

Abstract
BACKGROUND: Lung function parameters are used as signs in the diagnosis and evaluation of asthma; however, their sensitivity and specificity are not ideal. We calculated and combined angle β with lung function parameters to identify the ideal indicator.
OBJECTIVE: We aimed to identify an ideal indicator for evaluating the severity of airway obstruction in children with asthma.
METHODS: In total, 151 school-age children diagnosed with asthma were selected as the asthma group, and 106 healthy children were selected as the control group. The subjects were divided into the exacerbation group, chronic persistent group, and clinical remission group. Furthermore, the subjects were classified into mild and moderate groups or severe and critical groups. Angle β was calculated in each group. A receiver operating characteristic curve analysis was performed to determine the cutoff values of angle β and lung function parameters that together provided high sensitivity and specificity for airway obstruction evaluation in children with asthma.
RESULTS: The mean value of angle β in the asthma group was significantly smaller than that in the control group (178.18° and 196.72°, respectively, P < .001). More exacerbations or greater severity corresponded to smaller angle β values (P < .001). The best cutoff value of angle β was 189.43°, and the area under the receiver operating characteristic curve of angle β was 0.877, which is greater than the area under the receiver operating characteristic curve of FEV1, forced expiratory flow (FEF) at 75% vital capacity (FEF25%), and FEF at 50% vital capacity (FEF50%), but smaller than the area under the receiver operating characteristic curve of FEF75% and FEV1/FVC%. Interestingly, combining these measures can enhance the sensitivity and specificity in assessing airway obstruction.
CONCLUSIONS: Angle β was a useful indicator for assessing airway obstruction. Furthermore, angle β combined with FEV1, FEV1/FVC%, FEF25%, FEF50%, and FEF75% can enhance the sensitivity and specificity of airway obstruction evaluations.
- angle β
- routine pulmonary function testing
- asthma
- children
- maximum expiratory flow-volume curve
- spirometry
- airway obstruction
Introduction
Asthma is a common and potentially serious chronic disease that imposes a substantial burden on patients, their families, and the community. Asthma causes respiratory symptoms, limitation of activity, and flare-ups (ie, exacerbations) that sometimes require urgent treatment and may be fatal.1 Asthma is an inflammatory disease of the lower airways characterized by the presence of airway inflammation, reversible air-flow obstruction, and airway hyperresponsiveness and alterations of the normal structure of the airways.2 Spirometry is the most common lung function test available, is used extensively in both clinical practice and research studies, and is the most sensitive method to assess narrowing of the airways, which occurs in asthma and bronchiectasis.3 The American Thoracic Society/European Thoracic Society reissued equipment specifications and standardized guidelines in 2005.4 Pulmonary function assessment is an integral part of the clinical management of children with respiratory disease, and spirometry should be a standard part of the assessment of children who present to a pediatrician with chronic respiratory symptoms.3 Routine pulmonary function testing (PFT) is a simple but important procedure used to detect air-flow limitation.5
Air-flow obstruction is indicated by a reduction in both values of the FEV1/FVC% relative to reference or predicted values6 and is usually characterized by a gradual curvilinear decrease in flow after the peak expiratory flow (PEF).7 Furthermore, the FVC and forced expiratory flow (FEF) at 25%, 50%, and 75% (FEF25%, FEF50%, and FEF75%, respectively) of the vital capacity also represent air-flow obstruction. Flows at high lung volumes represent the caliber of the central (large) airways (FEV1%), whereas flows at low lung volumes primarily represent the caliber of peripheral (small) airways (FEF25%, FEF50%, and FEF75%).8,9 Spirometry has been the most widely used measure of lung function, but no systematic studies of all spirometric tests in terms of sensitivity and specificity have been performed,10 therefore, identifying a more sensitive and specific indicator to evaluate airway obstruction in children with asthma is necessary.
The maximum expiratory flow-volume curve depicts the interrelationship between flow and volume during maximum expiration.11 Slowing of the expiratory flow that results from air-flow obstruction induces a concave shape in the maximum expiratory flow-volume curve during forced exhalation.12 As determined in a previous study,13 a concave maximum expiratory flow-volume curve is a sensitive indicator of air-flow limitation and can be detected in subjects with normal values of traditional lung function parameters. Previous studies identified angle β, which refers to the descending branch of the maximum expiratory flow-volume curve, as a marker to characterize the shape of the maximum expiratory flow-volume curve and found that subjects with asthma had a significantly lower angle β than did healthy individuals.6,12,14
However, these previous studies were conducted in single centers and included small sample sizes and single-factor comparisons. To identify an ideal indicator for evaluating the severity of airway obstruction in children with asthma, the marker angle β combined with FEV1, FEV1/FVC%, FEF25%, FEF50%, and FEF75% was applied in this study. Furthermore, we analyzed and investigated changes in angle β in children with asthma at different stages, including during an exacerbation, in a multi-center study that involved additional samples. The purposes of this study were to determine the best cutoff value of angle β to differentiate children with asthma from healthy children and to combine angle β with FEV1, FEV1/FVC%, FEF25%, FEF50%, and FEF75% to improve the sensitivity and specificity in assessing airway obstruction in children with asthma.
QUICK LOOK
Current knowledge
Angle β has been found to be an indicator that can be used to evaluate the severity of airway obstruction. Previous studies focused on preschool-age children. To increase the discriminating accuracy, these studies investigated single groups at single centers to calculate and combine angle β with the fractional concentration of exhaled nitric oxide or maximum mid-expiratory flow. Identifying more sensitive and specific indicators of airway obstruction is important.
What this paper contributes to our knowledge
Our multi-center study found that the best cutoff value of angle β was 189.43° in children with asthma. More severe exacerbations of asthma corresponded to smaller angle β values. Likewise, more severe airway obstruction corresponded to smaller angle β values. Angle β combined with FEV1%, FEV1/FVC%, forced expiratory flow at 25%, 50%, and 75%, especially angle β combined with the forced expiratory flow at 25% and FEV1/FVC% can enhance the sensitivity and specificity of airway obstruction severity evaluations.
Methods
Study Design: Clinical Research
In total, 151 school-age children (64 females; mean ± SD age, 8.66 ± 2.17 y) diagnosed with asthma at the Department of Internal Medicine Asthma Clinic of the Third Affiliated Hospital of Zhengzhou University, the Department of Pediatric Respiratory Medicine of Luoyang Women and Children's Medical Care Center of Henan Province, and the Department of Pediatric Respiratory Medicine of Luohe Children's Hospital of Henan Province, were recruited for the present study. Asthma was defined based on the Global Initiative for Asthma guidelines.1 The control group included 106 normal children (58 females; mean ± SD age, 8.86 ± 1.57 y) without a history of asthma or related respiratory symptoms as defined by the International Study of Childhood-Asthma Control Test and Asthma Therapy Assessment questionnaire15 recruited from the First Affiliated Primary School of Zhengzhou University. None of the subjects had a respiratory infection for at least 1 month before study inclusion. To ensure an appropriate sample, we excluded 12 subjects who were not well-matched based on the lung function test. This study was reviewed and approved by the ethics committee of the Third Affiliated Hospital of Zhengzhou University, and written informed consent was obtained from all the subjects and their parents.
Specific Experimental Methods
The subjects were grouped according to the different stages of asthma and different severity of acute asthma episodes. The children with asthma were divided into an exacerbation group, chronic persistent group, and clinical remission group according to the different stages of asthma. In addition, subjects with asthma were classified into mild and moderate group or severe and critical group based on the severity of the asthma exacerbation. Angle β was calculated in each group. Receiver operating characteristic (ROC) curve analyses were performed to determine the best cutoff value, and the area under the curve (AUC) of angle β, FEV1, FEV1/FVC%, FEF25%, FEF50%, FEF75%, and angle β combined with the above lung function parameters.
PFT
Routine PFT is safe for patients in the context of established screening preparticipation guidelines.16 Spirometry is the accepted standard and method of choice for the diagnosis of obstructive airway diseases. Spirometry is also the most commonly performed PFT in pulmonary diagnostics in adults and in children ages > 6 y.17 PFT was performed by using a pediatric lung function apparatus (Type MasterScreen IOS, Cardinal Health Germany, Hoechberg, Germany) according to American Thoracic Society/European Thoracic Society recommendations.4 The lung function tests were performed between 2:00 pm and 5:00 pm. The following variables were obtained from the best of 3 reproducible forced expiratory maneuvers6,18: FVC, FEV1, FEV1/FVC%, PEF, FEF25%, FEF50%, and FEF75%. The multi-center pulmonary function technicians (YZ, CC) were trained and qualified by the national children's pulmonary function cooperation group and received a certificate before performing tests to ensure homogeneity in the multi-center lung function test. Moreover, incentive programs (such as the blowing balloons program) were used to train the children to perform rapid forced expiration, which helped each child generate his or her best PEF values.
Calculation of Angle β
The curvilinearity of the maximum expiratory flow-volume curve was determined by angle β,6 which is the connecting line between the PEF point that corresponds to the vertex of the maximum expiratory flow-volume curve on the y-axis, FEF50% on the corresponding point of the descending branch of the maximum expiratory flow-volume curve with the radian, and the end line on the corresponding point of the exhaled air on the x-axis. Angle β is used to describe the shape of the descending branch of the maximum expiratory flow-volume curve. Angle β was calculated based on the method of Kapp et al,14 as follows: β = 180°− tan−1([PEF − FEF50%])/(0.5 × FVC) + tan−1 (FEF50%/[0.5 × FVC]). All tan−1 values were calculated in degrees (Fig. 1A).

Characteristics of angle β in children with asthma at different stages. Illustrations of the concave (A), linear (B), and convex (C) shapes of the maximum expiratory flow-volume (MEFV) curve. D: Comparison of the P value of various values of angle β during different stages of asthma. Angle β was smaller during exacerbation (178°) than during the chronic duration period (191.5°, P =.034) and clinical remission period (200.3°, P < .001). Angle β was smaller during the chronic duration period than that during the clinical remission period (P = .037). All data are presented as mean ± SD. PEF = peak expiratory flow; FEF = forced expiratory flow.
Statistical Analysis
All statistical analyses were performed with statistics software (SPSS 21 [SPSS, Chicago, Illinois] and R 2.2.1 [Alcatel-Lucent, Murray Hill, New Jersey]). The descriptive data of the demographic and clinical characteristics (continuous and categorical variables) of the study subjects were analyzed as frequencies, which represented the mean and 95% CIs. The measurement data are expressed as the mean ± SD. A univariate analysis of variance was used for the multi-group comparison, and an independent-samples t test was used for pairwise comparisons. The count data are expressed as percentages, and the sensitivity and specificity of the factor correlations were analyzed by ROC curve analysis. The combinations of angle β with FEV1, FEV1/FVC%, FEF25%, FEF50%, and FEF75% were analyzed by using a logistic regression model, and the prediction probability was used as a discriminating indicator. A P value of <.05 was considered to indicate a statistically significant difference.
Results
The characteristics of the subjects are shown in Table 1. In total, 151 subjects were included in the asthma group, and 106 healthy children were included in the control group; the children were ages 6–14 y. No differences in age, sex, height, or weight were identified between the two groups (P > .05). However, the lung parameters (FVC, FEV1, FEV1/FVC, PEF, FEF25%, FEF50%, and FEF75%) varied, especially angle β.
Subject Characteristics
Schachter et al19 previously found that classifying lung function by the different stages of asthma can be useful for delineating disease. In our study, we divided the subjects into exacerbation, chronic duration, and clinical remission groups according to the different stages of asthma. The characteristics of angle β at different stages in children with asthma are described in Figure 1. During the exacerbation period, the value of angle β was 178.0°, which corresponded to the concavity of the maximum expiratory flow-volume curve (Fig. 1A). During the chronic duration period, the value of angle β was 191.5°, which corresponded to a maximum expiratory flow-volume curve with a linear shape (Fig. 1B). During the clinical remission period, the value of angle β was 200.3°, which indicated the convexity of the maximum expiratory flow-volume curve (Fig. 1C).
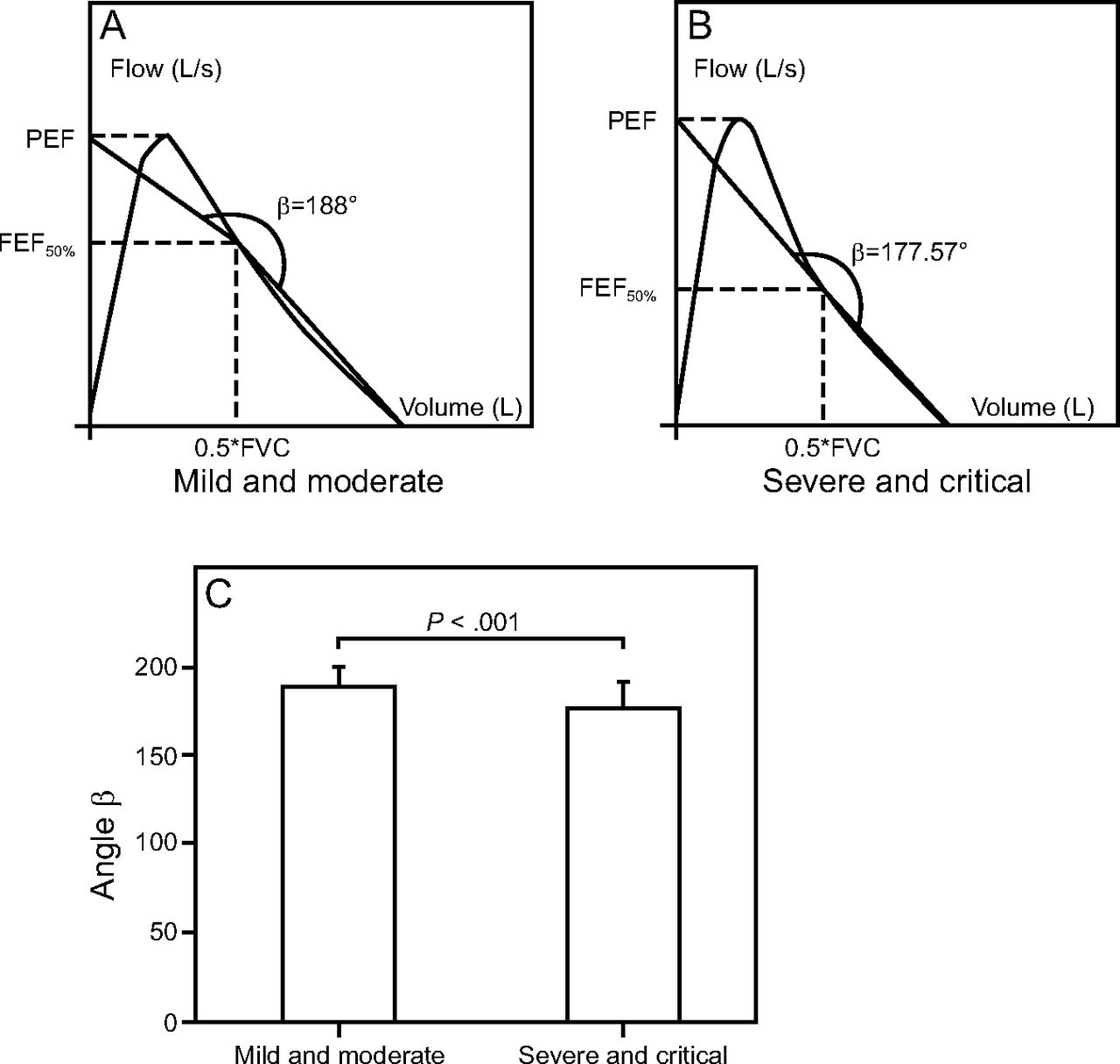
As shown in Figure 1D, during the exacerbation period, the value of angle β was obviously smaller than those during the chronic duration period (P = 0.034) and the clinical remission period (P < .001). Furthermore, the value of angle β during the chronic duration period was smaller than that during the clinical remission period (P = 0.037). Subsequently, we compared the value of angle β and the corresponding P value by varying degrees of severity during exacerbation episodes (Fig. 2). In the mild and moderate group, the shape indicated by angle β corresponded to a linear maximum expiratory flow-volume curve (Fig. 2A).

Angle β with different degrees of severity during the acute phase in children with asthma. Graphic description of the linear (A) and concave (B) shapes of the maximum expiratory flow-volume curve. C: Comparison of angle β and P values during acute asthma episodes with varying degrees of severity. The value of angle β differs between the mild and moderate groups (188.96° ± 12.76°) and the severe and critical groups (177.57° ± 14.04°, P < .001). All data are presented as the mean ± SD. PEF = peak expiratory flow; FEF = forced expiratory flow.
In the severe and critical group, the shape indicated by angle β corresponded to concavity of the maximum expiratory flow-volume curve (Fig. 2B). During an asthma exacerbation, more-severe symptoms corresponded to smaller angle β values. The values of angle β were smaller in the severe and critical group than those in the mild and moderate group (P < .001) (Figure 2C). Taken together, an analysis of our data indicated that angle β played an important role in the evaluation of airway obstruction in children with asthma at different stages and with different degrees of severity during exacerbation.
To determine whether angle β can improve the sensitivity and specificity in evaluating the degree of airway obstruction in children with asthma, we generated ROC curves to ascertain the precision of angle β, FEF25%, FEF50%, FEF75%, FEV1%, FEV1/FVC%, and their combinations in the evaluation of children with asthma (Fig. 3). The characteristics of angle β, FEF25%, FEF50%, FEF75%, FEV1%, and FEV1/FVC% are listed in Table 2.
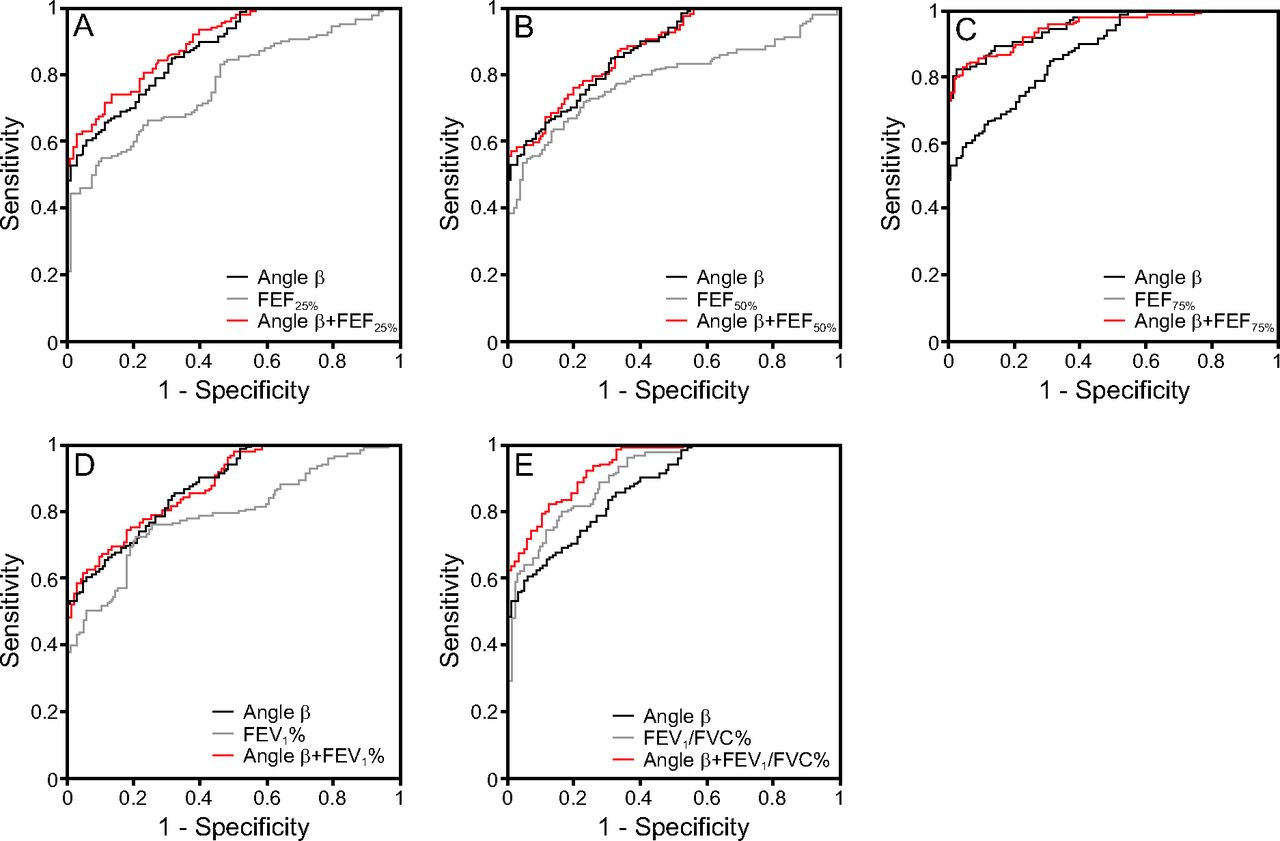
Receiver operating characteristic (ROC) curves of angle β, FEF25%, FEF50%, FEF75%, FEV1%, FEV1/FVC% and their combinations. ROC curve characteristics marking the sensitivity and specificity of angle β, FEF25% (A), FEF50% (B), FEF75% (C), FEV1% (D), FEV1/FVC% (E), and their combinations in the detection of children with asthma. The area under the ROC curves of angle β, FEF25% and angle β combined with FEF25% (A), the areas under the ROC curves of angle β, FEF50%, and angle β combined with FEF50% (B), the areas under the ROC curves of angle β, FEF75%, and angle β combined with FEF75% (C), the areas under the ROC curves of angle β, FEV1% and angle β combined with FEV1% (D), and the areas under the ROC curves of angle β, FEV1/FVC%, and angle β combined with FEV1/FVC% (E); a larger area corresponds to greater sensitivity and specificity. FEF = forced expiratory flow.
Distinguishing the Accuracy of Angle β, FEV1%, FEV1/FVC%, FEF25%, FEF50%, FEF75%, and Combinations
As shown in Figure 3.A, B, D, the AUC of angle β was larger than those of FEF25%, FEF50%, and FEV1%. In addition, the AUC of the combinations of angle β with FEF25%, FEF50%, and FEV1% were markedly increased, which indicated that angle β combined with FEF25%, FEF50%, and FEV1% can increase the sensitivity and specificity in evaluating airway obstruction in school-aged children with asthma. In particular, angle β combined with FEF25% produced a more significant result. Analogously, as shown in Figure 3.C, E the AUC of angle β was smaller than those of FEF75% and FEV1/FVC%. However, the AUC of the combinations of angle β with FEF75% and FEV1/FVC% were increased. Interestingly, compared with angle β, FEF75%, or FEV1/FVC% alone, the combination of angle β with FEF75% or FEV1/FVC% can improve the sensitivity and specificity in evaluating the degree of airway obstruction in children with asthma. In particular, angle β combined with FEV1/FVC% produced a more significant result.
The AUCs and the best sums of the sensitivity and specificity of the cutoff values of angle β, FEV1%, FEV1/FVC%, FEF25%, FEF50%, and FEF75% are shown in Table 2. Interestingly, compared with angle β, FEV1%, FEV1/FVC%, FEF25%, FEF50%, and FEF75% alone, the AUC of the combinations of angle β with FEV1%, FEV1/FVC%, FEF25%, FEF50%, and FEF75% were improved 12.1%, 3.1%, 13.6%, 10.6%, and 0.4%, respectively, which suggests that angle β combined with FEV1%, FEV1/FVC%, FEF25%, FEF50%, and FEF75% can improve the sensitivity and specificity in assessing the airway obstruction severity in children with asthma, especially angle β combined with FEF25% and FEV1%.
The distribution of children with asthma according to the values of angle β, FEF25%, FEF50%, FEF75%, FEV1%, and FEV1/FVC% are shown in Figure 4. Analysis of these data showed that, in the asthma group, the values of angle β and the pulmonary function parameters that represent airway size (FEF25%, FEF50%, FEF75%), the degree of obstruction (FEV1%), and whether the airway is obstructed (FEV1/FVC%) were relatively small, and most values were concentrated in the lower left corner of the scatter plot. In the control group, the values of angle β and the lung function parameters (FEF25%, FEF50%, FEF75%, FEV1%, and FEV1/FVC%) were relatively larger than the best cutoff values and were mainly concentrated in the upper right side of the scatter plot. The best cutoff values of angle β, FEF25%, FEF50%, FEF75%, FEV1%, and FEV1/FVC% provided an objective basis for assessments of airway obstruction and corresponding severity in children with asthma.
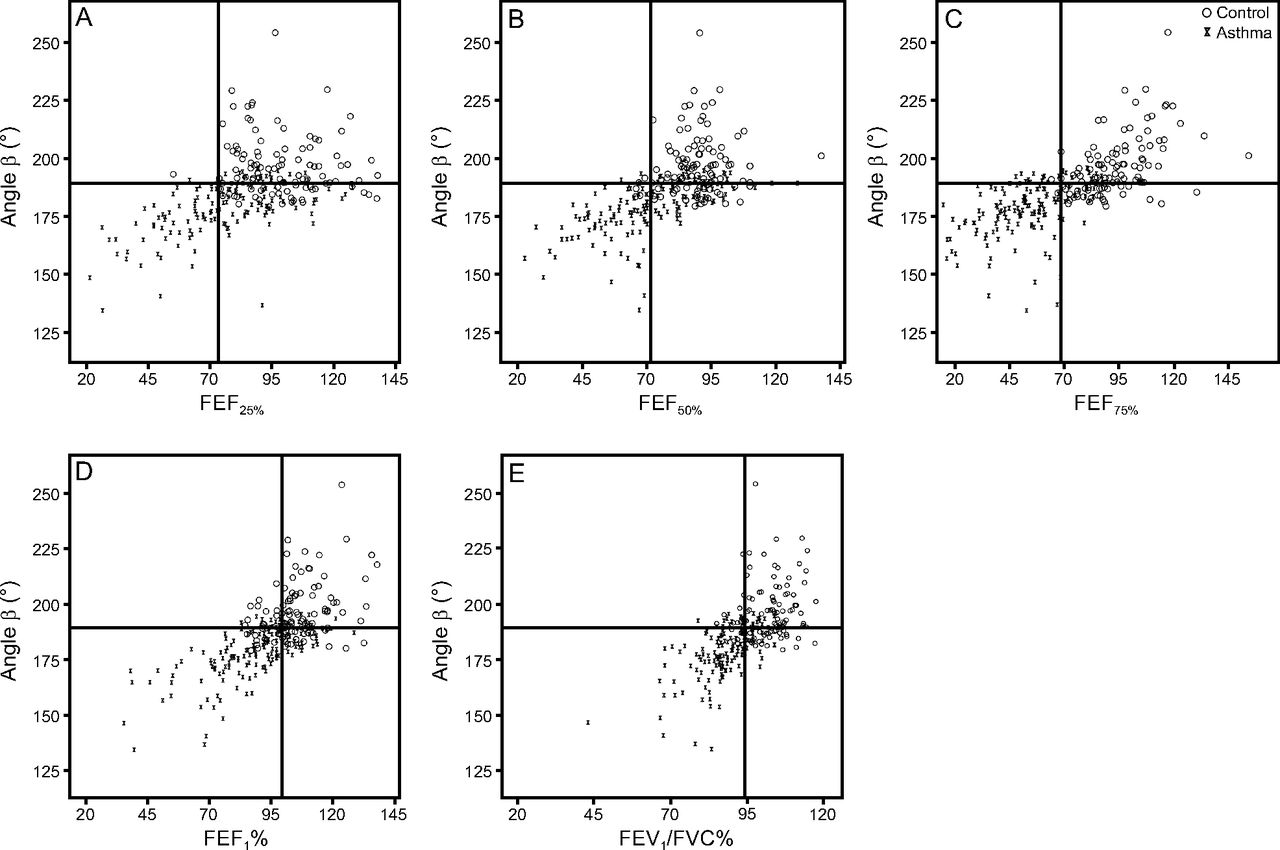
The distribution characteristics of angle β, FEF25%, FEF50%, FEF75%, FEV1%, and FEV1/FVC%. The lines indicate the best cutoff values of angle β, FEF25%, FEF50%, FEF75%, FEV1%, and FEV1/FVC% for the detection of children with asthma. Each diagram shows statistical significance (P < .001). FEF = forced expiratory flow.
Discussion
A concave maximum expiratory flow-volume curve represents airway obstruction,20 which serves as a proxy of asthma disease severity or lack of control, and may be used to identify patients at risk for severe exacerbations.21 In this study, we described angle β quantitation of the radian of the maximum expiratory flow-volume curve to estimate the severity of airway obstruction in children with asthma. Furthermore, we found that the mean value of angle β in our healthy individuals was >180°, which corresponded to an maximum expiratory flow-volume curve with a convex shape, which was consistent with observations reported in previous studies22–24 that describe how the descending limb of the maximum expiratory flow-volume curve is convex in young children with rapid cessation of flow toward the end of the forced expiration maneuver.
In addition, our findings also extend the literature by providing the value of angle β in children who were undergoing PFTs and showed that this population had smaller angle β values than healthy peers. To our knowledge, some previous studies6,14,25 compared the values of angle β between children with asthma and healthy individuals. A similar study demonstrated that children with wheezing disorders had lower angle β values than healthy individuals.25 In addition, Kapp et al14 observed that children and adults with chronic bronchitis or asthma have a significantly lower mean angle β. The values of angle β in this study were consistent with those of previous studies,6,14 which confirmed the feasibility of our study.
A concave flow-volume curve has been described in a few studies that investigated childhood asthma.26,27 Linna26 reported that a concave-shaped flow-volume curve is the most sensitive indicator of airway obstruction and predicts the severity of asthma better than conventional flow values. In healthy subjects, flows during forced expiration are almost homogenous, and the shape of the curve, therefore, is linear. However, in subjects with airway obstruction, which is usually accompanied by hyperinflation of the lungs, flows are more or less nonhomogenous in the different bronchi, which may explain the concave pattern of the curve but does not explain the convex shape of the curve. In this study, we showed that more-severe airway obstruction in this population corresponded to a more concave curve and that, because children with asthma experienced gradual relief of airway obstruction and their condition gradually improved, angle β gradually increased and the shape of the curve gradually became convex, which represented a better explanation for the convex shape of the curve.
We also generated ROC curves to ascertain the precision of angle β alone and combined with pulmonary function parameters in the evaluation of children with asthma. We found that, when evaluating airway obstruction, angle β was a sensitivity and specificity indicator, and angle β combined with FEF25%, FEF50%, FEF75%, FEV1%, and FEV1/FVC% could increase the sensitivity and specificity in evaluating airway obstruction, with angle β combined with FEF25% producing a more significant result. Zhang et al27 suggest that the severity of asthma in children can be predicted at the first visit based on a concave flow-volume curve and the frequency of symptoms. In this study, we used the size of angle β to describe the flow-volume curve and to assess the severity of airway obstruction and changes in asthma. Unlike previous studies, we did not compare the symptoms of children with asthma, which we will consider in future studies.
To the best of our knowledge, this study was the first to provide the values of angle β in children with asthma. The values of angle β are essential because the shape of the maximum expiratory flow-volume curve changes according to the 3 different stages of asthma and 2 types of severity during an exacerbation in children. The values of angle β are also more practical for routine use. We showed that, in the various stages of asthma, more exacerbation corresponds to a smaller angle β, and, during exacerbations, a greater severity corresponds to a smaller angle β, which indicated more concave maximum expiratory flow-volume curves. Furthermore, angle β had the best accuracy in discriminating the maximum expiratory flow-volume curve shape of children with asthma from that of healthy children. We also showed that angle β can detect changes associated with air-flow obstruction. In a previous study, it was reported that angle β also varies with the pattern of abnormal lung function.19 Angle β in obstructive (moderate and severe) and restrictive lung function patterns is significantly lower than angle β in a normal pattern. Consistent with this previous study, the current study demonstrated that severe and critical obstructive lung function in children with asthma is associated with a smaller angle β than that associated with mild and moderate airway obstruction.
Our study aimed to identify spirometric parameters to enhance the sensitivity and specificity of airway obstruction evaluations in children with asthma. Previous studies attempted to combine angle β with the fractional concentration of exhaled nitric oxide (FENO) to enhance the discriminating accuracy.6 In addition, Weiner et al28 analyzed an objective index, that is, angle β combined with maximum mid-expiratory flow, and verified that this combination performs well in evaluating air-flow limitation and could be automatically calculated, accurately matched the mean expert score, and was also significantly associated with the risk of hospitalization, however, wide variability was noted in the intersubject assessment. In contrast to previous studies, this study combined angle β with pulmonary function parameters, which represented the small airways (FEF25%, FEF50%, FEF75%), the degree of obstruction (FEV1%), and whether the airway is obstructed (FEV1/FVC%), and found that such combinations can improve the sensitivity and specificity in assessing airway obstruction severity in children with asthma.
The purpose of our study was not to replace conventional spirometric indices with angle β, but to provide an objective tool to enhance the sensitivity and specificity of airway obstruction evaluations. In a previous study, the original sample size prevented an adequate analysis of specific clinical outcomes;28 an index that can improve the sensitivity and specificity of the assessment of the obstructive process is needed. Our ROC curve analysis served as a useful and objective tool that is complementary to FENO or maximum mid-expiratory flow and enhances the sensitivity and specificity of airway obstruction assessment. Lung function spirometric evaluations and angle β measurements are relatively simple to perform in nearly all children.4 According to our findings, the combined use of angle β and FEF25%, FEF50%, FEF75%, FEV1, and FEV1/FVC% may be a practical strategy that can help clinicians detect children with asthma, especially when patients have only mild clinical symptoms.
The values of angle β, FEF25%, FEF50%, FEF75%, FEV1%, and FEV1/FVC% in most children with asthma are lower than the best cutoff values (189.4°, 73.30%, 71.55%, 68.25%, 99.35%, and 93.5%, respectively) and are mainly concentrated in the bottom left of the scatter plot, although these values can be greater than the corresponding best cutoff values in some children with asthma and, therefore, are mainly concentrated in the bottom right of the scatter plot. The reason may be that, during different periods of asthma, the degree of airway obstruction differs, especially during clinical remission of asthma when angle β is close to normal. Similarly, in most control group, the values of angle β, FEF25%, FEF50%, FEF75%, FEV1%, and FEV1/FVC% are greater than the best cutoff values and are mainly concentrated in the bottom right of the scatter plot, but these values can be smaller than the corresponding best cutoff values in other control group and, therefore, are mainly concentrated in the bottom left of the scatter plot. A possible explanation is that different age groups may have different reference ranges. The distribution area of the corresponding scatter plot differs when angle β is combined with different lung function parameters.
A previous study evaluated the distributions of angle β and FENO in a scatter plot and showed that the asthma group's angle β and FENO were mainly distributed below the scatter plot, whereas the control group's angle β and FENO were mainly distributed above the scatter plot because the children with asthma had a small angle β and a large FENO, whereas the normal children had a large angle β and a small FENO.6 The best cutoff value for each index can be found in the distribution area of angle β and the scatter diagram, combining the different indices in children with asthma, which may be helpful in guiding clinical practice.
One shortcoming of this analysis was that angle β may be affected by subjective factors, such as poor coordination in lung function testing and inadequate force during expiration. The pulmonary function maneuver is a subjective criterion that is difficult to assess. Therefore, we attempted to avoid these subjective factors during participant selection. Furthermore, we removed subjects who were not well matched according to the lung function test. Another shortcoming of this analysis was that our study was cross-sectional and lacked longitudinal data that reflected the day-to-day variability in angle β in children; therefore, the changes in angle β cannot be interpreted comprehensively.
Conclusions
We calculated angle β to confirm the intuitive concept that has long been familiar to clinicians, namely, that the shape of the maximum expiratory flow-volume curve reflects the degree of airway obstruction in children with asthma. In addition, our study demonstrated that the sensitivity and specificity of assessing airway obstruction severity in children with asthma can be improved by combining angle β with pulmonary function parameters obtained by ROC curve analysis. Therefore, as shown in this study, detecting the curvilinearity of the maximum expiratory flow-volume curve has the potential to improve the assessment of early airway obstruction in children with asthma. Angle β as an assessment tool may be useful for lung disease research and applications, particularly airway obstructive disease research.
Acknowledgments
The authors thank Dr Lin-lin Zhang, who provided valuable comments on the manuscript.
Footnotes
- Correspondence: Yanli Zhang MD PhD, Department of Pediatrics, the Third Affiliated Hospital of Zhengzhou University, No. 7 Rehabilitation Before Street, Erqi District, Zhengzhou City, Henan Province 450052, China. E-mail: 30562393{at}qq.com.
The authors have disclosed no conflicts of interest.
- Copyright © 2020 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}
{kind=link}