

Abstract
Respiratory monitoring in patients receiving oxygen therapy for acute care is mandatory at the initial stage of in-hospital management given the potential risk of clinical worsening. Although some patients benefit from close monitoring in the ICU, the vast majority of them are managed in general wards with reduced staff and clinical supervision. The objective of monitoring is to detect early clinical deterioration, which may help prevent in-hospital cardiac arrest. In addition to the clinical and usual evaluations (eg, breathing frequency, breathing pattern, oximetry, and oxygen flow requirements), early warning scoring systems have been developed to detect clinical deterioration in acutely ill patients. The monitoring of these scores is recommended for patients receiving oxygen therapy. These scores have several limitations, among which is the absence of oxygen flow evaluation. Manual and intermittent monitoring of these scores in the ward is time-consuming and may not be sufficient to accurately detect deterioration of patient’s clinical condition in a timely manner. Automated and continuous monitoring, in addition to clinical evaluation and arterial blood gases analysis, which remain necessary, may improve the detection of clinical worsening in specific patients. Devices that automatically titrate and wean oxygen flow on the basis of  enable measurement of several major cardiorespiratory parameters (eg,
enable measurement of several major cardiorespiratory parameters (eg,  , oxygen flow, heart rate, breathing frequency, and heart rate variability). The combination of these parameters into new scores is at least as accurate and well-evaluated, and recommended early warning scores and may be useful in monitoring patients receiving oxygen therapy.
, oxygen flow, heart rate, breathing frequency, and heart rate variability). The combination of these parameters into new scores is at least as accurate and well-evaluated, and recommended early warning scores and may be useful in monitoring patients receiving oxygen therapy.
- acute respiratory failure
- COPD
- oxygen therapy
- respiratory monitoring
- oximetry
- oxygen flow
- breathing frequency
- early warning scores
- automated oxygen therapy
Introduction
In-hospital cardiac arrest remains a frequent event, with almost 300,000 occurring every year among adult patients in the United States.1 This is nearly 10 times higher than the annual motor vehicle fatality rate in United States.2 Cardiac arrest is most frequently due to cardiac causes (50–60%) or respiratory insufficiency (15–40%). Contrary to out-of-hospital cardiac arrests, in-hospital cardiac arrests are considered preventable because hospitalized patients, usually managed during the acute phase of their illness, are closely monitored.3 In most cases, a deterioration of the clinical condition occurs prior to an in-hospital cardiac arrest.4 Prevention is therefore recommended with early identification of at-risk patients combined with early interventions, such as rapid response teams.5 The first step is the identification of clinical condition worsening with the usual monitoring tools (eg, vital signs, biological signs) and with scoring systems based on multiple criteria. Many scoring systems have been developed based on the concept of an early warning scoring (EWS) system, published > 20 years ago.6 These scores, however, are difficult to implement, and results of these scoring systems are not generalizable across heterogeneous hospitals systems.7,8 It is likely that many patients receive oxygen therapy before cardiac arrest, especially if cardiac arrest is related to respiratory insufficiency. Surprisingly, oxygen flow is not part of the EWS systems, even though this is a major parameter used by clinicians to evaluate the severity of a patient’s illness. This discrepancy will be discussed in this review. In patients receiving oxygen therapy, clinical evaluation and close monitoring are essential, including breathing frequency, signs of respiratory distress, and other physiological parameters related to oxygen needs.9 In addition, the close monitoring of physiological parameters is recommended for patients receiving conventional oxygen therapy, and  should be used “in all breathless and acutely ill patients.”10 The British Thoracic Society also recommends the use of a physiological track and trigger system such as the National Early Warning Score (NEWS) to monitor patients receiving oxygen therapy.10,11
should be used “in all breathless and acutely ill patients.”10 The British Thoracic Society also recommends the use of a physiological track and trigger system such as the National Early Warning Score (NEWS) to monitor patients receiving oxygen therapy.10,11
We review several monitoring parameters and scoring systems recommended for patients receiving oxygen therapy and discuss the limitations of current scores. We will then present a new score, the Early Warning ScoreO2, which is dedicated to patients receiving oxygen therapy, and includes the oxygen flow. This score was designed in the context of the development of automated oxygen titration devices.
Usual Monitoring of Patients on Oxygen Therapy
Clinical Evaluation
Clinical evaluation is required to evaluate the severity of illness in patients receiving oxygen therapy, and visually monitoring a patient may provide more information on the patient’s condition than any scores. In addition to the basic vital signs (eg, pulse, breathing frequency, arterial pressure, temperature), the breathing pattern, signs of hemodynamic shock, and encephalopathy must be evaluated in acutely ill patients to detect signs of low peripheral perfusion and signs of respiratory distress (Fig. 1).12 Other essential parameters to evaluate patients receiving oxygen therapy include breathing frequency, oxygenation parameters ( and oxygen supplementation requirements), and arterial blood gases. However, such monitoring, which implies repeated evaluations of several parameters, is time-consuming and not frequently performed due to staff overload, and thus it may not be sufficient to detect a patient’s deterioration, especially in units with reduced monitoring (eg, outside ICUs) where continuous monitoring of clinical and physiological parameters is not feasible.13
and oxygen supplementation requirements), and arterial blood gases. However, such monitoring, which implies repeated evaluations of several parameters, is time-consuming and not frequently performed due to staff overload, and thus it may not be sufficient to detect a patient’s deterioration, especially in units with reduced monitoring (eg, outside ICUs) where continuous monitoring of clinical and physiological parameters is not feasible.13

Usual and advanced monitoring for acutely ill patients receiving oxygen therapy. EWS = Early Warning Scoring.
Breathing Frequency
Clinical events before in-hospital cardiac arrest are typically respiratory events with increased breathing frequency.14 Breathing frequency is among the first vital signs to change in deteriorating patients, and it has been reported to be the best individual predictor of cardiac arrest in general wards.9 However, the usual vital parameters, including  values and breathing frequency, are insufficiently monitored in patients in the general ward before severe outcomes such as cardiac arrest, ICU admission, or unexpected death.3,15 This parameter is well correlated with other signs of respiratory distress.16 The current method to evaluate breathing frequency in spontaneously breathing patients outside ICU is the visual measurement of breathing in a given time. Measurement of breathing frequency is commonly performed by manually counting the chest movements of the individual over a period of 15–60 s.17 This practice is time-consuming and prone to large variation in estimates of breathing frequency. Typically, the number of breaths occurring within 15 s is counted and then multiplied by 4 to give an estimate of breaths/min, which is therefore quantized into units of 4 breaths/min. This cumbersome method has to be repeated by nurses or other clinicians several times a day and is prone to operator variability. In daily practice, this parameter may not be adequately recorded.18
values and breathing frequency, are insufficiently monitored in patients in the general ward before severe outcomes such as cardiac arrest, ICU admission, or unexpected death.3,15 This parameter is well correlated with other signs of respiratory distress.16 The current method to evaluate breathing frequency in spontaneously breathing patients outside ICU is the visual measurement of breathing in a given time. Measurement of breathing frequency is commonly performed by manually counting the chest movements of the individual over a period of 15–60 s.17 This practice is time-consuming and prone to large variation in estimates of breathing frequency. Typically, the number of breaths occurring within 15 s is counted and then multiplied by 4 to give an estimate of breaths/min, which is therefore quantized into units of 4 breaths/min. This cumbersome method has to be repeated by nurses or other clinicians several times a day and is prone to operator variability. In daily practice, this parameter may not be adequately recorded.18
Recently, L’Her et al19 demonstrated that breathing frequency could be obtained from photoplethysmography tracings. The breathing frequency derived from pulse oximetry signals correlated very well with breathing frequency measured manually, even in subjects with atrial fibrillation.19 This function has been incorporated into some automated oxygen titration and weaning systems, enabling the continuous measurement of breathing frequency in patients wearing a pulse oximetry device.19
Pulse Oximetry
Pulse oximetry is usually considered accurate to evaluate and monitor blood oxygenation20 and is considered the fifth vital sign.10,20 Differences may exist between oximetry devices, although it is usually considered that several oximeters from different leading companies are equivalent in terms of accuracy for  values > 80% when tested in optimal conditions with healthy subjects.21-23 However, differences between oximeters tend to be more pronounced when the comparisons are conducted in patients.24-27
values > 80% when tested in optimal conditions with healthy subjects.21-23 However, differences between oximeters tend to be more pronounced when the comparisons are conducted in patients.24-27
Oximetry measurements have well-known limitations, such as dyshemoglobinemia, polished fingernails, darkly pigmented skin, low perfusion, and motion artefact.20,28 Oximetry inaccuracies are frequently reported in the case of low  (ie, < 80%) and in the case of darkly pigmented skin.21,22 However, several technical improvements have increased the accuracy of the signal in difficult situations. Jubran and Tobin29 reported in 1990 that
(ie, < 80%) and in the case of darkly pigmented skin.21,22 However, several technical improvements have increased the accuracy of the signal in difficult situations. Jubran and Tobin29 reported in 1990 that  > 95% was required to obtain sufficient oxygenation in populations with darkly pigmented skin. Currently, the differences among oximetry devices are negligible for usual levels of
> 95% was required to obtain sufficient oxygenation in populations with darkly pigmented skin. Currently, the differences among oximetry devices are negligible for usual levels of  . During severe hypoxemia, however, a gap of a few mm Hg still exists between
. During severe hypoxemia, however, a gap of a few mm Hg still exists between  and
and  . In several studies by one group, oximeters overestimated
. In several studies by one group, oximeters overestimated  by 2.5–5 mm Hg in comparison with
by 2.5–5 mm Hg in comparison with  in subjects with darkly pigmented skin, especially at very low values (ie, < 70%) and with large standard deviations.21,22,24 Among well-recognized pulse oximeters (eg, Masimo, Nonin, and Nellcor), the bias with reference values (ie,
in subjects with darkly pigmented skin, especially at very low values (ie, < 70%) and with large standard deviations.21,22,24 Among well-recognized pulse oximeters (eg, Masimo, Nonin, and Nellcor), the bias with reference values (ie,  ) were low whatever the color skin when
) were low whatever the color skin when  or
or  values were > 80%.22 In the same study, bias of ± 4% still existed with very low
values were > 80%.22 In the same study, bias of ± 4% still existed with very low  values (ie, 60–70%), and differences up to 10% could be detected in
values (ie, 60–70%), and differences up to 10% could be detected in  values among the tested devices during severe hypoxemia, especially when disposable sensors were used.22 Yamamoto et al30 reported that polished fingernails had only minor impact on
values among the tested devices during severe hypoxemia, especially when disposable sensors were used.22 Yamamoto et al30 reported that polished fingernails had only minor impact on  measurements. In another study conducted in 33 healthy women, several polish colors were tested and the authors noted moderately reduced
measurements. In another study conducted in 33 healthy women, several polish colors were tested and the authors noted moderately reduced  values with specific colors (ie, blue, beige, purple, and white), but the tested oximeters were not among the reference oximeters.31
values with specific colors (ie, blue, beige, purple, and white), but the tested oximeters were not among the reference oximeters.31
Monitoring of pulse oximetry alone did not demonstrate an impact on patient outcomes.32 This may be explained by liberal oxygen administration, which is largely used to avoid hypoxemia. In addition, in a health care system with few hypoxemia events,  is not a good marker of severity, and the level of oxygen flow should instead be used to evaluate respiratory severity. Interestingly, intermittent pulse oximetry monitoring has been reported to be inaccurate to detect episodes of hypoxemia after general surgery.33 In > 800 subjects after noncardiac surgeries, continuous
is not a good marker of severity, and the level of oxygen flow should instead be used to evaluate respiratory severity. Interestingly, intermittent pulse oximetry monitoring has been reported to be inaccurate to detect episodes of hypoxemia after general surgery.33 In > 800 subjects after noncardiac surgeries, continuous  monitoring was performed with blinded results for clinicians. Hypoxemia was frequent, but 90% of the episodes were missed by nurses with intermittent
monitoring was performed with blinded results for clinicians. Hypoxemia was frequent, but 90% of the episodes were missed by nurses with intermittent  measurements.33
measurements.33
Oxygen Requirements ( or Oxygen Flow)
or Oxygen Flow)

How many times have we explained to students that  or
or  provided alone, without mentioning the oxygen requirements (in L/min or as
provided alone, without mentioning the oxygen requirements (in L/min or as  ) is useless to assess a patient’s illness severity? For patients receiving mechanical ventilation, ARDS severity is categorized based on
) is useless to assess a patient’s illness severity? For patients receiving mechanical ventilation, ARDS severity is categorized based on  /
/ 34 or
34 or  /
/ .35 In nonintubated patients,
.35 In nonintubated patients,  or
or  should be interpreted while considering
should be interpreted while considering  (or estimated
(or estimated  36) to evaluate a patient’s illness severity. Surprisingly, there is no EWS that incorporates oxygen flow or
36) to evaluate a patient’s illness severity. Surprisingly, there is no EWS that incorporates oxygen flow or  , although many incorporate
, although many incorporate  .37 Some EWS systems incorporate oxygen requirements, but only in a binary fashion that evaluates if oxygen supplementation is used.37 To our knowledge, only one score derived from NEWS incorporated a semiquantitative evaluation of oxygen flow, even though a patient with an oxygen flow of 2 L/min or 10 L/min (equivalent to 0.30 or 0.60
.37 Some EWS systems incorporate oxygen requirements, but only in a binary fashion that evaluates if oxygen supplementation is used.37 To our knowledge, only one score derived from NEWS incorporated a semiquantitative evaluation of oxygen flow, even though a patient with an oxygen flow of 2 L/min or 10 L/min (equivalent to 0.30 or 0.60  36) are not equivalent!38
36) are not equivalent!38
In comparison with several preexisting models (ie, EWS, Modified EWS [MEWS], and VitalPac EWS [ViEWS]), the  /
/ ratio showed comparable or better predictive accuracy for unexpected ICU transfers in the respiratory wards and for mortality prediction.39 The
ratio showed comparable or better predictive accuracy for unexpected ICU transfers in the respiratory wards and for mortality prediction.39 The  , in addition to breathing frequency and
, in addition to breathing frequency and  , was also used to predict outcome with high-flow nasal cannula therapy.40
, was also used to predict outcome with high-flow nasal cannula therapy.40
With automated oxygen titration devices, the oxygenation parameters ( and oxygen flow or corresponding equivalent
and oxygen flow or corresponding equivalent  ) and respiratory parameters are continuously monitored, and respiratory scores that include these parameters and trends may be helpful in monitoring patients receiving oxygen therapy (see below).
) and respiratory parameters are continuously monitored, and respiratory scores that include these parameters and trends may be helpful in monitoring patients receiving oxygen therapy (see below).
Minute Ventilation
Minute ventilation is a relevant and desirable parameter of monitoring for patients with respiratory failure or for patients receiving sedation.41 In patients who are not on invasive or noninvasive mechanical ventilation, however, this parameter may be difficult to accurately measure in daily practice. Respiratory inductive plethysmography has been used for research purposes to measure tidal volume, breathing frequency, but it requires multiple calibrations and is not adapted for typical care.42 A bio-impedance respiratory volume monitor (ExSpiron, Respiratory Motion, Waltham, Massachusetts) has been proposed and tested during procedural sedations, and it has produced interesting results in detecting apnea or hypoventilation in postoperative care.43-45 However, this monitoring is not recommended in the daily practice for patients receiving oxygen therapy for respiratory failure.10
Arterial Blood Gas Analysis
In patients with potential increased  (ie, patients with suspected or known CO2 retention and especially in the case of loss of consciousness) and in patients with suspected metabolic disorders (eg, renal insufficiency, shock states, or specific intoxications), arterial blood gas analysis with lactate dosage may be required at the initiation of management and then as needed based on the patient’s clinical evolution.10 Arterial blood gas analysis is mainly used to measure pH,
(ie, patients with suspected or known CO2 retention and especially in the case of loss of consciousness) and in patients with suspected metabolic disorders (eg, renal insufficiency, shock states, or specific intoxications), arterial blood gas analysis with lactate dosage may be required at the initiation of management and then as needed based on the patient’s clinical evolution.10 Arterial blood gas analysis is mainly used to measure pH,  , and bicarbonates.
, and bicarbonates.  values are not required when
values are not required when  can be measured, especially if oxygenation recommendations are followed (ie, if
can be measured, especially if oxygenation recommendations are followed (ie, if  is maintained at 88–92% or 90–94%). The prescription of long-term oxygen therapy may be an exception, and
is maintained at 88–92% or 90–94%). The prescription of long-term oxygen therapy may be an exception, and  may be then required to decide on the initiation of this treatment.46 In other situations, capillary blood gas analysis may be sufficient for the clinician’s decision-making and preferred for the patient’s comfort.47 A meta-analysis of the studies comparing arterial and capillary blood gas measurements, pH,
may be then required to decide on the initiation of this treatment.46 In other situations, capillary blood gas analysis may be sufficient for the clinician’s decision-making and preferred for the patient’s comfort.47 A meta-analysis of the studies comparing arterial and capillary blood gas measurements, pH,  , and bicarbonates values were well correlated.48 Several noninvasive measurements of CO2 may be alternatives to arterial blood gas analysis for CO2 monitoring, such as capnography (end-tidal CO2 measurements) and transcutaneous CO2 measurements. In mechanically ventilated patients, capnography has been evaluated extensively, although in extubated patients the data are not convincing during procedural sedations or in patients with respiratory failure.49,50 Similarly, transcutaneous arterial CO2 measurements have shown mixed results and cannot replace arterial blood gas analysis.51-54
, and bicarbonates values were well correlated.48 Several noninvasive measurements of CO2 may be alternatives to arterial blood gas analysis for CO2 monitoring, such as capnography (end-tidal CO2 measurements) and transcutaneous CO2 measurements. In mechanically ventilated patients, capnography has been evaluated extensively, although in extubated patients the data are not convincing during procedural sedations or in patients with respiratory failure.49,50 Similarly, transcutaneous arterial CO2 measurements have shown mixed results and cannot replace arterial blood gas analysis.51-54
Advanced Monitoring for Patients on Oxygen Therapy
Early Warning Scores
The concept of the EWS was developed over; 20 years ago.6 The scoring system has been developed for the early recognition of patients at risk for clinical deterioration.55 In-hospital patients managed for acute respiratory failure are frequently on oxygen therapy, and many are at risk of early deterioration. Data indicate that 10–20% of the patients managed for community-acquired pneumonia requiring hospitalization will be transferred to an ICU,56,57 and the same proportion require ICU admission within 72 h. Carr et al58 evaluated a registry of cardiopulmonary arrest events that occurred within 72 h of hospital admission; 12% occurred in patients with preexisting pneumonia, and among those patients with pneumonia, almost 40% of cardiac arrests occurred outside the ICU setting.58 Viral pneumonia may have an even worse outcome,59 and approximately 30% of patients managed for COVID-19 required management in the ICU.60,61
Many scores have been developed to monitor in-hospital patients: EWS, MEWS, NEWS, ViEWS, Abreviated VitalPac (AbEWS), NEWS2, Hamilton EWS (HEWS), Nottingham University EWS (NUH-EWS), Chronic Respiratory EWS (CREWS), NEWS-Lactate, Cardiac Arrest Risk Triage (CART), among others.62-68 There are > 100 different published track-and-trigger systems, most of which have been modified from the original EWS and developed using expert opinion, which has demonstrated variable levels of reliability, validity, and usefulness.69,70 Meta-analyses have been conducted to evaluate the impact of the implementation of these scores on outcomes55 NEWS, which combines physiological parameters such as breathing frequency,  , delivery of oxygen (or not), pulse rate, systolic blood pressure, level of consciousness, and temperature, may be beneficial for predicting patient deterioration.65 However, a general conclusion cannot be generated due to heterogeneity in the way the score is used in studies and in populations studied.7 Monitoring any EWS is recommended in hospitalized patients, especially when receiving oxygen.10,11 When compared to the Quick Sepsis-Related Organ Failure Assessment (qSOFA) and systemic inflammatory response syndrome (SIRS), NEWS was found to be the most accurate for the detection of all sepsis end points.71,72 The introduction of the NEWS score did not change patient outcomes in several recent evaluations, although the NEWS score can predict outcome and determine the patient’s illness severity when evaluated at the emergency department and after admission.73-75 One of several issues regarding these scoring systems is that the recording of all parameters is time-consuming and frequently incomplete.15 In addition, these scores provide only an intermittent view of a patient’s condition, and deterioration between 2 evaluations may be missed.76
, delivery of oxygen (or not), pulse rate, systolic blood pressure, level of consciousness, and temperature, may be beneficial for predicting patient deterioration.65 However, a general conclusion cannot be generated due to heterogeneity in the way the score is used in studies and in populations studied.7 Monitoring any EWS is recommended in hospitalized patients, especially when receiving oxygen.10,11 When compared to the Quick Sepsis-Related Organ Failure Assessment (qSOFA) and systemic inflammatory response syndrome (SIRS), NEWS was found to be the most accurate for the detection of all sepsis end points.71,72 The introduction of the NEWS score did not change patient outcomes in several recent evaluations, although the NEWS score can predict outcome and determine the patient’s illness severity when evaluated at the emergency department and after admission.73-75 One of several issues regarding these scoring systems is that the recording of all parameters is time-consuming and frequently incomplete.15 In addition, these scores provide only an intermittent view of a patient’s condition, and deterioration between 2 evaluations may be missed.76
Results of a study by Hodgson et al77 suggested that NEWS was less discriminative in predicting deterioration in subjects with respiratory disease compared to a population of unselected medical admissions. The NEWS2 score has been developed to take into account different  targets in patients with COPD, but there is a debate on the utility of this new score in clinical practice.78-80
targets in patients with COPD, but there is a debate on the utility of this new score in clinical practice.78-80
New Automated and Continuous Scoring Systems Derived From Wearable Sensors
New technologies have been developed to allow continuous monitoring in the medical setting with the aim to detect clinical deterioration earlier, to reduce work load, and to improve patient comfort (Fig. 2).81-85 Several wireless and wearable sensors that allow continuous measurement of new scoring systems related to EWS have been evaluated in several studies, showing good accuracy and promising results for patient monitoring.76,86,87 In these studies, automated breathing frequency measurement was considered more accurate than measurements made by nurses. In addition, the detection of hypoxemia was more accurate with continuous measurements of  than with intermittent measurements.33
than with intermittent measurements.33

Advanced monitoring with manual and automated recording of Early Warning Scoring (EWS) systems. MEWS = modified EWS; NEWS = National EWS, ViEWS = VitalPac EWS; AbEWS = abbreviated VitalPac; NEWS2 = National EWS 2; NEWS-L = NEWS-lactate; CART = Cardiace Arrest Risk Triage.
New Automated and Continuous Scoring Systems Derived From Automated Oxygen Titration
In patients receiving high-flow nasal cannula oxygen therapy, the ratio of pulse oximetry/ ), defined as the ratio of
), defined as the ratio of  /
/ to breathing frequency (breaths/min), predicted the need for invasive mechanical ventilation.40,88 This index cannot be transposed to conventional oxygen therapy, given the impact of nasal high-flow cannula therapy on breathing frequency.89,90 With automated oxygen titration (eg, with the FreeO2 device, OxyNov, Quebec, Canada), which requires continuous pulse oximetry measurement, it is possible to continuously obtain several physiological values such as
to breathing frequency (breaths/min), predicted the need for invasive mechanical ventilation.40,88 This index cannot be transposed to conventional oxygen therapy, given the impact of nasal high-flow cannula therapy on breathing frequency.89,90 With automated oxygen titration (eg, with the FreeO2 device, OxyNov, Quebec, Canada), which requires continuous pulse oximetry measurement, it is possible to continuously obtain several physiological values such as  , oxygen flow, breathing frequency, heart rate, and heart rate variability. Indeed, in addition to the oxygen flow, which varies based on the patient’s requirements to attain the
, oxygen flow, breathing frequency, heart rate, and heart rate variability. Indeed, in addition to the oxygen flow, which varies based on the patient’s requirements to attain the  target, it is possible to obtain several important physiological parameters derived from the oximetry measurement.91
target, it is possible to obtain several important physiological parameters derived from the oximetry measurement.91  and pulse rate are the main parameters obtained with pulse oximeters. Breathing frequency can be continuously measured with a specific algorithm based on photoplethysmographic signal analysis.19 Heart rate variability can also be measured with the photoplethysmographic signal analysis.19 With automated oxygen titration, it is possible to combine these measured parameters in a new EWS that is focused on patients on oxygen therapy (Early Warning ScoreO2) (Fig. 3, Fig. 4). The Early Warning ScoreO2, with several combinations of cardiorespiratory parameters provided by the automated oxygen titration device, was at least as accurate as several well-validated scores (eg, NEWS, NEWS2,
and pulse rate are the main parameters obtained with pulse oximeters. Breathing frequency can be continuously measured with a specific algorithm based on photoplethysmographic signal analysis.19 Heart rate variability can also be measured with the photoplethysmographic signal analysis.19 With automated oxygen titration, it is possible to combine these measured parameters in a new EWS that is focused on patients on oxygen therapy (Early Warning ScoreO2) (Fig. 3, Fig. 4). The Early Warning ScoreO2, with several combinations of cardiorespiratory parameters provided by the automated oxygen titration device, was at least as accurate as several well-validated scores (eg, NEWS, NEWS2,  /
/ ) in 1,729 subjects in the emergency department setting and in 102 subjects in the ICU setting.92,93 Additional evaluations of these new scores are required to confirm the initial promising results. These automated and continuously measured scores may be useful for monitoring patients with acute respiratory failure on oxygen therapy, especially in the general ward. With the recent COVID-19 outbreak61 and other transmissible respiratory viruses (Middle East respiratory syndrome [MERS]94, severe acute respiratory syndrome [SARS]95), the need to reduce the interventions from health care workers at the patient’s bedside to limit contaminations is an important goal. It may be achieved by automating the delivery and the monitoring of oxygen therapy, whereas almost all patients receive oxygen therapy when they require hospitalization.61
) in 1,729 subjects in the emergency department setting and in 102 subjects in the ICU setting.92,93 Additional evaluations of these new scores are required to confirm the initial promising results. These automated and continuously measured scores may be useful for monitoring patients with acute respiratory failure on oxygen therapy, especially in the general ward. With the recent COVID-19 outbreak61 and other transmissible respiratory viruses (Middle East respiratory syndrome [MERS]94, severe acute respiratory syndrome [SARS]95), the need to reduce the interventions from health care workers at the patient’s bedside to limit contaminations is an important goal. It may be achieved by automating the delivery and the monitoring of oxygen therapy, whereas almost all patients receive oxygen therapy when they require hospitalization.61
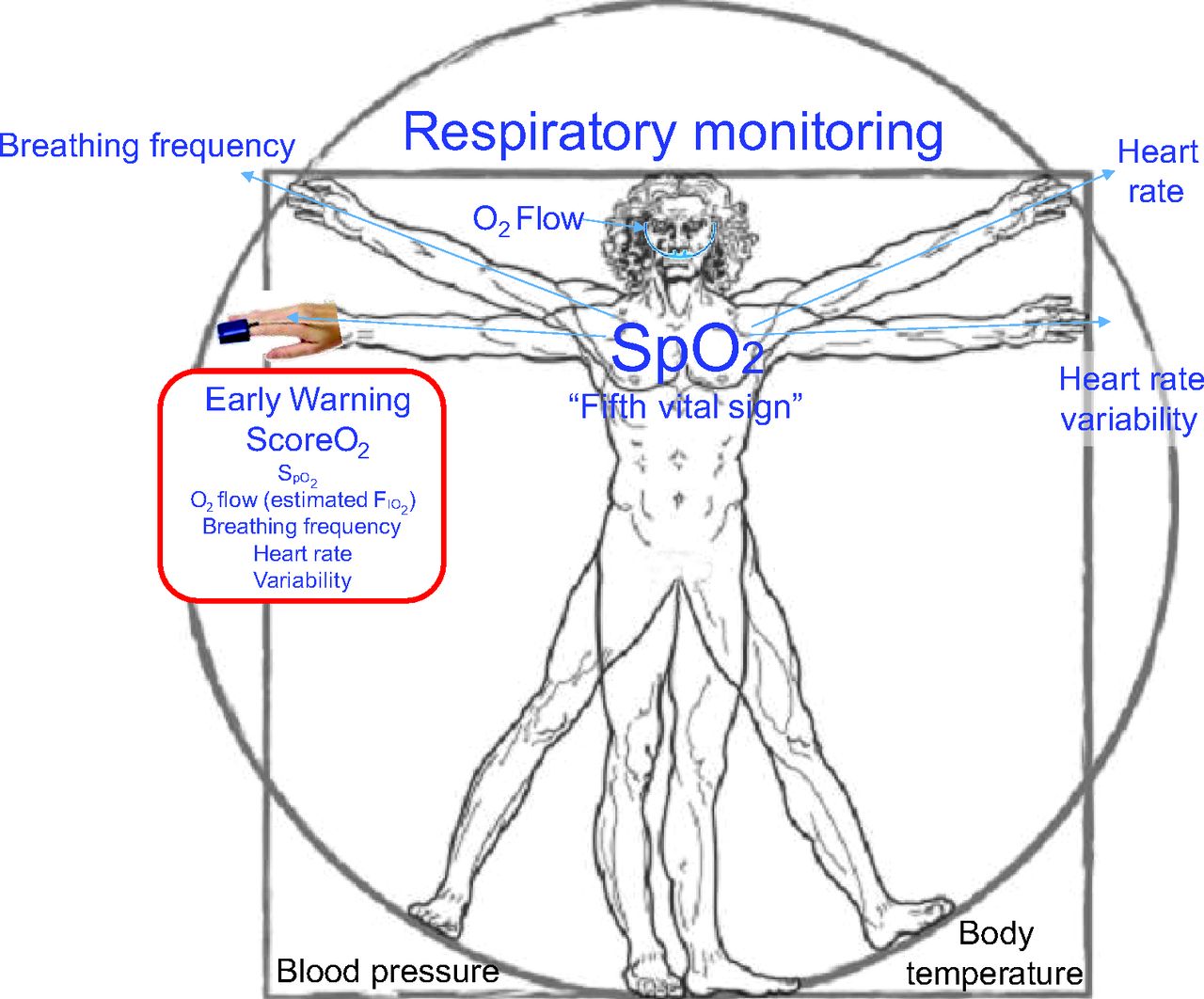
Early Warning ScoreO2 was developed from physiological parameters measured with the automated oxygen-titration device FreeO2. O2 flow (and estimated  ),
),  , breathing frequency, and heart rate have been combined in this score. Variability is another parameter derived from photoplethysmography that can be used in the score.
, breathing frequency, and heart rate have been combined in this score. Variability is another parameter derived from photoplethysmography that can be used in the score.

Examples of variations of the Early Warning ScoreO2 (ScoreO2) during 48 h in 2 patients with COPD. A: One patient had a favorable clinical evolution; (B) the other patient had a poor clinical evolution. In both patients, the automated oxygen-titration device (FreeO2) was set with a target  of 90%. The patient with a favorable outcome had an initial breathing frequency of 35 breaths/min, received oxygen flow of 1.0 L/min, and had an Early Warning ScoreO2 of 6.7. After 2 d, breathing frequency and oxygen flow decreased, and the resulting ScoreO2 was 5.0. The patient with the poor outcome (ie, ICU admission and intubation) had an initial ScoreO2 of 7.7 with a progressive increase to 20.4.
of 90%. The patient with a favorable outcome had an initial breathing frequency of 35 breaths/min, received oxygen flow of 1.0 L/min, and had an Early Warning ScoreO2 of 6.7. After 2 d, breathing frequency and oxygen flow decreased, and the resulting ScoreO2 was 5.0. The patient with the poor outcome (ie, ICU admission and intubation) had an initial ScoreO2 of 7.7 with a progressive increase to 20.4.
Summary
Respiratory monitoring is essential in patients receiving oxygen therapy for acute care, especially during the first days after treatment initiation. A patient’s clinical condition may rapidly improve, which should lead to a reduction of support, including oxygen therapy, and to the early detection of criteria for hospital discharge. A patient’s clinical condition may also worsen rapidly to the point that more intensive monitoring, additional support, and potentially a reevaluation of treatment may be needed. Usual monitoring includes clinical oxygenation parameters and, for specific patients, arterial blood gas analysis. Advanced monitoring includes the utilization of EWS systems. The aim of EWS systems is to detect clinical worsening early. However, EWS systems have several limitations, including the lack of evaluation of oxygen requirements and manual and intermittent recording. Intermittent monitoring is a time-consuming and labor-intensive process, and it may miss changes in a patient’s clinical condition. This approach may not be optimal for the dynamic management of patients in a health care system under pressure with an increased number of fragile patients and a limited number of ICU beds. Automated and continuous monitoring may optimize patient care by improving the early detection of clinical deterioration while reducing the work load related to monitoring. Physiological parameters, including oxygen requirements, measured by devices that automatically deliver oxygen based on the  have been combined. In initial evaluations, the new scores that stem from these simple parameters provide information that is at least as accurate as other EWS systems in detecting early deterioration of clinical conditions. These new scores may improve the monitoring of patients receiving oxygen therapy, but additional research is required to evaluate the impact on patient outcomes.
have been combined. In initial evaluations, the new scores that stem from these simple parameters provide information that is at least as accurate as other EWS systems in detecting early deterioration of clinical conditions. These new scores may improve the monitoring of patients receiving oxygen therapy, but additional research is required to evaluate the impact on patient outcomes.
Footnotes
- Correspondence: François Lellouche MD PhD, Centre de Recherche de l’Institut Universitaire de Cardiologie et de Pneumologie de Québec, 2725 Chemin Sainte-Foy, G1V4G5, Québec, QC, Canada. E-mail: francois.lellouche{at}criucpq.ulaval.ca
Drs Lellouche and L’Her are co-founders, shareholders, and directors of Oxynov, a research and development company that designed and marketed the automated oxygen adjustment system (FreeO2) used in this work.
- Copyright © 2020 by Daedalus Enterprises
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.
- 26.
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.
- 53.
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.
- 64.
- 65.↵
- 66.
- 67.
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.
- 80.↵
- 81.↵
- 82.
- 83.
- 84.
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵









{kind=link}
{kind=link}
{kind=link}
{kind=link}