

Abstract
BACKGROUND: Patients undergoing mechanical ventilation in the ICU often receive supplemental oxygen. If not closely monitored, this may lead to hyperoxia. The use of an oxygen-weaning protocol may reduce this risk by pacing the titration of oxygen therapy to patient needs. ICU protocols are correlated with decreased mortality and length of stay and have great potential for cost savings. The goals of this study were to determine whether the oxygen-weaning protocol at a university-affiliated hospital was followed and to measure the length of time respiratory therapists took to wean patients once the oxygen-weaning parameters were met.
METHODS: This was a retrospective chart review of subjects > 18 y of age admitted to the medical ICU who underwent intubation and mechanical ventilation and were placed on an oxygen therapy protocol. The following data were collected: demographics, arterial blood gases, the length of time to change  after meeting weaning parameters, and the percent change in
after meeting weaning parameters, and the percent change in  .
.
RESULTS: Data were collected from 30 subjects. The most common oxygen saturation parameter measured via pulse oximetry ( ) used to initiate weaning oxygen was 92%. The mean ± SD
) used to initiate weaning oxygen was 92%. The mean ± SD  administered to subjects was 39.6 ± 15.3% prior to extubation. The majority of subjects exhibited adequate oxygenation prior to extubation (mean ± SD):
administered to subjects was 39.6 ± 15.3% prior to extubation. The majority of subjects exhibited adequate oxygenation prior to extubation (mean ± SD):  99.3 ± 6.7 mm Hg,
99.3 ± 6.7 mm Hg,  95.1 ± 26.9%. The mean ± SD length of time to the first change in
95.1 ± 26.9%. The mean ± SD length of time to the first change in  from the time a subject met the weaning criteria was 9.1 ± 10.6 h (range 1–39 h; interquartile range 2–13 h).
from the time a subject met the weaning criteria was 9.1 ± 10.6 h (range 1–39 h; interquartile range 2–13 h).
CONCLUSIONS: Subjects admitted to the medical ICU who were intubated, mechanically ventilated, and placed on the oxygen therapy protocol experienced a significant delay in oxygen weaning. Closer monitoring and adherence to the oxygen-weaning protocol should be considered to reduce the potential risk for hyperoxia.
- oxygen weaning
- weaning protocols
- oxygen titration protocol
- patient-driven protocols
- protocol adherence
- weaning indices
Introduction
Patients in the medical ICU are frequently treated with supplemental oxygen. Unfortunately, when oxygen therapy is not closely monitored, it may lead to hyperoxia. Oxygen-weaning protocols serve as a guide to titrate the oxygen concentration based on a patient’s needs. The idea that you can’t give too much oxygen is a common misconception.1,2 Oxygen is a drug and, like any other drug, too much oxygen can be dangerous. Hyperoxia is a state of excess oxygen concentration, and hyperoxemia is the state of higher than normal arterial oxygen levels.3 Administering oxygen at higher concentrations for prolonged periods of time is associated with longer hospital stay, long-term mortality, and an increased risk of death.4 Hyperoxia is a well-known adverse effect of oxygen therapy, yet it is routinely underestimated by most clinicians. Observational studies have reported that subjects in the ICU are regularly managed with excessive  and remain hyperoxemic for long periods of time.2,3
and remain hyperoxemic for long periods of time.2,3
Oxygen-weaning protocols and guidelines are designed to pace the titration of oxygen therapy to prevent complications and improve outcomes.5 Applying the steps of a weaning protocol is essential to improve patient outcomes.6 The use of respiratory care protocols has been shown to enhance the quality of care as well as reduce the misallocation of resources, resulting in a significant reduction in mortality.7-9 Yet titration of oxygen therapy is not performed in a timely manner despite the presence of oxygen saturation as measured via pulse oximetry ( ) or
) or  levels significantly above ordered weaning parameters.10
levels significantly above ordered weaning parameters.10
Metcalf et al11 recently evaluated the effectiveness of oxygen-weaning protocols and reported that a considerable number of subjects in the ICU receiving oxygen may be routinely monitored with pulse oximetry but do not have the correct oxygen therapy prescriptions. Implementation and adherence to respiratory care protocols may depend on the respiratory therapist’s perception of the importance of such practices to ensure patient safety.
The goals of this study were to determine whether the oxygen-weaning protocol at a university-affiliated hospital was followed and to measure the length of time respiratory therapists took to wean patients once the oxygen-weaning parameters were met.
Quick Look
Current Knowledge
Oxygen therapy is used on a daily basis to treat acute hypoxemic respiratory failure, and oxygen protocols are used to titrate  . The safety of oxygen protocols in the mechanically ventilated patient and risk of hyperoxia or refractory hypoxemia have seldom been studied.
. The safety of oxygen protocols in the mechanically ventilated patient and risk of hyperoxia or refractory hypoxemia have seldom been studied.
What This Paper Contributes to Our Knowledge
We reviewed the use of oxygen therapy protocols for intubated patients and investigated the adherence to an oxygen protocol for the mechanically ventilated patient in the medical ICU during a 4-month period. Delay of oxygen titration occurred in most subjects. Therefore, it is recommended to develop, implement, and adopt an evidence-based multidisciplinary oxygen protocol in the medical ICU.
Methods
A retrospective chart review was conducted using electronic medical records at a university-affiliated, 496-bed hospital in San Antonio, Texas. Subjects ≥ 18 y old admitted to the medical ICU between January 1, 2017, and April 30, 2017, who were receiving oxygen therapy while undergoing mechanical ventilation and had orders for the oxygen protocol, were included in the study. Upon accessing the electronic medical records, only patients admitted to the ICU beginning with day 1 of the study period and meeting criteria were sequentially included in the study until a convenience sample of 30 subjects was reached. The study was approved by the institutional review board at the University of Texas Health Science Center at San Antonio and University Health System.
Data Collection
The following data were collected for the study: gender, date of admission, race, ethnicity, admitting diagnosis, PEEP,  , and arterial blood gases including the date, time,
, and arterial blood gases including the date, time,  ,
,  , and
, and  . In addition to each subject’s baseline oxygen data, the time difference between the subject meeting the minimum
. In addition to each subject’s baseline oxygen data, the time difference between the subject meeting the minimum  ordered by the physician to start the weaning protocol and the time the change in
ordered by the physician to start the weaning protocol and the time the change in  occurred were measured. Baseline
occurred were measured. Baseline  and percent change were also recorded after each
and percent change were also recorded after each  adjustment. The length of time to change
adjustment. The length of time to change  after meeting titration parameters and the percent change in
after meeting titration parameters and the percent change in  were calculated and used for analysis.
were calculated and used for analysis.
Outcomes
The primary outcome was the time to wean in minutes/h from the point the subject started mechanical ventilation, had specific orders for the oxygen-weaning protocol, and met the criteria to wean from oxygen therapy to the first weaning attempt documented.
Statistical Analysis
All statistical analyses were performed using SPSS 25 (IBM, Armonk, New York). One-sample Wilcoxon test was used to determine group medians. Two-tailed Pearson correlation was used to determine whether time in hours to first change in  was associated with initial PEEP,
was associated with initial PEEP,  ,
,  , or
, or  /
/ values. Correlation was considered statistically significant at P < .05.
values. Correlation was considered statistically significant at P < .05.
Results
Data were collected from 30 subjects ≥ 18 y old who were admitted to the medical ICU from January 1, 2017, and April 30, 2017, were receiving oxygen therapy while undergoing mechanical ventilation, and had orders for the oxygen protocol. The mean ± SD age was 54.2 ± 14.7 y. There were 14 men (46.6%) and 16 women (53.4%) in this sample. The subjects’ baseline admission diagnoses characteristics are listed in Table 1.
Admission Diagnoses
The most common  parameter used in the medical ICU to initiate weaning oxygen was 92% (n = 18), followed by
parameter used in the medical ICU to initiate weaning oxygen was 92% (n = 18), followed by  > 90% (n = 11). One subject was weaned at
> 90% (n = 11). One subject was weaned at  > 95%. The mean
> 95%. The mean  ,
,  , and
, and  /
/ values from the arterial blood gas that was obtained prior to the initiation of weaning from mechanical ventilation were 103.8 mm Hg, 92.5%, and 177, respectively (Table 2).
values from the arterial blood gas that was obtained prior to the initiation of weaning from mechanical ventilation were 103.8 mm Hg, 92.5%, and 177, respectively (Table 2).
Oxygenation Status Prior to Initiation of Weaning
The mean ± SD level of PEEP used for most subjects was 6.3 ± 2.01 cm H2O (range 5–10; interquartile range [IQR] 5–8). The mean  administered to these subjects before initiating weaning was 63.8 ± 28.9% (range 21–100; IQR 40–60). The median time to first change in
administered to these subjects before initiating weaning was 63.8 ± 28.9% (range 21–100; IQR 40–60). The median time to first change in  when subjects met weaning criteria was 5 h (mean 9.1 ± 10.6 h; range 1–39; IQR 2–13) (Fig. 1). Almost half of the subjects (46.9%) were weaned within 4 h of meeting the criteria; for 30.0% of the subjects, it took 12 h to make the first change in
when subjects met weaning criteria was 5 h (mean 9.1 ± 10.6 h; range 1–39; IQR 2–13) (Fig. 1). Almost half of the subjects (46.9%) were weaned within 4 h of meeting the criteria; for 30.0% of the subjects, it took 12 h to make the first change in  after meeting criteria (Fig. 2).
after meeting criteria (Fig. 2).
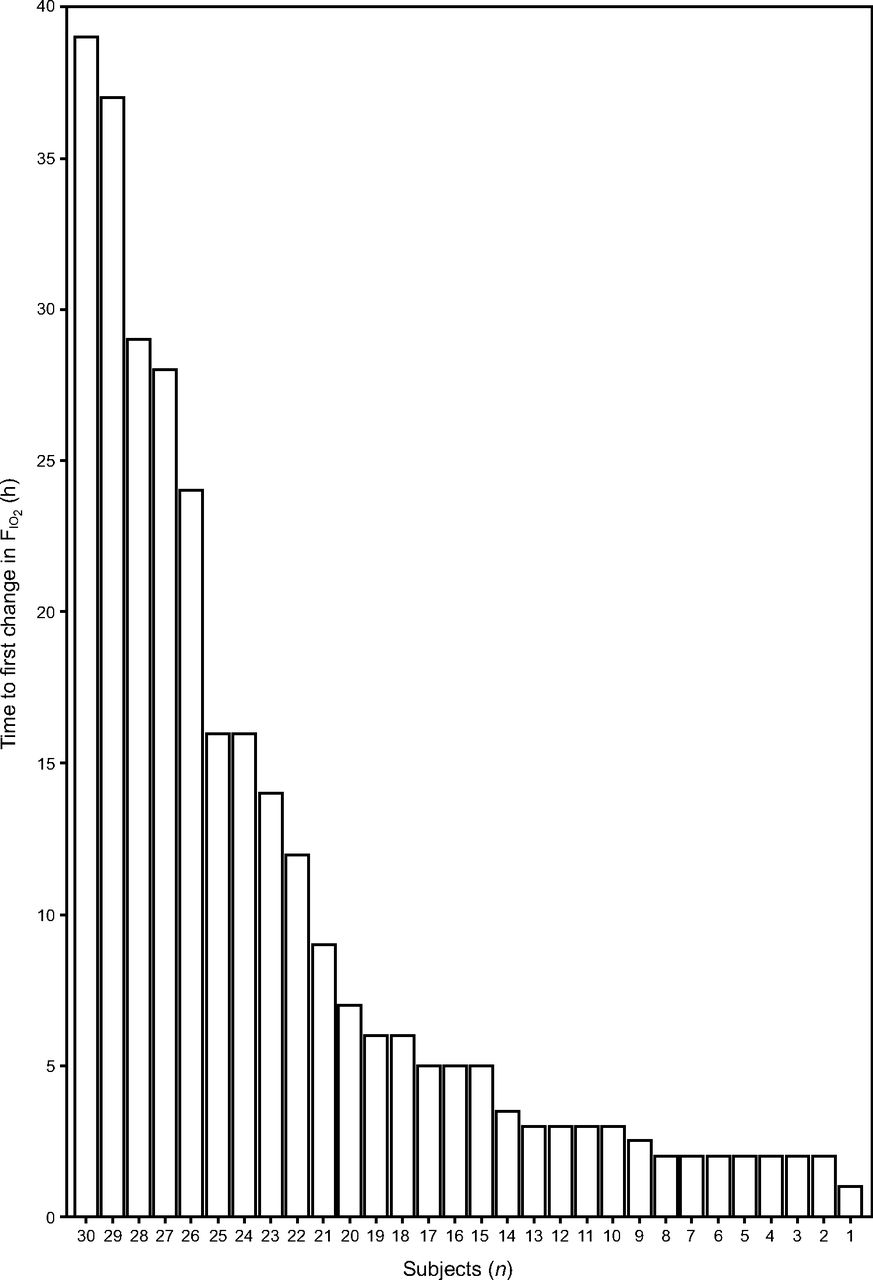
Time of first  change after meeting weaning criteria.
change after meeting weaning criteria.
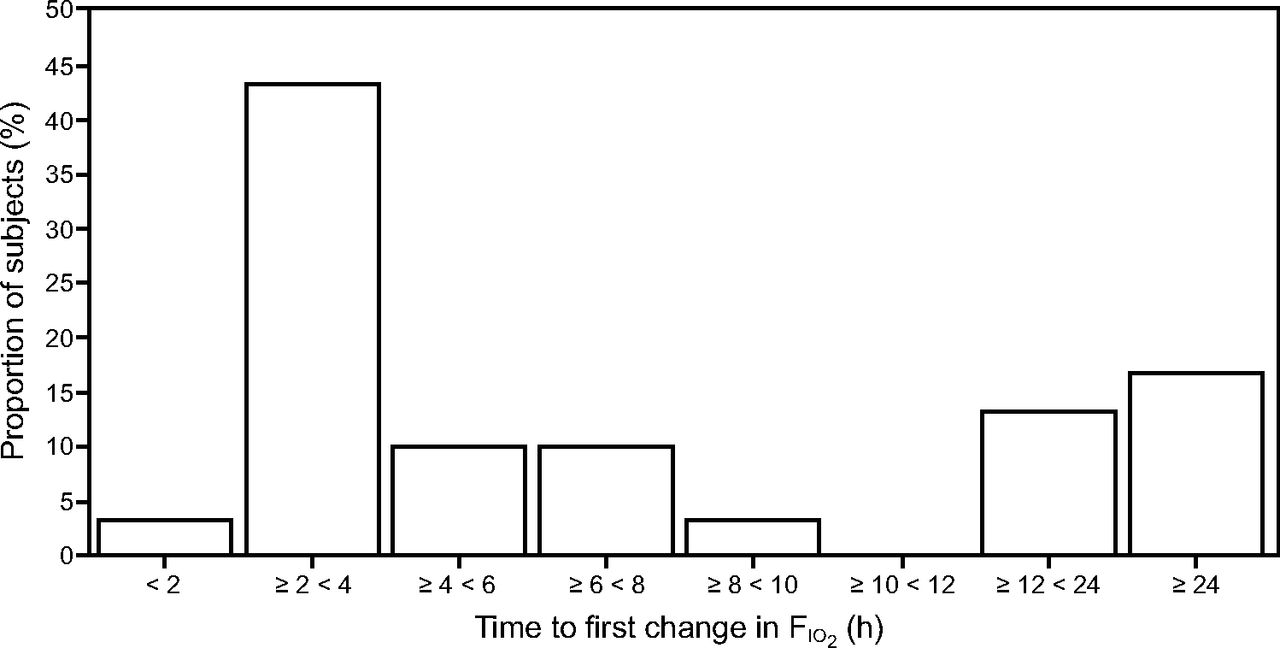
Percent of subjects in whom  was changed over time after meeting weaning criteria.
was changed over time after meeting weaning criteria.
The mean ± SD percent change in  when the change was performed was 21.9 ± 14.3%; range 10–60; IQR 12–30). The average number of hours that subjects were administered oxygen therapy was 21.5 ± 27.6 h after they no longer required oxygen per the protocol. There were no correlations between time to first change in
when the change was performed was 21.9 ± 14.3%; range 10–60; IQR 12–30). The average number of hours that subjects were administered oxygen therapy was 21.5 ± 27.6 h after they no longer required oxygen per the protocol. There were no correlations between time to first change in  and initial PEEP (r = −0.029, P = .88),
and initial PEEP (r = −0.029, P = .88),  (r = 0.149, P = .44),
(r = 0.149, P = .44),  (r = 0.314, P = .09), and
(r = 0.314, P = .09), and  /
/ (r = 0.265, P = .17).
(r = 0.265, P = .17).
Discussion
The purpose of this study was to evaluate adherence to an oxygen protocol for titration in adult patients undergoing mechanical ventilation admitted to a medical ICU and to measure the time required to wean subjects once the oxygen-weaning parameters were met. The results indicate that the oxygen protocol was not routinely followed and that patients might remain at a higher-than-required  after meeting the criteria for weaning for an excessive length of time.
after meeting the criteria for weaning for an excessive length of time.
Most critical care patients who are intubated and mechanically ventilated are administered supplemental oxygen therapy with an  values of 0.21–1.0, which is adjusted to meet the patient’s needs. However, the safest level of oxygen for these critically ill patients is unknown.12 Helmerhorst et al13 reported increased mortality with marked hyperoxia (> 200 mm Hg) and time spent in this hyperoxic state has a linear relationship with hospital mortality.
values of 0.21–1.0, which is adjusted to meet the patient’s needs. However, the safest level of oxygen for these critically ill patients is unknown.12 Helmerhorst et al13 reported increased mortality with marked hyperoxia (> 200 mm Hg) and time spent in this hyperoxic state has a linear relationship with hospital mortality.
Although none of the studies reviewed reported on adherence to oxygen therapy protocols for intubated subjects by respiratory therapists in adult ICUs, there are a number of studies that reviewed the effects of hyperoxia and the effectiveness of using oxygen therapy protocols.3,6,9 Holbourn et al5 investigated supplemental oxygen prescription at Waikato Hospital and reported that, of the 120 subjects, only 51.7% had correct oxygen therapy orders. The study emphasized that clinicians should adequately evaluate the oxygen needs of subjects and consistently follow a safe oxygen protocol.5 A recent online survey of personnel in 45 hospitals conducted by Metcalf et al11 stated that, among the health care providers surveyed, oxygen titration and ventilator weaning are the most commonly used protocols within these critical care facilities. After comparing 9 different respiratory care protocols, (ie, asthma, COPD, ARDS, hypoxemia, pneumonia, noninvasive ventilation therapy, supplemental oxygen titration and discontinuation, ventilator weaning, and bronchopulmonary hygiene), respondents felt that the use of protocols enhanced cost and quality of care. The study also noted that larger hospitals (ie, > 350 beds) use protocols more widely than smaller hospitals.11 These findings are similar to the setting of our study, which occurred in a large academic medical center.
A study by Jochmans et al14 reported that the measured  for subjects in the ICU was within the predicted range only 64% of the time, and there was a clear trend toward hyperoxygenation in the mechanically ventilated subjects (odds ratio 1.3, 95% CI 1.22–1.38, P < .001). Furthermore, Rachamle et al15 reported that 74% of mechanically ventilated subjects were exposed to excessive
for subjects in the ICU was within the predicted range only 64% of the time, and there was a clear trend toward hyperoxygenation in the mechanically ventilated subjects (odds ratio 1.3, 95% CI 1.22–1.38, P < .001). Furthermore, Rachamle et al15 reported that 74% of mechanically ventilated subjects were exposed to excessive  , which was correlated with a worse oxygenation index in a dose-response manner. Our results are consistent with these findings associated with hyperoxia, and, although we did not calculate the oxygen index, it can be inferred. The exposure of patients to hyperoxia is likely to be harmful in the ICU, and this phenomenon often goes unnoticed. Damiani et al16 conducted a study among 189,143 subjects who suffered from a stroke, traumatic brain injury, or cardiac arrest and noted that hyperoxia was associated with increased mortality in post-cardiac arrest subjects (odds ratio 1.42, 95% CI 1.04–1.92), stroke (odds ratio 1.23, 95% CI 1.06–1.43), and traumatic brain injury (odds ratio 1.41, 95% CI, 1.03–1.94). Eastwood et al17 reported that using a target oxygen saturation range of 88–92% was feasible for mechanically ventilated cardiac arrest survivors and resulted in more use of spontaneous ventilation modes, more ventilation on room air (
, which was correlated with a worse oxygenation index in a dose-response manner. Our results are consistent with these findings associated with hyperoxia, and, although we did not calculate the oxygen index, it can be inferred. The exposure of patients to hyperoxia is likely to be harmful in the ICU, and this phenomenon often goes unnoticed. Damiani et al16 conducted a study among 189,143 subjects who suffered from a stroke, traumatic brain injury, or cardiac arrest and noted that hyperoxia was associated with increased mortality in post-cardiac arrest subjects (odds ratio 1.42, 95% CI 1.04–1.92), stroke (odds ratio 1.23, 95% CI 1.06–1.43), and traumatic brain injury (odds ratio 1.41, 95% CI, 1.03–1.94). Eastwood et al17 reported that using a target oxygen saturation range of 88–92% was feasible for mechanically ventilated cardiac arrest survivors and resulted in more use of spontaneous ventilation modes, more ventilation on room air ( = 0.21), and shorter length of stay in a critical care unit. In addition, a post hoc analysis of the PROXI trial identified the potential risks of acute coronary syndromes associated with perioperative hyperoxia.7
= 0.21), and shorter length of stay in a critical care unit. In addition, a post hoc analysis of the PROXI trial identified the potential risks of acute coronary syndromes associated with perioperative hyperoxia.7
A systematic review by Chu et al18 reviewed the safety of liberal vs conservative oxygen therapy in acutely ill adults. They reported that hyperoxia resulted in higher in-hospital and 30-d morbidity rates as well higher mortality at 30 d.18 Chu and colleagues also noted across institutions that oxygen saturations of ≥ 96% (range 94–99%, IQR 96–98%) increased mortality both in hospital and in follow-up periods postdischarge.18 These potential adverse events related to hyperoxia clearly command consideration in avoiding unnecessary oxygen administration.18 L’Her et al reported in their randomized controlled trial that hyperoxia can be reduced with an automated oxygen-titration system.19 These studies emphasize the importance of our findings related to excessive periods of hyperoxia and emphasize the need for close adherence to oxygen therapy protocols to improve patient safety and outcomes. Suzuki and colleagues20,21 established that conservative oxygen therapy for subjects undergoing mechanical ventilation (target  = 90–92%) was feasible and free of adverse outcomes while allowing a marked decrease in excess oxygen exposure. Subjects in this conservative oxygen therapy group experienced a lower incidence of atelectasis (odds ratio 0.28, 95% CI 0.12–0.66, P = .003) and earlier mechanical ventilator weaning success (adjusted hazard ratio 2.96, 95% CI 1.73–5.05, P < .001). 20,21 However, the ICU-ROX study reported no significant differences in stay between the mechanically ventilated conservative therapy group and the usual oxygen therapy groups.22 The authors reported that using a target oxygen saturation range of 88–92% was feasible for mechanically ventilated cardiac arrest survivors and resulted in more use of spontaneous ventilation mode, more ventilation on room air (
= 90–92%) was feasible and free of adverse outcomes while allowing a marked decrease in excess oxygen exposure. Subjects in this conservative oxygen therapy group experienced a lower incidence of atelectasis (odds ratio 0.28, 95% CI 0.12–0.66, P = .003) and earlier mechanical ventilator weaning success (adjusted hazard ratio 2.96, 95% CI 1.73–5.05, P < .001). 20,21 However, the ICU-ROX study reported no significant differences in stay between the mechanically ventilated conservative therapy group and the usual oxygen therapy groups.22 The authors reported that using a target oxygen saturation range of 88–92% was feasible for mechanically ventilated cardiac arrest survivors and resulted in more use of spontaneous ventilation mode, more ventilation on room air ( = 0.21) and shorter critical care unit stay.22 These studies support the view that conservative oxygen management may improve patient safety and reduce both mortality and duration of ventilation.
= 0.21) and shorter critical care unit stay.22 These studies support the view that conservative oxygen management may improve patient safety and reduce both mortality and duration of ventilation.
Current strategies support timely weaning of oxygen to avoid hyperoxia using pulse oximetry. Despite research stressing the detrimental effects of hyperoxia, excessive use of oxygen continues in critical care units. Metcalf et al11 surveyed the use of protocols and noted that most hospitals used oxygen-weaning protocols. A significant barrier to the implementation of oxygen-titration protocols is a lack of knowledge regarding current literature or guidelines, which leads to disparities between clinical practice and evidenced-based recommendations.23 Respiratory therapists are capable of titrating the  in intubated and mechanically ventilated patients, which can significantly shorten duration of mechanical ventilation and weaning.23
in intubated and mechanically ventilated patients, which can significantly shorten duration of mechanical ventilation and weaning.23
Limitations of this retrospective data analysis include a small convenience sample size, possible selection bias, and short study period (ie, 4 months). A sample population extending the study to surgical, neurological, and cardiovascular ICUs would allow the generalization of the results to a broader group of critical care patients. However, considering the scarce documentation regarding adherence to oxygen protocols, this small sample most likely reflects the current practice because the subject population in the study came from one of the busiest critical care facilities in San Antonio. This study did not follow subjects postextubation to evaluate the short- and long-term effects of excessive hyperoxia. In addition, a larger sample size including nonintubated patients from different critical care areas should be conducted. An important point to consider is that the results assume that respiratory therapists documented all  changes in the electronic medical records in real time. A delay in documenting changes in
changes in the electronic medical records in real time. A delay in documenting changes in  could have changed the results. However, patient assessments are performed and documented every 2 h at the clinical site, thus documentation in the electronic medical records should be a close reflection of real-time changes performed by respiratory therapists.
could have changed the results. However, patient assessments are performed and documented every 2 h at the clinical site, thus documentation in the electronic medical records should be a close reflection of real-time changes performed by respiratory therapists.
Further studies should evaluate the clinical outcomes of patients for whom oxygen therapy was not weaned in a timely manner. This study can be expanded to analyze factors that hinder the clinicians from effectively implementing the protocol and identifying the barriers associated with implementation and adoption.
Conclusions
This retrospective chart review indicates that clinicians in charge of making changes in oxygen concentrations often do not follow the existing oxygen-weaning protocol. This can result in a considerable time lag between meeting the criteria for weaning and actually weaning critical care patients from oxygen. Available published scientific data offer strong evidence that hyperoxia is harmful. The benefits of oxygen therapy should be weighed against potential adverse effects. We recommend that the current protocol be revised to include a multidisciplinary team approach and to establish both a minimum  to initiate weaning and a maximum
to initiate weaning and a maximum  level not to exceed 96%.24 Broader studies are necessary to investigate the factors that influence proper protocol implementation, in addition to the long-term clinical effects of patients who were not weaned from oxygen in accordance with protocol.
level not to exceed 96%.24 Broader studies are necessary to investigate the factors that influence proper protocol implementation, in addition to the long-term clinical effects of patients who were not weaned from oxygen in accordance with protocol.
Footnotes
- Correspondence: Ruben D Restrepo MD RRT FAARC, Division of Respiratory Care, The University of Texas Health Science Center at San Antonio, 7703 Floyd Curl Dr, San Antonio, TX 78229. E-mail: restrepor{at}uthscsa.edu
A version of this paper was presented at the Open Forum at the AARC Congress 2017, held October 4–7, 2017, in Indianapolis.
- Copyright © 2020 by Daedalus Enterprises









{kind=link}
{kind=link}