

Abstract
BACKGROUND: Signs and symptoms of asthma are well established; however, no study has been performed to rank them. Therefore, we performed this systematic review and meta-analysis to determine the pooled frequencies of different signs and symptoms of asthma in subjects age ≥ 14 y to develop a patient-specific questionnaire.
METHODS: Specific search queries were developed to include records published in Embase, PubMed, Cochrane Library, and Google Scholar, until November 2016. We planned to include randomized controlled trials (RCTs) and observational studies for determining the pooled proportions of signs and symptoms and association between combination of symptoms and asthma severity in subjects age ≥ 14 y. The quality assessment was performed using 3 parameters: reported number or percentage of subjects with asthma symptoms, respiratory disorder history, and method for data collection.
RESULTS: Of the 4,939 records retrieved, 67 observational studies (N = 57,033 subjects; age ≥ 14 y) were considered eligible for inclusion in the analysis. A total of 10 symptoms were reported across the studies, with pooled proportions of nasal congestion, sleep disturbances, breathlessness, chest tightness, and wheezing being 61.57%, 56.56%, 50.31%, 50.41%, and 46.97%, respectively. In records of medical history, the pooled proportion of rhinitis was 76.37%, followed by allergy/atopy at 63.53%. The pooled proportion of asthma medication use was 83.27%. In terms of the symptom combinations, the combination of wheezing, breathlessness, chest tightness, and cough was reported in 71.26% of subjects from 4 studies (n = 12,014 subjects). Nasal congestion, sleep disturbance, and chest tightness were the most common symptoms of asthma, followed by wheezing and breathlessness with a combination of symptoms (ie, wheezing, breathlessness, chest tightness, and cough) affecting the highest proportion of subjects.
CONCLUSIONS: Asthma severity was dependent on variety of symptoms, consisting mostly of wheezing, breathlessness, chest tightness, and cough. On the basis of our analysis, we recommend a combination of symptoms be included in diagnostic-based questionnaires to aid early diagnosis.
Introduction
Asthma is a chronic inflammatory airway disease that is characterized by airway obstruction and bronchial hyper-responsiveness.1 According to the 2018 Global Asthma Report (http://www.globalasthmareport.org/Global%20Asthma%20Report%202018.pdf, Accessed December 12, 2018), nearly 339 million people are affected by asthma worldwide, and the 2016 Global Burden of Disease collaboration reported 420,000 asthma-related deaths per year.
According to the previous Global Asthma Report, published in 2014 (http://www.globalasthmareport.org/2014/resources/Global_Asthma_Report_2014.pdf, Accessed April 14, 2017), the total global asthma population is expected to exceed 400 million by 2025. The burden of asthma by age as estimated by disability-adjusted life years has shown a peak distribution between the ages of 10–14 y and 75–79 y and the lowest disease burden was at an age of 30–34 y.
In China, although a high prevalence of asthma is reported in children < 14 y old, only 67% of children have physician-diagnosed asthma.2 Further, there is a huge economic burden associated with asthma in developing countries,2 which tends to increase with a greater severity and inadequate control of the disease.3 The evolution of asthma pathophysiology, treatments, treatment recommendations, and the adoption of a patient-centered approach makes possible early diagnosis for effective asthma management.4–6 Therefore, early identification of asthma symptoms is key to early asthma diagnosis, its control, and saving the patient (and society) from high treatment costs.
However, despite asthma management guidelines focusing on improving asthma diagnosis, multiple studies have reported misdiagnosis or overdiagnosis of asthma.7–9 Asthma is overdiagnosed in developed countries, and obesity is one of the potential causes of overdiagnosis. In obesity, there is reduced chest wall compliance, thereby leading to reduced lung volumes and increased breathlessness, and thus patients with obesity are more likely to be misdiagnosed as having asthma.8 Misdiagnosis is the major reason for undertreatment or unwanted treatment of asthma symptoms, which may result in aggravation of symptoms or unwanted exposure to drugs, respectively, and may lead to adverse consequences.10–13 Therefore, this systematic review and meta-analysis was performed to collect the reported signs and symptoms and clinical/medical history of subjects with asthma, and to collate related frequencies to quantify the most frequent parameters in a large patient population. We believe that the quantification of the signs and symptoms and clinical/medical history of asthma will help health care practitioners better diagnose asthma and provide optimized treatment.
Methods
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and is registered in PROSPERO (CRD42016054026).
Funding
The study was funded by AstraZeneca China. The funding body approved the study design, data collection, data analysis, data interpretation, and writing of the manuscript. The writing committee had full access to all data and had the final responsibility for the decision to submit the manuscript for publication.
Search Strategy
We performed a search of published clinical literature in English-language biomedical literature databases including PubMed, Google Scholar, Cochrane, and Embase using specific search strings: (asthma OR ‘asthma’ OR ‘asthma, bronchial’) AND (predictive OR prediction) AND ([symptoms] OR [medical history OR comorbidity] OR [diagnosis OR diagnoses]). Articles from database inception to November 2016 were searched without any other date restriction. See the supplementary materials at http://www.rcjournal.com for a detailed search strategy.
Study Selection and Quality Assessment
We planned to include all original research articles (retrospective or prospective), surveys, observational studies, case-control studies, cohort studies, and randomized controlled trials (RCTs) that reported, determined, or discussed the frequency of asthma symptoms along with the medical history and comorbidities at the time of enrollment in the study. The studies were considered relevant for inclusion if they had enrolled asthma subjects age ≥ 14 y, were published in English, and described the signs and clinical history of asthma at baseline. The initial screening included selection of articles based on the title and abstract, which was followed by another step of evaluation using the full text. Studies were excluded if they had designs other than those mentioned in the inclusion criteria (eg, case reports, preclinical evaluations, pharmacokinetic studies, systematic reviews, and meta-analyses) or did not include adequate presentation or discussion of the clinical symptoms of asthma.
Prior to screening, all duplicate records were deleted. The remaining articles were screened independently by 2 researchers (JF and JX), with one of the reviewers being a senior academic. Completely nonrelevant articles were excluded by evaluating the titles and abstracts. The 2 reviewers assessed the eligibility of the remaining articles using full text. Any disagreement regarding the inclusion of any study was resolved after discussion or intervention by a third reviewer (QM) if consensus was not reached after discussion.
Eligible studies were subjected to quality assessment to avoid any potential publication bias. Due to inclusion of multiple study types, we planned to perform the quality assessment using the Cochrane risk bias tool for RCTs (http://handbook.cochrane.org/chapter_8/table_8_5_a_the_cochrane_collaborations_tool_for_assessing.htm, Accessed April 14, 2017), and checklists or scales for non-randomized/observational studies developed by the Newcastle-Ottawa Scale (http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp, Accessed April 14, 2017), the Meta-Analysis of Observational Studies in Epidemiology,14 and Strengthening the Reporting of Observational Studies in Epidemiology.15 For observational studies, the quality of articles was assessed based on 3 parameters: (i) reported number/percentage of subjects with asthma symptoms; (ii) respiratory disorder history; and (iii) standardized method for data collection (eg, standardized case report form/questionnaire/medical records). The quality of observational studies was considered acceptable when 2 of the 3 aforementioned criteria were met. The reasons for exclusion of articles are listed in Figure 1.

Flow chart.
Data Extraction
Extracted data were entered in a spreadsheet template and categorized as baseline information (eg, study duration, study design, recruitment methods, sample size), symptoms, clinical history, asthma severity, and drug utilization history. Any data not reported in the paper were considered as missing.
Statistical Analysis
We computed descriptive statistics for the baseline variables. All continuous variables were presented with means with standard deviations (SD) or medians with interquartile ranges (IQR) as appropriate. All categorical variables were presented as percentages or frequencies. Simple frequency (%) and 95% CIs of different symptoms and clinical or medical history in the individual studies were determined and pooled to give a pooled proportion with a 95% CI. The pooled proportion for a combination of symptoms and the association between combinations and asthma severity were determined using relative risk and 95% CI. Statistical heterogeneity was determined using I2 statistics and was important when I2 exceeded 50%. Therefore, depending on the heterogeneity among the included studies, a fixed-effects model (I2 < 50%) or a random-effects model (I2 > 50%) was used to evaluate the outcomes. All the statistical analyses were performed with R 3.3.2 (http://personality-project.org/r/book/R.short.course.pdf, Accessed April 14, 2017). No subgroup/sensitivity analysis was performed despite the inclusion of heterogeneous study types because the baseline data collected for analysis would not be influenced by study design.
Results
Search Results and Study Characteristics
A total of 4,939 studies were retrieved after thorough manual and electronic searches in all the databases and removing the duplicates. Two independent reviewers checked the abstracts for relevancy, resulting in 134 articles selected for full-text evaluation. Of these 134 articles, 67 were included and analyzed in our meta-analysis based on our inclusion and exclusion criteria. The reasons for exclusion of 67 articles are presented along with a detailed study flow in Figure 1. The included 67 studies (63 prospective observational studies, 4 retrospective studies) enrolled 57,033 subjects age ≥ 14 y with asthma symptoms.16–82 The characteristics of included studies are presented in Table 1.
Characteristics of Included Studies
Pooled Frequencies
Signs and Symptoms
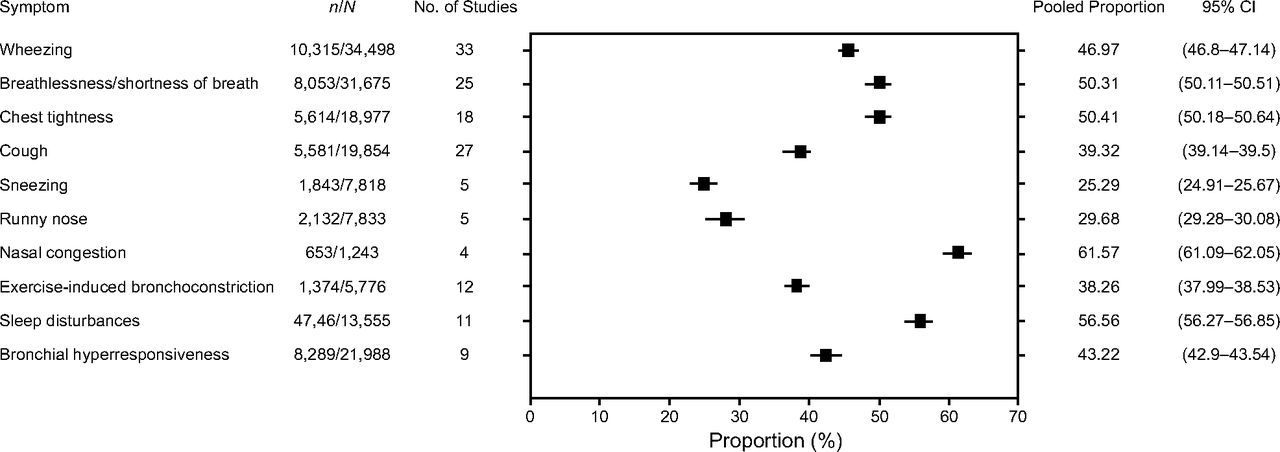
Overall, 9 major signs and symptoms were reported in the included 67 studies, with each study reporting ≥ 1 symptom; a total of 7 symptoms was the maximum in any one study (Fig. 2). Figure 2 does not present whether symptoms were reported during the day or the night. Heterogeneity among the studies included for evaluating individual parameters was high (I2 = 95–99%), so the meta-analysis for all the individual parameters was performed using a random-effects model.

Frequency of all signs and symptoms.
Pooled proportions of the signs and symptoms exceeding 40% included nasal congestion (61.57% [95% CI 61.09–62.09] in 4 studies), sleep disturbance (56.56% [95% CI 56.27–56.85] in 11 studies), chest tightness (50.41% [95% CI 50.18–50.64] in 18 studies), breathlessness (50.31% [95% CI 50.11–50.51] in 25 studies), wheezing (46.97% [95% CI 46.80–47.14] in 33 studies), and bronchial hyper-responsiveness (43.22% [95% CI 42.90–43.54] in 9 studies) (Fig. 2). Symptoms were also categorized by time of occurrence, with a pooled frequency of 38.8% for daytime (7 studies) and 32.3% at night (11 studies). The signs and symptoms with the 5 greatest pooled frequencies are listed in Table 2.
Five Most Frequent Signs and Symptoms
Medical and Drug Utilization History
Figure 3 presents the pooled proportions of clinical or medical history parameters reported in the studies. Similar to signs and symptoms, the proportion of subjects with a specific history were recorded, and pooled proportions were calculated by means of a random-effects model (I2 = 98.80–99.80%). The most prevalent clinical history parameters reported were rhinitis (76.37% [95% CI 76.17–76.57]) in 18 studies, allergy/atopy (63.53% [95% CI 63.37–63.39]) in 33 studies, hospitalization due to asthma (57.87% [57.65–58.13]) in 16 studies, and sinusitis (51.10% [50.61–51.59]) in 4 studies. Other relevant medical histories included smoking, family history, and preexisting respiratory indications.

Medical history.
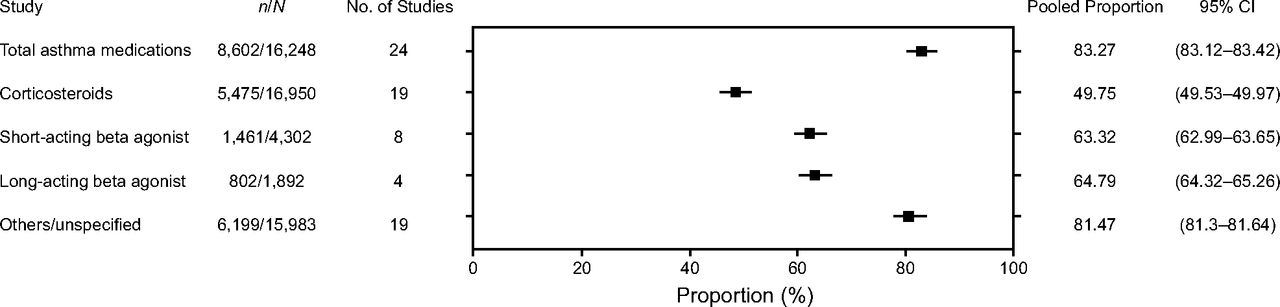
Figure 4 presents the utilization of anti-asthma drugs administered in the included study population. Overall, 83.27% (95% CI 83.12–83.42) of subjects had a history of taking asthma medications (24 studies; however, no segregation was reported). Further, the combined utilization of inhaled and oral corticosteroids was 49.75% (95% CI 49.53–49.97) in 19 studies. Short- and long-acting β agonists were administered to a pooled population of 63.32% (95% CI 62.99–63.35) and 64.79% (95% CI 64.32–65.26) in 8 and 4 studies, respectively.

Drug utilization history.
Severity of Symptoms or Disease
Figure 5 presents the severity of asthma in the subjects included in our analysis. The highest proportion of subjects in our analysis were reported to have moderate to severe asthma (62.42% [95% CI 38.78–80.13%]), which was reported in 6 studies. Twelve studies included subjects with severe asthma, for which the pooled proportion was 26.17% (95% CI 16.55–37.11%). The pooled proportion of moderate and mild asthma were 20.64% (95% CI 10.62–32.95%) and 23.70% (95% CI 15.32–33.25%), respectively. In addition, some of the studies included in the analysis enrolled subjects with only moderate to severe asthma, so these results should be interpreted with caution.

Severity of symptoms.
Combination of Symptoms and Asthma Severity
Symptoms reported within a single study were presented as combinations. A total of 37 symptom combinations (defined as symptoms that exist concurrently in a subject) were reported in the included 67 studies (see the supplementary materials at http://www.rcjournal.com). We also calculated the average proportion of subjects affected by the different combinations of symptoms, the number of studies reporting the combination of symptoms, and the frequency of subjects with different severity of asthma (see the supplementary materials at http://www.rcjournal.com). In terms of prevalence, concurrent symptoms including wheezing, breathlessness, and bronchial hyper-responsiveness (combination 35) affected the highest number of subjects (n = 11,297), followed by combination 17, in which subjects were affected by symptoms of wheezing, breathlessness, chest tightness, cough, sneezing, runny nose/rhinorrhea, sleep disturbances, bronchial hyper-responsiveness, and sinusitis (n = 6,590). The least prevalent symptom combination was combination 20 (13.36%), which was a concurrent existence of wheezing, breathlessness, chest tightness, cough, exercise-induced bronchoconstriction, sleep disturbances, asthma exacerbations, and bronchial hyper-responsiveness.
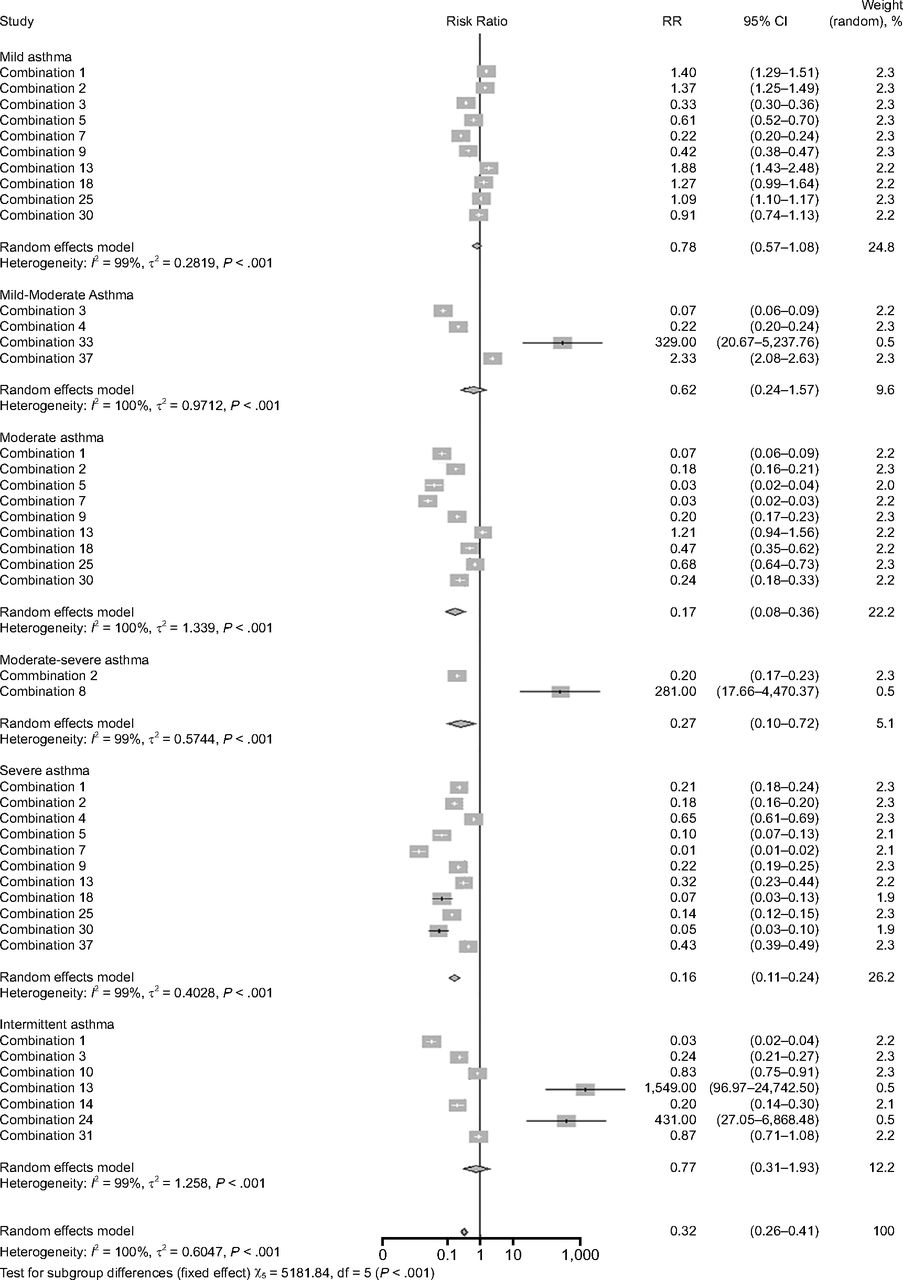
A random-effects model (heterogeneity 100%, τ2 0.6047, P = 0.004) was used to determine the association between the combination of symptoms and the risk of asthma (Fig. 6). The risk of mild asthma was 0.78 (95% CI 0.57–1.08), which occurred with combinations 1 (wheezing, breathlessness, chest tightness, and cough), 2 (bronchial hyper-responsiveness), 3 (wheezing), 5 (wheezing, breathlessness, cough), 7 (wheezing, breathlessness, chest tightness, cough, and bronchial hyper-responsiveness), 9 (cough), 13 (runny nose/rhinorrhea, nasal congestion), 18 (wheezing, breathlessness, exercise-induced bronchoconstriction, sleep disturbances, asthma exacerbation), 25 (asthma exacerbation, sinusitis), and 30 (wheezing, breathlessness, chest tightness, cough, exercise-induced bronchoconstriction).
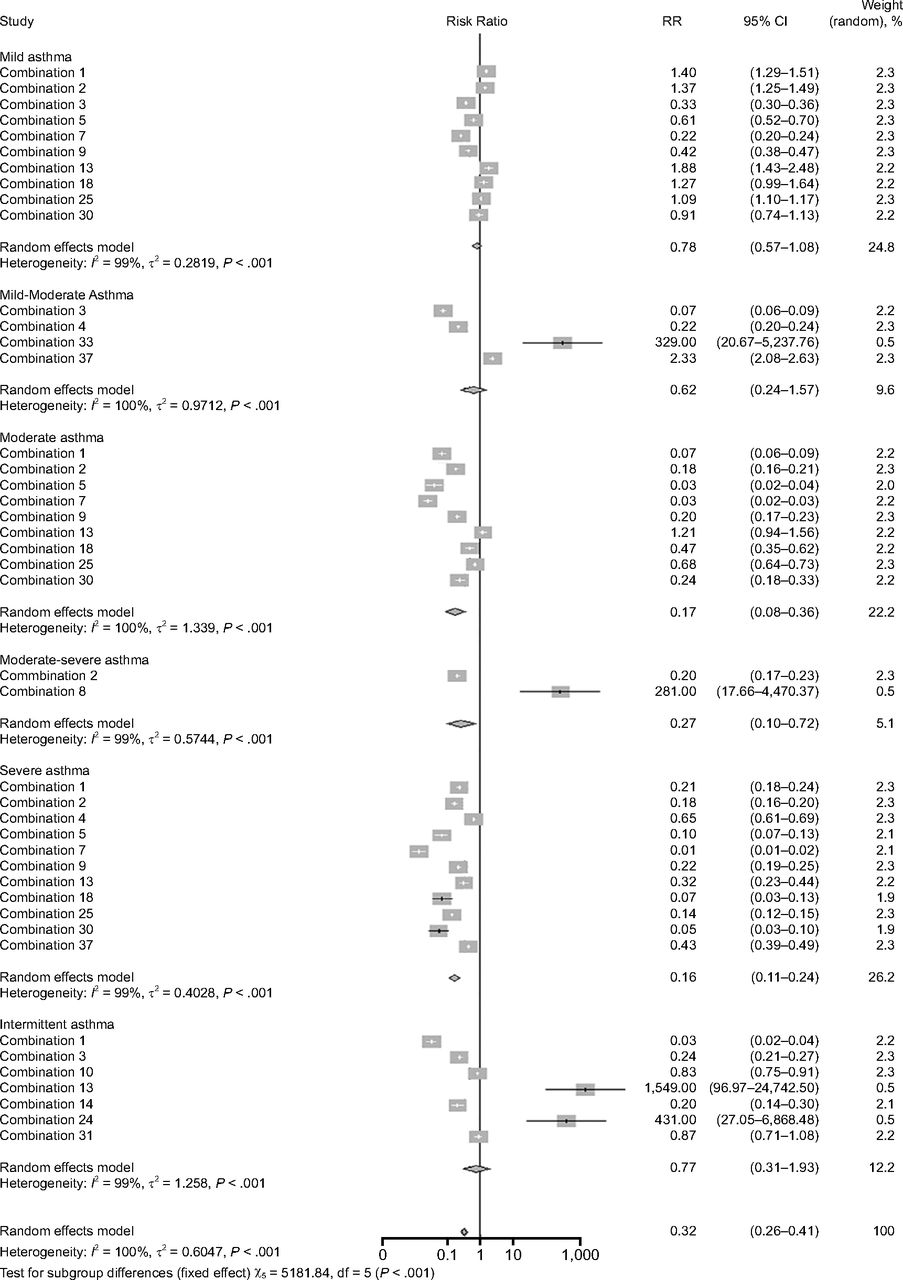
Risk of different asthma severities with different combinations of symptoms.
A relative risk of 0.62 (95% CI 0.24–1.57) was reported for mild to moderate asthma due to the symptoms in combinations 34 (wheezing, cough), 33 (wheezing, breathlessness, cough, exercise-induced bronchoconstriction), and 37 (wheezing, breathlessness, chest tightness, cough, sneezing, runny nose/rhinorrhea, nasal congestion, sleep disturbances). Presence of asthma symptoms in combinations 1, 2, 4, 5, 7, 9, 13, 18, 25, 30, and 37 were observed to be associated with a severe asthma risk (relative risk 0.16, 95% CI 0.11–0.24). The evidence from Figure 6 showed that multiple combinations of symptoms resulted in different severities of asthma, showing that all symptoms are important in the diagnosis of asthma severity. All of the symptom combinations showed a significant difference from each other in terms of severity of asthma (P < .001 for all), indicating that the presence of symptoms is a significant contributor in the diagnosis of disease and its severity. A scattered funnel plot confirmed the high degree of heterogeneity among the combination of symptoms reported in the studies (see the supplementary materials at http://www.rcjournal.com).
Discussion
This meta-analysis screened a multitude of articles and revealed 10 major signs and symptoms for the diagnosis of asthma in subjects age ≥ 14 y. Although the signs and symptoms of asthma are well documented, there is a lack of quantitative data on the frequency of most of the symptoms. Although the Global Initiative for Asthma (GINA) dissemination committee report determined the prevalence of symptoms, it was based on a country-wise approach and did not list the frequency of each symptom of asthma.83 To our knowledge, this meta-analysis is the first to evaluate the frequencies of major signs and symptoms in such a large population of asthmatics (N = 57,033), determining concurrent symptoms (defined as combinations) in subjects and identifying the relationship between the combination of symptoms and asthma severity. Although questionnaires are used for the diagnostic evaluation of adult asthma, they have their own limitations.84 In adults, asthma-screening questionnaires were developed for predicting disease in studies with either a small sample size (n = 2585 and n = 7886) or with short-term reproducibility of ≤ 73% for > 3 symptoms.86 Thus, use of questionnaires did not generate a sufficient amount of evidence for asthma diagnosis.87 However, the reproducibility of the asthma symptom questionnaire needs to be improved further for a higher number of symptoms.88 Due to these limitations, we planned to generate a new Chinese questionnaire to cover all aspects. The determination of frequencies of asthma symptoms in this meta-analysis, in a pooled population of > 50,000 subjects with asthma from multiple studies, will be useful in developing a questionnaire-based diagnostic tool that will allow better diagnosis of asthma in subjects age ≥14 y.
Multiple guidelines, including GINA (http://ginasthma.org/2017-pocket-guide-for-asthma-management-and-prevention, Accessed August 14, 2017), National Heart, Lung and Blood Institute Guidelines for the Diagnosis and Management of Asthma (https://www.nhlbi.nih.gov/health-pro/guidelines/current/asthma-guidelines/summary-report-2007, Accessed August 14, 2017), and the British Guideline on the Management of Asthma (http://sign.ac.uk/guidelines/fulltext/153/index.html, Accessed August 14, 2017) define asthma as the presence of symptoms including wheezing, breathlessness, chest tightness, cough, and air-flow obstruction. Of these, patients might experience one or more symptoms or multiple combinations. Further, hyper-responsiveness and underlying airway inflammation are also described as perpetrators of airway obstruction, and they can lead to the development of clinical symptoms. Although guidelines and previous studies have defined asthma as the presence of symptoms, we found no lists of the most frequently reported or experienced symptoms. This systematic review and meta-analysis of the published literature attempted to list the most frequently occurring individual symptoms and the most frequently reported combinations of symptoms in subjects with asthma. The presence of symptoms is the first presenting criteria for asthma for making a correct diagnosis before administering spirometry, peak flow measurements, and provocative challenges.89 Therefore, control of asthma also depends on controlling the symptoms. The questionnaire-based approach for determining control of asthma symptoms is also discussed in the GINA guidelines. The Asthma Control Questionnaire (http://www.thoracic.org/members/assemblies/assemblies/srn/questionaires/acq.php, Accessed April 14, 2017) and the Asthma Control test (http://www.thoracic.org/members/assemblies/assemblies/srn/questionaires/act.php, Accessed April 14, 2017) are standardized tools for determining the control of symptoms at regular intervals.
Results of our analysis showed that multiple symptoms coexisted in subjects at the time of diagnosis, which is in accordance with the definition from the guidelines. Additionally, except sneezing and runny nose, all of the symptoms were reported in > 38% of the subjects, making sneezing and runny nose the least frequently reported symptoms. The findings of our study also agree with individual studies reporting wheezing, coughing, dyspnea, and chest tightness among the most commonly reported symptoms.16,17,90 Rhinitis, allergy/atopy, and smoking were the most common factors in clinical or medical history evaluation. Further, 42.8% of subjects had a history of hospitalization due to respiratory symptoms, and 37.91% were exposed to risk factors at work. The factors assessed were in the scope of medical history assessment as described in the literature.91
Despite the fact that asthma is highly prevalent, it is still underdiagnosed.92 Studies have reported that physicians may not be completely able to diagnose asthma,93–95 which may be due to multiple reasons, including underreporting of symptoms by the subjects to health care practitioners94 or the moderate ability of the health care practitioners to interpret the findings of laboratory evaluations.91 A study conducted in China also reported a very low rate of physician-diagnosed asthma (1.4%),96 with another study reporting a decrease in trends of asthma diagnosis in Taiwan from 2000 to 2011. Another global cross-sectional study reported the prevalence of physician-diagnosed asthma at 0.19%, which was much lower than the reported global prevalence of 4.27%.97
Commonly Reported Symptoms in Asthmatics
Because symptoms and history are important aspects of asthma diagnosis, the role and responsibility of health care practitioners in diagnosing asthma at the earliest stages are significant. In our study, symptom combinations were found to be associated with the severity of asthma. However, only one symptom combination (combination 8) was specifically reported with moderate to severe asthma, with other symptom combinations reported consistently in all types of asthma. This was of particular interest because, although we saw a higher incidence of a few symptoms, their specificity with severity was poor, especially rhinitis, sneezing, and cough. Symptoms like wheezing, breathlessness, and chest tightness are commonly reported in all patients with asthma, regardless of the severity of the disease. Thus, the onset of these symptom combinations may help diagnose asthma earlier in the disease process and with a greater efficiency.
Our findings also support the results of a recently concluded clinical study, which reported that the frequency of respiratory symptoms is significantly associated with disease severity and usage of anti-asthma treatment.98 The results also highlight the importance of various combinations of symptoms reported in patients with asthma, and further research is warranted on the treatment aspect of asthma, including therapy initiation based on different symptom combinations. Thus, the correct evaluation of signs and symptoms of asthma at an early stage might have a clinical importance in application of effective treatment strategies and potentially better prognosis in subjects with asthma.89 Further, accurate diagnosis will also reduce concerns about overdiagnosis and underdiagnosis.99 We believe that the early diagnostic and clinical improvement in patients with asthma will translate into a reduction in economic burden, as demonstrated by Nunes et al2 From the perspective of clinicians, we believe support in accurate and early diagnosis will help standardize the practices followed for asthma diagnosis.
In the studies included in our meta-analysis, we reported asthma symptoms categorized as occurring during the day in 7 studies (38.81% of subjects) and occurring at night in 11 studies (32.26% of subjects). This might not be a correct representation of the timing of the symptoms because some studies did not report the frequency of symptoms based on time of day. However, evidence from the literature suggests that subjects with asthma experience symptoms throughout the day, with the frequency and severity of symptoms worsening with disease progression.100 The reason for a greater risk at night is due to different physiological changes in the body and comorbid diseases, which make asthmatics more susceptible to an exacerbation and poorer asthma control, quality of life, and sleep.101,102 Symptoms including wheezing, coughing, and chest discomfort have been reported to be more severe at night compared to during the day. Similarly, in terms of frequency of symptoms, wheezing, coughing, upper airway obstruction, and allergic symptoms were observed more frequently at night than during the day.103 It should be further noted that self-reported symptoms are more accurate and less susceptible to recall bias than symptoms reported by a parent or caregiver, which may aid clinicians in initiating early therapy and hence better outcomes.
Strengths and Limitations of the Analysis
Our study had several strengths. First, this comprehensive meta-analysis presented the symptoms and clinical history of asthma in > 55,000 subjects with asthma (age ≥ 14 y) from 67 studies performed in countries around the world. Second, the methodology we followed was compliant with the PRISMA guidelines for systematic reviews. Third, with the limitations of existing questionnaires, new instruments developed using the metadata of a large population should be more robust for the diagnosis of asthma.
Our study also had several limitations. First, we only included observational studies, but this would not affect the results because we considered only the baseline criteria for analysis; this was also the reason for not performing a subgroup or sensitivity analysis. Second, we could only identify respiratory medical history from the literature, and, therefore, classification of history according to system organ class was not possible. Third, there was a high degree of heterogeneity among the included studies, which required the use of a random-effects model. Finally, we considered all of the variants of asthma together and not as different entities. Due to these limitations, the results must be interpreted with caution.
Conclusions
From our analysis, it was evident that subjects with asthma largely present with a combination of symptoms, with nasal congestion, wheezing, chest tightness, sleep disturbances, and breathlessness being the most prevalent symptoms, affecting > 45% of the sample. Further, we also observed that most of the subjects with asthma had a history of rhinitis and allergy, and the majority were diagnosed with moderate to severe asthma. On the basis of our analysis, we conclude that the ranking of these symptoms and history can aid in improving diagnosis and in providing more appropriate asthma management and control. Again, based on the combination of symptoms reported, we suggest including commonly observed combined symptoms of wheezing, breathlessness, chest tightness, cough, sleep disturbances, and bronchial hyper-responsiveness, among others, during the development of a diagnostic-based questionnaire that will aid in an earlier diagnosis and prompt treatment.
Acknowledgment
The authors acknowledge Karan Sharma and Dr Amit Bhat (Indegene) for providing the necessary writing assistance and editorial support during development of this manuscript.
Footnotes
- Correspondence: Qianli Ma PhD MD, Institution of Respiratory Disease, Xinqiao Hospital of 3rd Military Medical University, Chongqing, China. E-mail: cqmql{at}163.com.
The authors were supported in part by AstraZeneca. The authors have disclosed no other conflicts of interest.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2020 by Daedalus Enterprises
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.
- 12.
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.
- 50.
- 51.
- 52.
- 53.
- 54.
- 55.
- 56.
- 57.
- 58.
- 59.
- 60.
- 61.
- 62.
- 63.
- 64.
- 65.
- 66.
- 67.
- 68.
- 69.
- 70.
- 71.
- 72.
- 73.
- 74.
- 75.
- 76.
- 77.
- 78.
- 79.
- 80.
- 81.
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}