

Abstract
BACKGROUND: High-flow nasal cannula (HFNC) is a key component of oxygen therapy and has largely been used in patients with acute respiratory failure. We conducted a matched controlled study with the aim to compare the preventive use of oxygen therapy delivered by HFNC versus via air-entrainment mask (standard O2) after extubation in adult subjects with liver transplantation for reducing postextubation hypoxemia.
METHODS: Twenty-nine subjects with liver transplantation who received HFNC after extubation (HFNC group) were matched 1:1 with 29 controls (standard O2 group) chosen from an historical group of 90 subjects admitted to the ICU during the previous 36 months. The primary outcome of the study was the incidence of hypoxemia at 1 h and 24 h after extubation. Secondary outcomes were the rate of weaning failure, ICU length of stay, and 28-d mortality.
RESULTS: The incidence of hypoxemia was not significantly different between the HFNC and standard O2 groups at 1 h and 24 h after extubation. In the HFNC group, there was a trend toward a lower rate of weaning failure compared with the standard O2 group. ICU length of stay and 28-d mortality were similar in both groups.
CONCLUSIONS: Early application of HFNC in the subjects with liver transplantation did not reduce the incidence of hypoxemia after extubation compared with standard O2 and did not modify the incidence of weaning failure, ICU length of stay, and 28-d mortality in this high-risk population of subjects. (ClinicalTrials.gov registration NCT03441854.)
- high-flow nasal cannula
- standard oxygen therapy
- postoperative pulmonary complications
- liver transplantation
- noninvasive ventilation
- postoperative hypoxemia
Introduction
Postoperative pulmonary complications are frequently observed after major abdominal surgery and increase morbidity, mortality, and length of ICU and hospital stay. Anesthesia, postoperative pain, and surgical procedure, especially liver transplantation, result in a low end-expiratory lung volume and altered physiology (vital capacity, functional residual capacity, tidal volume), atelectasis, restrictive syndrome, and diaphragmatic dysfunction. Derangements of respiratory function are observed in up to 90% of patients undergoing major surgery, may last up to 7 d (eg, diaphragmatic dysfunction), and frequently result in significant and prolonged reduction of arterial oxygenation.1–6 Furthermore, patients who undergo liver transplantation are commonly affected by several comorbidities and have to cope with stressful surgery due to its duration and risk of bleeding; moreover the latter is associated with massive transfusion and consequent respiratory failure.7 In this context, standard O2 therapy delivered by nasal cannula or an air-entrainment mask is the standard of care to improve postoperative hypoxemia. However, when standard O2 fails in this intent, noninvasive ventilation is often used to treat arterial de-oxygenation.8
Recently, oxygen therapy by high-flow nasal cannula (HFNC) has been largely used in clinical practice due to its capability to deliver heated and humidified air flow (up to 60 L/min) through ease-of-use and noninvasive nasal prongs. HFNC allows better control of FIO2, generates low levels of PEEP, and decreases physiologic dead space by washout of the pharynx, which thus reduces the work of breathing and dyspnea. Furthermore, gas humidification and heating improve both mucociliary motion and patient comfort. Moreover, HFNC has received increasing interest by the scientific community because of its better performance in minimizing postextubation lung de-recruitment and improving oxygenation compared with standard O2.9,10 There is increasing evidence of the superiority of HFNC compared with standard O2 in reducing intubation rates and ICU length of stay in patients who are critically ill with acute hypoxemic respiratory failure 10,11 or at risk for re-intubation.12,13
To date, few studies have been published on HFNC application after extubation in major abdominal surgery.14,15 However, to our knowledge, no study has assessed the effect of HFNC oxygen therapy to prevent hypoxemia after extubation in patients who underwent liver transplantation. We performed a prospective observational study in subjects admitted to the ICU after liver transplantation and compared this group with an historical cohort matched for baseline characteristics to test the hypothesis that the prophylactic use of HFNC oxygen therapy is more effective in preventing hypoxemia after extubation than standard O2 therapy.
QUICK LOOK
Current knowledge
Patients undergoing liver transplantation usually have several concomitant morbidities that increase the risk of postextubation hypoxemia and postoperative pulmonary complications. Oxygen therapy via high-flow nasal cannula (HFNC) has been widely used in patients who are critically ill with acute respiratory failure.
What this paper contributes to our knowledge
In subjects with liver transplantation, compared with subjects who were critically ill with acute hypoxemic respiratory failure, the routine use of HFNC oxygen therapy did not significantly impact the rate of hypoxemia over the first 24 h after elective extubation. In this specific population, the risk of postoperative pulmonary complications and of consequent gas exchange impairment was not affected by the system used to deliver oxygen therapy in the postoperative period.
Methods
Subject Characteristics
We included all consecutive patients admitted to the 13-bed ICU of a tertiary teaching hospital in Rome who underwent liver transplantation for end-stage liver disease and/or hepatocellular carcinoma and for whom extubation was considered safe by the treating physician. The ethics institutional review committee at Fondazione Policlinico Universitario A Gemelli Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS) approved the study (approval 14923/18). Subjects who were included in the study or the next of kin gave consent to participate before inclusion. The study was registered on ClinicalTrials.gov (reference NCT03441854). We excluded patients ages < 18 y, with acute liver failure, previous cardiopulmonary resuscitation, hemodynamic instability (defined as one mean arterial pressure ≤ 65 mm Hg, vasopressors, cardiac ischemia, or arrhythmias), tracheotomy, hemorrhagic diathesis, sepsis or septic shock, or primary graft dysfunction, or those who were extubated in the operating room.
Study Protocol
All the subjects were admitted to the ICU deeply sedated, intubated, and on mechanical ventilation. According to hospital protocol, extubation was deemed safe when all the following criteria were verified: hemodynamic and metabolic stability, Glasgow Coma score ≥ 13, PaO2/FIO2) ≥ 300 mm Hg, breathing frequency ≤ 25 breaths/min, no clinical signs of respiratory distress (dyspnea, significant use of accessory muscles, or paradoxical abdominal motion), excessive orotracheal secretions, low pressure support, and PEEP requirement. Subjects who fulfilled these criteria underwent a spontaneous breathing trial with either a T-piece or pressure support of 7 cm H2O and PEEP of 0 cm H2O for 30 to 120 min.
Only subjects who showed no signs of respiratory fatigue or hypoxemia and/or hypercapnia with pH derangement were extubated and started on prophylactic oxygen therapy by using either HFNC (HFNC group) or air-entrainment mask (standard O2 group) with FIO2 titrated to maintain an SpO2 of at least 93%, for 24 h. The HFNC group received high-flow oxygen via the mechanical ventilator (Servo U, Maquet, Wayne, New Jersey) at a mean ±SD gas flow of 50 ± 10 L/min through an MR850 heated humidifier and a RT202 breathing circuit (Optiflow; Fisher & Paykel Heathcare, Auckland, New Zeland). The gas mixture was heated and humidified at 37°C and delivered to the patient through large-bore binasal prongs. The standard O2 group was chosen from a group of 90 subjects with liver transplantation from the hospital database, admitted to the same ICU between January 1, 2015, and December 31, 2017. All the subjects received the same postoperative analgesia protocol based on remifentanil infusion.
Preventive oxygen therapy was discontinued if the patient developed moderate acute hypoxemic respiratory failure (at least 2 of the following criteria: (1) breathing frequency >25 and < 35 breaths/min persistent for at least 1 h, (2) clinical signs of respiratory distress, (3) respiratory acidosis (pH < 7.35 units and PaCO2 > 45 mm Hg), (4) moderate hypoxemia defined as PaO2/FIO2 > 150 and < 300. In such situations, noninvasive ventilation was delivered by full-face or oronasal mask. If the subjects developed one of the following conditions: (1) hemodynamic instability, (2) agitation that required deep pharmacologic sedation, (3) surgical complication that required an urgent operative procedure, and (4) severe acute hypoxemic respiratory failure (at least 2 of the following criteria: clinical signs of respiratory distress, frequency >40 breaths/min, respiratory acidosis with arterial pH ≤ 7.30, and PaCO2) > 45 mm Hg, and severe hypoxemia defined as PaO2/FIO2 ≤ 100), endotracheal intubation was performed.
End Points
The primary end point of the study was the incidence of hypoxemia at 1 h and at 24 h after extubation. Hypoxemia was defined as PaO2/FIO2 of <300.13 Secondary end points were the following: pH, PaO2, and PaCO2 at 1 h and at 24 h after extubation, weaning failure (defined as the need for endotracheal intubation or noninvasive ventilation, infectious pulmonary complication during the first 48 h after extubation16), ICU length of stay, and 28-d mortality. Pulmonary infection was defined as a new infiltrate on chest radiograph, and two of the following clinical signs: body temperature > 38°C or < 35°C, leukocyte count > 10 × 103/mm3 or < 4 × 103/mm3, or purulent tracheal secretions.17
Measurements
Baseline assessment included age, sex, body mass index, the presence of diabetes mellitus, etiology of chronic liver disease, Model for End-Stage Liver Disease score, degree of hepatic encephalopathy, cardiac function assessed by bedside echocardiography (left ventricular ejection fraction and systolic pulmonary arterial pressure), the ARISCAT (Assess Respiratory Risk in Surgical Patients in Catalonia) risk index18 for developing postoperative pulmonary complications (low risk if < 26 points, intermediate if > 26 points and < 45 points, high if > 45 points), and preoperative pulmonary function tests. The pulmonary function tests included the value of FEV1, FVC, and the total lung capacity. On the basis of pulmonary function tests,19 the subjects were divided into 3 classes: restrictive (total lung capacity < 80% of the predicted), obstructive (FEV1/FVC < 70% of the predicted), and normal pattern. In addition, arterial pH, PaO2, and PaCO2 before surgical procedure were also recorded.
Intraoperative parameters included the duration of surgery and blood product requirement (erythrocytes, fresh frozen plasma, and platelets). Ascites was defined as mild (<5 L) or moderate-severe (≥5 L) according to the volume drained during surgery. Postoperative variables included the following: Simplified Acute Physiology Score II, length of invasive mechanical ventilation before extubation, gas exchange values (arterial pH, PaO2, PaCO2), breathing frequency, and SpO2 before extubation, at 1 h and at 24 h after extubation, chest radiograph evaluation (atelectasis, pleural effusion, interstitial and/or alveolar edema, and suspected pneumonia) before and after extubation.
Statistical Analysis
A review of data from our database over a 6-y period (2012–2017) revealed that ∼ 50% of patients with liver transplantation developed hypoxemia at 1 h after extubation when treated with standard O2 via an air-entrainment mask. A sample size of 25 for each group provided 80% power to detect a reduction of hypoxemia from 50% to 15% (alpha = 0.05). We did a 1:1 matching between the HFNC group and standard O2 group according to age, liver dysfunction assessed by Model for End-Stage Liver Disease, severity of illness at ICU admission assessed by Simplified Acute Physiology Score II, and body mass index. Continuous data were expressed as mean ± SD. Categorical data were presented as number and percentage. Comparisons were made by using the Student t test and Fisher exact test, as appropriate. A P value of <.05 was considered statistically significant. Statistical analysis was performed by using MEDcalc version 18.6 (MedCalc Software, Mariakerke, Belgium).
Results
Baseline Characteristics
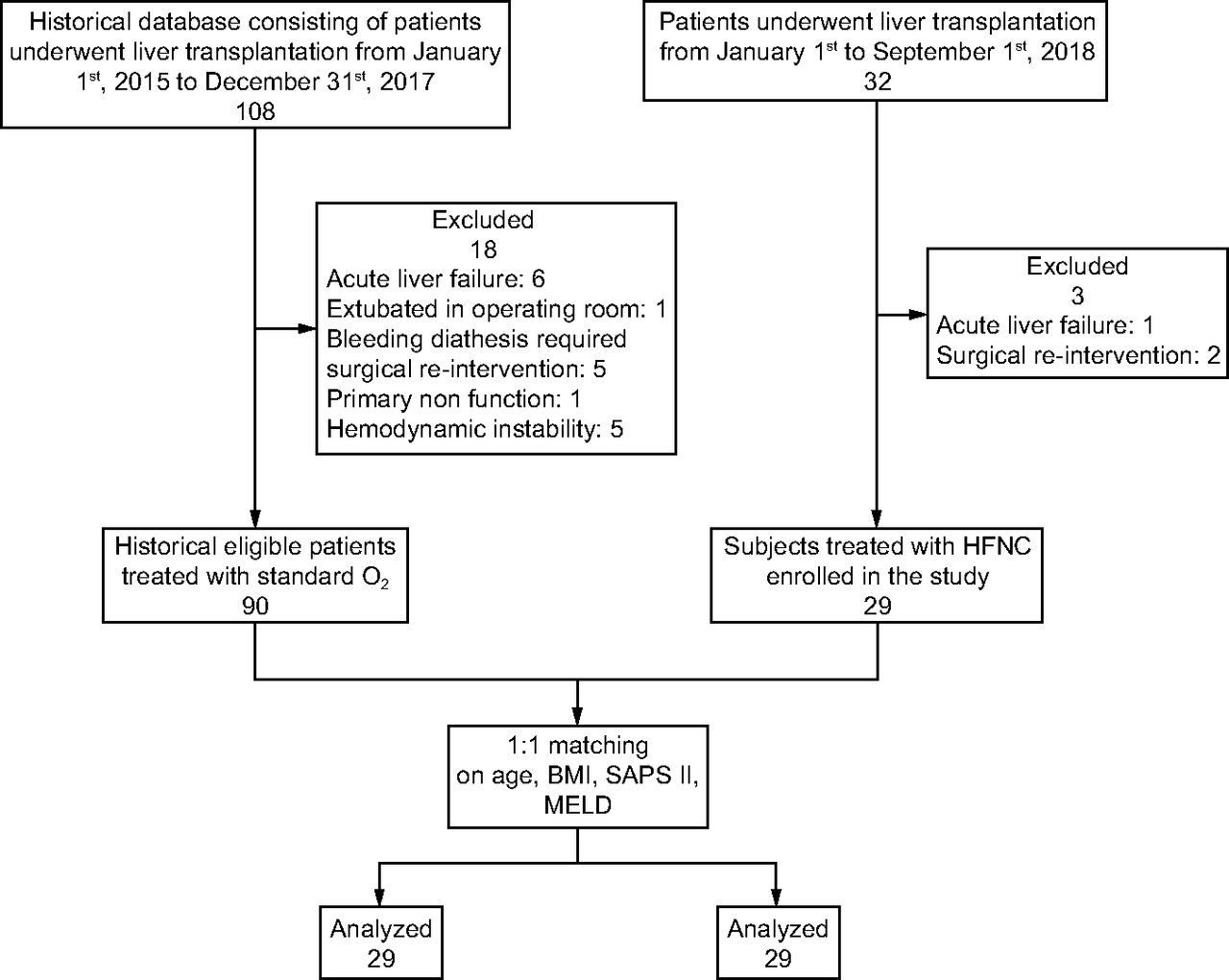
Between January 1 and September 1, 2018, 32 adult patients were admitted to the ICU after liver transplantation. Three patients were not included in the analysis because of acute liver failure (n = 1) and hemorrhagic diatheses (n = 2). The remaining 29 subjects had preventive HFNC oxygen therapy after extubation and were matched with 29 controls who were selected from an historical group of 90 patients treated with preventive standard O2 via air-entrainment mask (Fig. 1).

Flow chart. HFNC = high-flow nasal cannula; BMI = body mass index; SAPS II = Simplified Acute Physiology Score II; MELD = Model for End-Stage Liver Disease.
Baseline characteristics of standard O2 and HFNC groups are shown in Table 1. Both groups had comparable demographic characteristics; however the mean ± SD PaCO2 was lower in the standard O2 group compared with the HFNC group (32.36 ± 3.28 mm Hg and 36.00 ± 4.77 mm Hg, respectively, P < .01). The mean ± SD volume of ascites drained during surgery was larger in standard O2 group than in the HFNC group (4.64 ± 3.85 L vs 2.31 ± 3.19 L, P < .01, respectively). The duration of invasive mechanical ventilation before extubation as well as chest radiograph that documented pleural effusion were similar between both groups (Table 1). One subject in each group started continuous renal replacement therapy before liver transplantation for acute kidney injury.
Baseline Characteristics of the Subjects
Primary Outcome
No significant difference was observed between the standard O2 group versus HFNC group for the incidence of hypoxemia at 1 h (48% vs 41%, P = .59) and 24 h (34% vs 45%, P = .41) after extubation. Furthermore, the mean ± SD PaO2/FIO2 during hypoxemic episodes was similar between both groups at 1 h (242.75 ± 39.69 mm Hg vs 263.20 ± 49.23 mm Hg), and at 24 h after extubation (243.23 ± 41.77 mm Hg vs 262.42 ± 39.47 mm Hg).
Secondary Outcomes
The mean ± SD PaCO2 at 1 h after extubation was lower in the HFNC group compared with the standard O2 group (36.6 ± 4.3 vs 39.0 ± 6.7, P = .04), whereas no difference was observed at 24 h. We did not observe differences in the rate of weaning failure or ICU length of stay or 28-d mortality (Table 2).
Respiratory Variables and Secondary Outcomes
Adverse Events
No subjects required HFNC therapy interruption due to intolerance, although 10% of the subjects requested air-flow reduction immediately after the beginning of HFNC due to dryness of nasal mucosa.
Discussion
In this observational matched controlled study, the preventive application of oxygen therapy with HFNC after extubation in the subjects with liver transplantation did not reduce the incidence of hypoxemia compared with standard O2 via air-entrainment mask. Also, the preventive use of HFNC oxygen therapy did not decrease the rate of weaning failure, ICU length of stay, and 28-d mortality. Accordingly, these results implied that the use of preventive oxygen therapy by HFNC did not have a superior impact on arterial oxygenation or related respiratory outcomes compared with standard O2. However, HFNC did not increase the risk of postoperative pulmonary complications and was associated with a trend toward reduced weaning failure.
Patients who are admitted to the ICU after liver transplantation are at increased risk of hypoxemia and postoperative pulmonary complications for several reasons.20 The transplantation procedure itself causes bilateral transection of the abdominal muscles and chest-wall damage due to retractor use, which amplifies diaphragmatic impairment.20–25 Furthermore, these patients present with many concomitant morbidities, such as poor muscle mass, sarcopenia, hypoalbuminemia, and restrictive lung volumes due to ascites and pleural effusion. They also have to endure the effects of an extremely invasive surgery that may prolong the duration of mechanical ventilation, which increases the incidence of hypoxemia and the re-intubation rate after extubation. Although not supported by our findings, the application of increased flows by HFNC has been shown to progressively reduce inspiratory effort and improve lung aeration, dynamic compliance, and oxygenation in patients who are critically ill with acute hypoxemic respiratory failure.26 HFNC oxygen therapy has been widely used for patients of all age groups with respiratory failure of several etiologies, including preterm infants and adult medical and surgical patients who are critically ill. Unique features of HFNC lie in its simplicity of use and its remarkable tolerance and comfort.
To date, few studies have evaluated preventive HFNC application after extubation in abdominal surgery in heterogeneous populations.14,15 Overall, abdominal surgery can lead to postoperative pulmonary complications by altering diaphragmatic function and contractility, which causes reduced lung volumes and flows, which predisposes to lower-lobe atelectasis.1–4,27 Among the surgical population, the role of HFNC in preventing deterioration in pulmonary function after surgery is poorly defined. In cardiac surgery, results of studies demonstrated that prophylactic HFNC postextubation did not lead to improvements in pulmonary function or postoperative oxygenation in subjects with a body mass index ≥ 30 kg/m2.28,29 Conversely, in patients who underwent thoracoscopic lobectomy, oxygen therapy by HFNC improved oxygenation and reduced the risk of re-intubation, although it did not decrease the incidence of postoperative pulmonary complications.30
Our results concurred with a multicenter randomized control trial in which Futier et al14 found nonsuperiority of HFNC compared with standard O2 to prevent respiratory deterioration (incidence of hypoxemia, postoperative pulmonary complications, and length of hospital stay) after extubation in major elective abdominal surgery. However, Dhillon et al 15 showed that HFNC was associated with a lower risk of re-intubation compared with conventional oxygen therapy, although interpretation of these results is limited by the retrospective nature of the study.
According to Futier et al,14 HFNC application did not reduce the risk of pneumonia compared with standard O2. This finding is contrary to physiologic evidence that demonstrates the role of high-flow humidified oxygen to improve mucociliary function, secretion mobilization, and lung recruitment by PEEP.31 However, lung de-recruitment and atelectasis after extubation following general anesthesia may persist more than 24 h and is worsened by the negative effect of muscular paralysis on respiratory mechanics, patient inspiratory effort, and gas exchange.23,32,33
More recently, Azoulay et al34 randomized 776 immunocompromised and critically ill subjects with hypoxemic acute respiratory failure, to receive standard oxygen therapy or HFNC. The primary outcome of the study was 28-d mortality, and secondary outcomes were intubation and mechanical ventilation by day 28, PaO2/FIO2 over 3 d after intubation, breathing frequency, ICU, and hospital length of stay, ICU-acquired infections, patient comfort, and dyspnea.34 The investigators found no significant reduction in 28-d mortality by using HFNC compared with standard oxygen therapy.34 In accordance with the clinical trial by Azoulay34 (with 19 subjects with liver transplantation), we also found no significant difference for the 28-d mortality or ICU length of stay when comparing these modalities.
In a recent prospective randomized crossover study, Mauri et al26 assessed the effect of HFNC delivered at increasing flow on inspiratory effort and the work of breathing in subjects with acute hypoxemic respiratory failure. In this cohort, the investigators demonstrated that increasing HFNC flows progressively decreased inspiratory effort and improved lung aeration and dynamic compliance.26 Furthermore, the results of this study showed that the effect on inspiratory work load and CO2 clearance was already obtained at the lowest flow.26 In our trial, we observed a significantly lower PaCO2 1 h after extubation in the HFNC group. In fact, the literature reports reduced anatomic dead space due to increased nasopharyngeal washout, with a consequently larger fraction of minute ventilation participating in gas exchange.35 Frequently, candidates for liver transplantation display a restricted respiratory pattern related to the size of the ascites and/or pleural effusion.36 In fact, in our population, we detected a significantly low preoperative PaCO2, especially those in the standard O2 group who had more ascites. This condition was solved by the liver transplantation.37
To the best of our knowledge, this was the first clinical study that explored the usefulness of the preventive application of HFNC after elective extubation in subjects who were undergoing liver transplantation. Another strength of our study was the selection of a specific patient population at increased risk for postoperative pulmonary complications demonstrated by the moderately high ARISCAT index. These issues led to the wide spread application of HFNC in these patients at high risk. Furthermore, the use of a high-flow system was economical because it was integrated into the ICU ventilator, therefore, no new equipment charge was applied. This finding was contrary to the results of Mayordormo-Colunga and Medina,38 who evaluated clinical and cost-effectiveness of HFNC compared with noninvasive ventilation. The investigators concluded that the cost of acquiring HFNC equipment is not currently justified, because HFNC is not superior to noninvasive ventilation in many clinical scenarios, and most pediatric and adult ICUs already have noninvasive ventilation devices.
Study Limitations
We acknowledge that this study had some limitations. First, this was not a randomized control trial. Second, this study was conducted in a single center with a relatively small sample size. Third, the aim of study was to evaluate HFNC efficacy compared with standard O2, without analyzing modifications in respiratory mechanics during the utilization of different oxygenation techniques. Fourth, we did not measure actual delivered FIO2 with either the HFNC or air-entrainment mask because this would have required invasive maneuvers, such as the insertion of a nasopharyngeal catheter.39 These maneuvers could decrease patient comfort, which thus affected our results.
Conclusions
Preventive application of HFNC after extubation in subjects with liver transplantation did not reduce the incidence of hypoxemia in comparison with standard O2 via an air-entrainment mask. Moreover, among this high-risk population of subjects who were immunocompromised, HFNC did not reduce weaning failure, ICU length of stay, or 28-d mortality compared with standard O2. Further studies are needed to identify the subset of patients with liver transplantation who are the best candidates to benefit from HFNC.
Footnotes
- Correspondence: Rita Gaspari MD, Department of Intensive Care and Anesthesia, Fondazione Policlinico Universitario A Gemelli IRCCS, Largo Agostino Gemelli 8,00168 Rome, Italy. E-mail: rita.gaspari{at}policlinicogemelli.it.
The authors have disclosed no conflicts of interest.
See the Related Editorial on Page 131
- Copyright © 2020 by Daedalus Enterprises









{kind=link}