.

Flow chart.
Statistical Analysis
Statistical analysis was done by using either Stata 9.0 (Stata, College Station, Texas) or Instat 3 (GraphPad Software, La Jolla, California). Continuous variables were expressed as median (interquartile range) and were compared by using the Mann-Whitney test. Comparisons of continuous variables between the Berlin definition classifications and ARDS etiologies were done by using non-parametric analysis of variance (Kruskall-Wallis test) and the Dunn post test. Categorical variables were compared by using the Fisher exact test. Alpha was set at 0.05.
Stepwise backward logistic regression modeling primarily was used to assess the influence of nonpulmonary factors on hospital mortality. The only pulmonary-related variables used in the model were the Berlin definition categories.1 Other variables included pre hoc cutoff values (described above), which signify aspects of cardiovascular, renal, hepatic, and hematologic dysfunction as well as APACHE II, SAPS II, age, primary ARDS etiology, sepsis as a co-diagnosis, and formal use of the ARDSnet ventilator protocol, and whether subjects met ARDSnet comorbidity exclusion criteria.8 Variables with P < .20 remained in the final model.
Results
Hypotension, renal impairment, acidosis, and higher APACHE II and SAPS II scores were significantly associated with ARDS severity at syndrome onset and coincided with increased hospital mortality (Table 1). Differences in nonpulmonary organ dysfunction between Berlin definition classifications became more apparent when assessed by using pre hoc cutoffs (Table 2). At syndrome onset, between 80 and 90% of the subjects had at least one dysfunctional nonpulmonary organ system, the most prevalent being cardiovascular (73%), followed by hematologic (46%), renal (20%), and hepatic (19%) (Fig. 2). The presence of nonpulmonary organ dysfunction was significantly greater in severe ARDS (90%) versus both mild (80%) and moderate ARDS (83%) (P < .001) Moreover, the number of dysfunctional organ systems involved also increased with ARDS severity (see http://www.rcjournal.com).
Distribution of Illness Severity and Organ-System Dysfunction on the Day of ARDS Onset by Berlin Definition Categories1
Odds Ratio (95% CI) for Nonpulmonary Organ Dysfunction on the Day of ARDS Onset According to the Berlin Definition

Prevalence and number of nonpulmonary organs with signs of dysfunction at ARDS onset according to Berlin definition classifications.
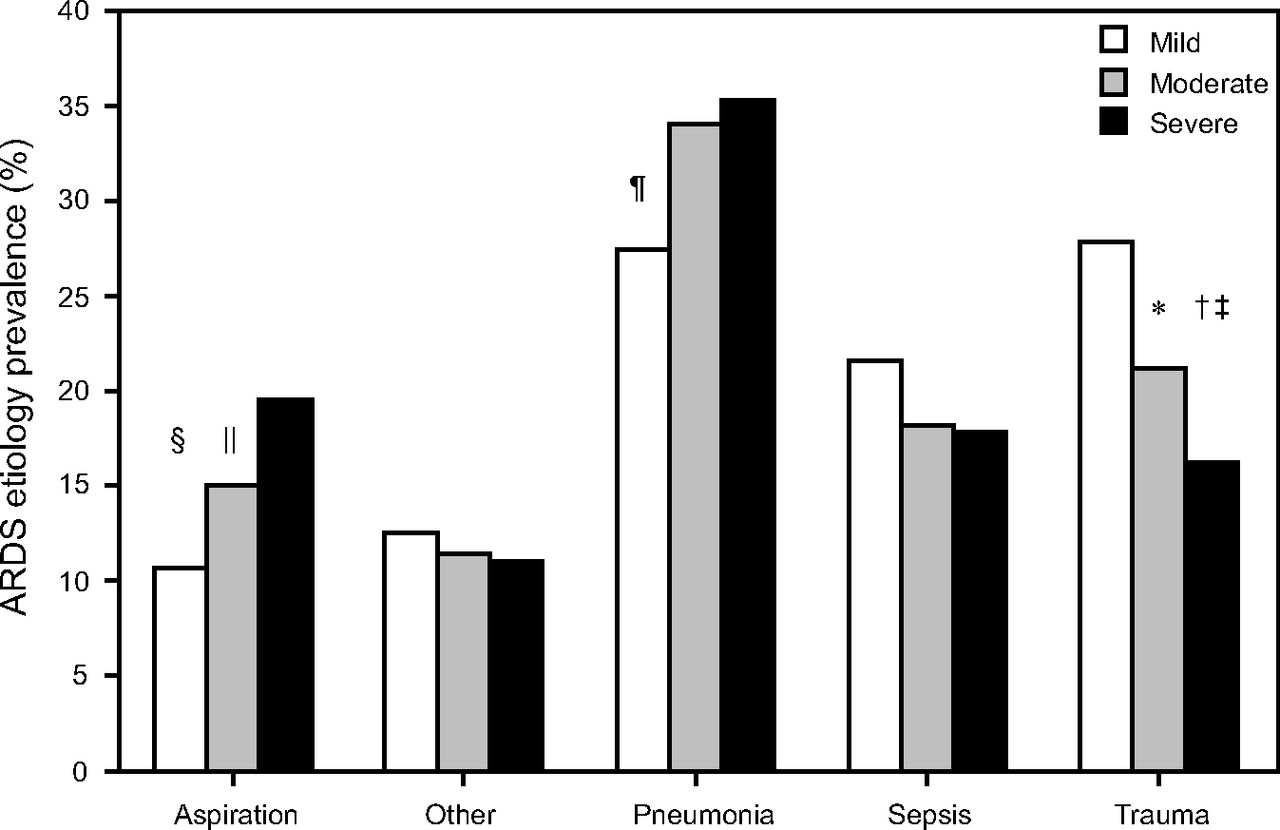
Primary ARDS etiologies differed across severity classifications. The percentage of subjects with trauma-associated ARDS decreased significantly as severity increased (Fig. 3). When organ dysfunction was assessed by primary ARDS etiology, the most consistent findings were the significantly higher degree of organ dysfunction in non-pulmonary sepsis and least impairment with trauma-associated ARDS (Table 3). A similar pattern was found when comparing APACHE II and SAPS II scores between etiologies, the only salient difference was that scores for aspiration-associated ARDS were not different than that found in non-pulmonary sepsis. In contrast, the prevalence of aspiration increased significantly with increasing ARDS severity, whereas pneumonia was more prevalent in moderate and severe ARDS compared with mild ARDS. Although nonpulmonary sepsis was not different across Berlin definition classifications, when sepsis was analyzed as a co-diagnosis, there was a significantly higher incidence in those subjects with severe ARDS (42%) compared with either mild (33%) (P = .01) or moderate forms (34%) (P = .003).

Distribution of ARDS etiology across Berlin definition classifications (* P = .016 versus mild, † P = .002 versus mild, ‡ P = .03 versus moderate, § P < .001 versus severe, II P = .03 versus severe, ¶ P = .03 versus moderate and severe).
Differences in Nonpulmonary Organ Dysfunction on the Day of ARDS Onset by Primary Etiology of Lung Injury
The subjects with severe ARDS succumbed more rapidly, with a 16% mortality rate that occurred within 2 d of syndrome onset versus those with either mild (2%) or moderate (6%) forms at the same time point (Fig. 4). This trend persisted throughout the first 28 d of ARDS. Between days 28 and 60, there was only a modest, 2–3%, increase in mortality among those with severe and moderate ARDS versus 1% among those initially categorized as having mild ARDS. Overall mortality was highest with nonpulmonary sepsis (44%) and lowest with trauma (22%) (see the supplementary materials at http://www.rcjournal.com). Within these 2 groups, mortality increased steadily from mild to severe ARDS from 35–56% (for sepsis) and 14–32% (for trauma).

Survival during the first 28 days of ARDS onset and at Day 60 by Berlin definition classifications.1
Although we excluded those with preexisting kidney and severe liver disease from our primary analysis, we also considered whether these patients might have populated more-severe forms of ARDS at syndrome onset. The percentage of those excluded due to chronic kidney disease was 3.7% (mild), 3.3% (moderate), and 2.5% (severe); none of the differences were significant (P values ranged from .58 to .82). Likewise, those with Child C liver dysfunction were 3.4% (mild), 5.3% (moderate), and 5.4% (severe); none of the differences were significant (P values ranged from .17 to .74). Despite the lack of distribution bias across Berlin definition classifications, these cohorts had substantially higher hospital mortality rates (52% for chronic renal disease and 78% for Child C liver disease).
The final multivariate logistic regression model revealed 11 factors independently associated with mortality. Among the three Berlin Definition categories, only severe ARDS was independently associated with hospital mortality (Table 4). In terms of organ systems, acute renal dysfunction (signified by a urine output of <0.5 mL/kg/h, BCR > 20) were associated with an increased mortality risk, as was hepatic dysfunction and pH < 7.20. In contrast, normal platelet function (ie, > 150 × 103/mm3) and having no exclusion factors for enrollment into a randomized controlled trial were protective. In terms of demographics, there was no difference across ARDS classifications in either the distribution of sex (females constituted 27 to 30% of each group) or in ethnicity: classified as Asian descent (17%), African descent (20%), Hispanic descent (22%), European descent (40%), and other groups (2%) who were either Native American or Middle-Eastern descent.
Adjusted Analysis of Organ Dysfunction and Mortality at Onset of ARDS
Discussion
The prominent findings of our study were as follows. First, nonpulmonary organ dysfunction was present at ARDS onset. As ARDS severity increased, so too did the degree of organ dysfunction as well as the number of involved systems. Second, impaired renal perfusion, hepatic dysfunction, marked acidosis, and severe ARDS (ie, PaO2/FIO2 ≤ 100 mm Hg) were independently associated with mortality risk. In contrast, normal hematologic function and the absence of standard exclusion criteria for enrollment into a therapeutic randomized controlled trial for ARDS were protective. Third, the mortality rates that we observed across ARDS categories were consistent with those reported by the Berlin definition Task Force.1 Moreover, the relative rapidity by which those with severe ARDS succumbed was particularly noteworthy. Fourth, the distribution of ARDS etiologies differed as severity increased with increasing prevalence of aspiration and pneumonia and with decreasing prevalence in trauma-associated acute lung injury.
A secondary finding was that an elevated BCR > 20, was independently associated with mortality and outperformed cutoffs for Cr and blood urea nitrogen. Rachoin et al15 also reported an association between BCR > 20 and mortality in the subjects who were critically ill. Together these findings contradicted a previous impression that elevated BCR represents pre-renal azotemia rather than kidney injury, thus, carrying a lower mortality risk.18 Rachoin et al15 reasoned that catabolism associated with critical illness (signified by elevated urea production) often coincides with reduced muscle mass, and causes lower Cr generation. Lower muscle mass related to advanced age, poor nutritional status, and female sex are associated with increased mortality risk during critical illness.18–20 Consistent with the findings of Rachoin et al,15 we found that BCR > 20 was significantly higher among whites (odds ratio [OR] 1.65 [95% CI 1.18–2.29], P = .004), females (OR 1.59 [95% CI 1.05–2.11], P = .026), and those age ≥65 y (OR 2.64 [95% CI 1.77–3.94], P < .001).
Mortality in patients who are critically ill results from the interactions among multiple failing organs, such that ARDS reflects the pulmonary manifestation of multiple organ failure.21 Multiple organ failure involves the phenomenon of “organ cross-talk” among systems, primarily through endothelial damage; the most commonly involved systems are pulmonary, cardiovascular, hematologic, renal, hepatic, gastrointestinal, and neurologic.21 Although the focus has been on the contribution of ventilator-induced lung injury, it is apparent that acute lung injury precedes invasive mechanical ventilation by hours and sometimes days. Thus, our interest was in investigating the presence of multiple organ failure signifiers at ARDS onset and before prolonged exposure to mechanical ventilation. In multiple organ failure reciprocal interactions between the lungs and kidneys have received the most attention.22 Because both function as “exchange organs,” which possess vast capillary networks, the endothelium of each is exposed to circulating inflammatory mediators, neutrophils, and monocytes, which renders each organ vulnerable to secondary injury from the other (as well as from other injured organs).
ARDS is independently associated with acute kidney injury, and patients with ARDS have a higher incidence of acute kidney injury compared with those without acute lung injury (44 vs 27%, respectively).23 Darmon et al23 reported acute kidney injury in ∼20% of subjects within 2 d of ARDS, which reached 44% by day 30. Of interest is that 52% of their subjects were classified as having mild ARDS. Moreover, acute kidney injury was independently associated with mechanical ventilation in those without ARDS. In contrast, at ARDS onset, 11% of our subjects already met acute kidney injury criteria. Only 15% had mild ARDS compared with 35% with severe ARDS. Moreover, in 62% of our subjects, mechanical ventilation was initiated on the day of ARDS onset compared with 17% initiation within 24 h, and 7% within 48 h before ARDS onset. These subjects were managed with the ARDSnet ventilator protocols.8,9 In the absence of ARDS, our practice is to ventilate all patients at a tidal volume of ≤8 mL/kg predicted body weight.
Nonetheless, it is not possible to ascertain the degree to which nonpulmonary organ dysfunction was attributable to ARDS versus mechanical ventilation. At ARDS onset, the subjects with mild, moderate, and severe ARDS were initially ventilated at mean tidal volumes of 7.3–7.4 mL/kg predicted body weight, with corresponding mean plateau pressures of 23, 24, and 27 cm H2O, respectively, and with mean driving pressures of 15, 16, and 17 cm H2O, respectively. The subjects with mild, moderate, and severe ARDS who survived until the next day had achieved mean tidal volumes of 6.2–6.3 mL/kg predicted body weight, mean plateau pressures of 23, 24, and 26 cm H2O, respectively, and mean driving pressures of 15, 14, and 14 cm H2O, respectively. Thus, it could be argued that ventilator-induced lung injury to distal organ dysfunction was likely a lesser factor than that initiated by the lung injury itself. However, studies by Terragni et al24 and Amato et al25 also indicate that exposure to plateau pressures of >26 cm H2O and driving pressures of >15 cm H2O (as occurred in our subjects with severe ARDS) may have contributed to nonpulmonary organ dysfunction. It is important to note that, in our study, nadir values in nonpulmonary organs on the day of ARDS onset could have occurred hours before or after the initiation of mechanical ventilation.
We also found that the absence of exclusion criteria used in the original ARDSnet trial had a protective effect.8 Because we already had excluded patients with Child C liver failure, this finding primarily reflected subjects in whom ARDS was complicated by acute brain injury. In addition, our finding that those whom we excluded because of severe chronic renal and hepatic disease had a higher mortality was in keeping with a previous study that demonstrated that ARDS mortality in the general population was consistently higher than that reported in randomized controlled trials in which subjects with substantial comorbidities were excluded.26
Also, in our previous studies PaO2/FIO2 and Berlin definition classifications1 were not robust predictors of hospital mortality compared with age, comorbidities, APACHE II and SAPS II scores, physiologic dead-space fraction, and oxygenation index.5,7,27 Although this seemed contradictory, categorizing ARDS according to the Berlin definition demarcates salient differences in oxygenation, reflective of pulmonary dysfunction that coincides with an increasing incidence of multiple organ failure. Thus, the elegance of the Berlin definition serves well the pragmatic needs of investigators who seek to advance our understanding into the epidemiology of ARDS as well as in evaluating new therapies.
The limitation of our study was its retrospective nature from a single center, by using quality assurance data with restricted granularity, so that the generalizability of our results was constrained. Despite these limitations, the data were derived from a large sample population characterized by well-represented etiologies of ARDS as well as diverse racial and ethnic backgrounds. It, therefore, provided a provisional glimpse into the nature and degree of nonpulmonary organ dysfunction and its distribution across Berlin definition classifications at ARDS onset and, for the majority of our subjects, before prolonged exposure to mechanical ventilation by using a lung-protective strategy.
Conclusions
Substantial nonpulmonary organ dysfunction was present on the day of ARDS onset that increased with increasing ARDS severity. Primary ARDS etiologies varied across classifications as severity increased with trauma decreasing and with aspiration and pneumonia increasing. BCR > 20 was associated with increased mortality risk and may signify the presence of a catabolic state.15 Mortality increased with ARDS severity; the rapidity with which subjects succumbed within the first few days was substantially higher in severe ARDS, a finding consistent with our observation that statistically significant differences in nonpulmonary organ dysfunction generally were not found between mild and moderate ARDS. The Berlin definition classification of ARDS severity1 is an elegant and useful scheme for studying the syndrome because it coincidentally captures increasing incidence of multiple organ failure.
Footnotes
- Correspondence: Richard H Kallet MSc RRT FAARC. E-mail: richkallet{at}gmail.com.
Mr Kallet presented a version of this paper as an Editors' Choice abstract at the Open Forum of the AARC Congress, held October 4-7, 2017, in Indianapolis, Indiana.
Mr Kallet discloses relationships with Nihon Kohden, Philips Respironics, and Getinge Group. The remaining authors have disclosed no conflicts of interest.
Supplementary material related to this paper is available at http://www.rcjournal.com.
See the Related Editorial on Page 610
- Copyright © 2019 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}
{kind=link}