

Abstract
BACKGROUND: Respiratory ICUs (RICUs) have recently been implemented in France to fill the gap between ICUs and respiratory wards for patients who will require prolonged mechanical ventilation (PMV). The aim of this study was to describe the outcomes of subjects with tracheostomy who were undergoing PMV before and after implementing a RICU in our hospital.
METHODS: Two cohorts were studied and followed up for 1 year. Cohort 1 included 66 subjects from December 2010 to December 2012, before implementing the RICU. Cohort 2 included 103 consecutive subjects included in the RICU from January 2016 to June 2017.
RESULTS: In cohort 2, lung and airway diseases were the main causes of chronic respiratory failure in 91.3% of the subjects versus 47.0% of the subjects in cohort 1 (P < .001). During the follow-up, 34.8% and 24.3% of the subjects in cohorts 1 and 2, respectively, were readmitted at least once (P = .14), which corresponded to 109 and 137 stays for cohorts 1 and 2. The median (95% CI) length of stay was 42 (37–50) d in the pre-RICU period versus 29 (26–33) d in the RICU period (P < .001). A complete or partial weaning was achieved in 30.3% of stays in the pre-RICU period versus 69.3% of stays in the RICU period (P < .001). The in-hospital mortality rate was 14.7% and 7.3% in the pre-RICU and RICU periods, respectively (P = .10). The 1-year survival did not differ between cohorts: 60.6% versus 53.9% in cohorts 1 versus 2; P = .42).
CONCLUSIONS: Implementing a RICU improved the outcomes of the subjects with tracheostomy who were undergoing PMV by reducing the length of stay and increasing complete or partial weaning. However, the 1-year survival remained unchanged.
- chronic respiratory failure
- health outcomes
- intermediate care facility
- respiratory intensive care units
- prolonged mechanical ventilation
- tracheostomy
Introduction
Mechanical ventilation is increasingly used in the management of acute respiratory failure,1 and up to one third of the patients who require mechanical ventilation will undergo tracheostomy.2 Among these patients, a population-based cohort study3 reported that 5% of patients would undergo prolonged mechanical ventilation (PMV) defined by at least 21 d of mechanical ventilation for ≥ 6 h/d.4 This proportion is supposed to increase because of the greater impact of care given to elderly people and patients with comorbidities.5 The recovery of patients undergoing PMV is a long and difficult process that will require specialized units dedicated to subject rehabilitation and functional restoration. These units are justified outside of the ICU if patients recover enough to survive without the close monitoring and supportive care provided by ICUs.6 There is a high variability in the terminology and definition of these units,7 which may even include medical wards because of a shortage in specialized beds.8
Respiratory ICUs (RICUs) have been implemented in the United States and in Europe9,10 to fill the gap between ICUs and respiratory wards to decrease medical costs, free up ICU beds, and initiate patient rehabilitation.11 Important benefits may be expected from this care pathway in terms of costs, staff management, and better use of ICU beds through the admission of patients who really need intensive care.12,13 Until 2015, in Île de France, which is the most populated French region, such units were sparsely available and patients on PMV were often managed in intermediate care facilities.14 In this region, the Public Health Authority (Agence Régionale de Santé) issued, in 2014, specifications for the opening of RICUs (Services de Rééducation Post-Réanimation https://www.iledefrance.ars.sante.fr/system/files/2018-03/SSR-Cahier-des-charges-SRPR-2013.pdf, Ac-cessed March 24, 2019).
Data on the care trajectories of subjects on PMV and outside of the ICU, especially in community-based European centers, are limited.15 Our previously described intermediate care facility that provided care to patients on PMV16 has recently been replaced by a RICU according to the 2014 Agence Régionale de Santé specifications. The aim of this study was thus to compare the outcomes of subjects who had tracheostomy and undergoing PMV before and after the implementation of a RICU in our hospital since January 2015.
QUICK LOOK
Current Knowledge
Respiratory ICUs (RICUs) have recently been implemented in France to fill the gap between ICUs and respiratory wards for patients who require prolonged mechanical ventilation (PMV). Important benefits may be expected from this care pathway in terms of costs, staff management, and better use of ICU beds through the admission of patients who really need intensive care. Data on the care trajectories of patients on PMV outside of the ICU are limited, especially in community-based European centers.
What this paper contributes to our knowledge
After a 1-year follow-up, we showed that implementing a RICU improved the outcomes of the subjects with tracheostomy and on PMV by reducing the length of stay, readmissions, and by increasing the rate of complete or partial weaning. There were fewer cases of respiratory sepsis and more cases of non-respiratory sepsis during the RICU period than during the pre-RICU period. However, the 1-year survival remained unchanged.
Methods
Study Population
The Bligny Hospital Center is a 374-bed community-based general hospital that offers acute care and rehabilitation units for patients with respiratory, cardiac, diabetic, and oncologic diseases. Patients who are recovering from acute respiratory failure that occurs in chronic respiratory failure are admitted in our respiratory department. Before 2015, they were managed in an intermediate care facility that was included in the respiratory department. The outcomes in this unit were previously described.16 The RICU opened in January 2015 as a 12-bed integrated subunit of the 64-bed respiratory department. All patients receive comprehensive management, including invasive and noninvasive ventilation, oxygen therapy, and rehabilitation. Beds are fully equipped for the management of patients who require invasive PMV through tracheostomy.
The study population consisted of 2 groups of patients admitted to our hospital before and after the opening of the RICU. Cohort 1 included 66 subjects from December 1, 2010, to December 1, 2012 (pre-RICU period). Patients came from home, acute care respiratory wards, or ICUs located in our hospital or in the Île de France region. Cohort 2 included all consecutive subjects admitted in the RICU from January 1, 2016, to June 30, 2017 (RICU period). This period was chosen to allow complete training of the care teams when the RICU was opened, the steady setup of a continuous flow of patients, and a complete 1-year follow-up at the end of the study.
Patients admitted to the RICU came exclusively from ICUs located in our hospital or in another hospital. They were eligible for inclusion in the study if they had a tracheostomy tube maintained in place for >7 d and were clinically stable when the decision was made to transfer them. They were excluded from the study if an end-of-life decision had previously been taken. The RICU staff included 2 physicians and 2 physical therapists. The nurse-to-subject ratio was 1:6. An important increase in the rate of activity devoted to the management of patients who require PMV through a tracheostomy tube was observed between our 2 cohorts (from 19% in our previously described unit16 to 68% in our RICU), which led to an almost 2-fold difference in the size of the 2 cohorts.
Data Collection
The following data were recorded on admission for all the subjects: demographics (age, sex, body mass index), age-adjusted Charlson comorbidity score; vital laboratory data and arterial blood gases; the simplified index of gravity score was obtained only in cohort 2.17 No subject underwent hemodialysis during the hospital stay.
All the subjects had chronic respiratory failure, whose cause was classified into 3 categories according to the Eurovent survey18: (1) lung and airway diseases: COPD, cystic fibrosis, bronchiectasis, pulmonary fibrosis; (2) rib cage abnormalities: kyphoscoliosis, tuberculosis sequelae (eg, thoracoplasty), obesity hypoventilation syndrome, and sequelae of lung resection; or (3) neuromuscular diseases: muscular dystrophy, motor neuron disease, post-polio kyphoscoliosis, central hypoventilation, spinal cord damage, and phrenic nerve paralysis. Weaning was initiated as soon as the respiratory status was stabilized after admission, according to a previously described procedure.16
Weaning outcome was classified as follows: 1, success if patient survived and was liberated from PMV to self-ventilation; 2, partial success if patient survived and was liberated from PMV to noninvasive ventilation; 3, failure if PMV could not be discontinued. Subject care trajectories were described as follows: the referral source, (ie, home, ICU, or acute care hospital for cohort 1; local ICU or other hospital ICU for cohort 2). We recorded the number of days between the initiation of invasive ventilation and tracheostomy and between the tracheostomy and the transfer in our hospital in all the subjects of cohort 2 and in the 44 subjects referred from ICU of cohort 1; the length of stay (LOS) in our hospital (intermediate care facility LOS or RICU LOS); the total ventilator days during stays; the total ventilator days within 1 year and reconnection to the ventilator after an unsuccessful weaning attempt (%); the discharge destination (home, ICU or acute care hospital readmission, skilled nursing facility), and the in-hospital mortality. The survival 1 year after hospital admission was recorded. All the survivors or their closest relatives were contacted by telephone in March 2014 for cohort 1 (5 subjects [5.8%] were lost to follow-up) and in September 2018 for cohort 2 (4 subjects [3.9%] were lost to follow-up). The conduct of this non-interventional monocentric retrospective study was approved by the ethics committee of Bligny Hospital, and informed consent was obtained for all the subjects.
Statistical Analysis
Quantitative data are presented as a mean ± SD or a median (95% CI) if data were not normally distributed (D’Agostino Pearson test for normal distribution; P < .05). Categorical data are presented as a number (percentage). Interunit differences in subject characteristics and care trajectories were compared by using an analysis of variance or a Mann-Whitney U test for quantitative data, depending on the variable distribution and a chi-square test for categorical data. The Kaplan-Meier method was used to describe survival. The 1-year survival rate was calculated by setting the zero time on the day of admission in our hospital.
Differences in survival between the groups were assessed by using the log-rank test. A Cox proportional hazards regression was used to identify predictors of survival. A multivariate analysis was performed by using a forward-stepwise selection. For the analysis of demographics and survival, only the first hospital stay was investigated. Changes in LOS and 1-year survival days between the time before and after implementation of the RICU were evaluated by using Shewhart p-control charts.19 The control limits were set at ±3 SD from the mean. Statistical significance was set at P = .05. The statistical analysis was performed by using MedCalc Statistical Software version 18.11.6 (MedCalc Software bvba, Ostend, Belgium).
Results
Subject Characteristics
Cohort 1 included 66 consecutive subjects and cohort 2 included 103 consecutive subjects; their characteristics are shown in Table 1 and were computed according to the cohort. Lung and airway diseases (mainly pneumonia and/or ARDS) as a cause for chronic respiratory failure as well as a cardiovascular comorbidity were more often reported in cohort 2. The causes of the 16 deaths (24.2%) of the 66 subjects that occurred in cohort 1 were the following: respiratory failure, n = 9; aspiration pneumonia, n = 2; multi-organ failure, n = 2; barotrauma, and n = 2; massive hemoptysis, n = 1. The causes of the 10 deaths (9.7%) of the total 103 subjects that occurred in cohort 2 were the following: respiratory failure, n = 5; cardiac failure, n = 2; pneumonia, n = 1; pulmonary embolism, n = 1; massive hemorrhage, n = 1. Compared with cohort 1, the C-reactive protein and pH values were higher and the hematocrit and  values were lower in cohort 2.
values were lower in cohort 2.
Subject Demographics, Anthropometric, and Clinical Characteristics on Admission
Subject Care Pathways and Outcomes
The care pathways are shown in Figure 1. During the follow-up period, 23 of the 66 subjects (34.8%) in cohort 1 and 25 of the 103 subjects in cohort 2 (24.3%) (P = .14 between both cohorts) were readmitted at least once, so that, for cohorts 1 and 2, 109 (pre-RICU period) and 137 hospital stays (RICU period), respectively, were analyzed. The outcomes observed during the pre-RICU and RICU periods are shown in Table 2. The median LOS (P < .001) and total ventilator days during stays (P < .001) were significantly lower during the RICU period than during the pre-RICU period. The Shewhart p-control chart showed 2 versus 1 out-of-control markers of LOS before and after implementation of the RICU (Fig. 2).
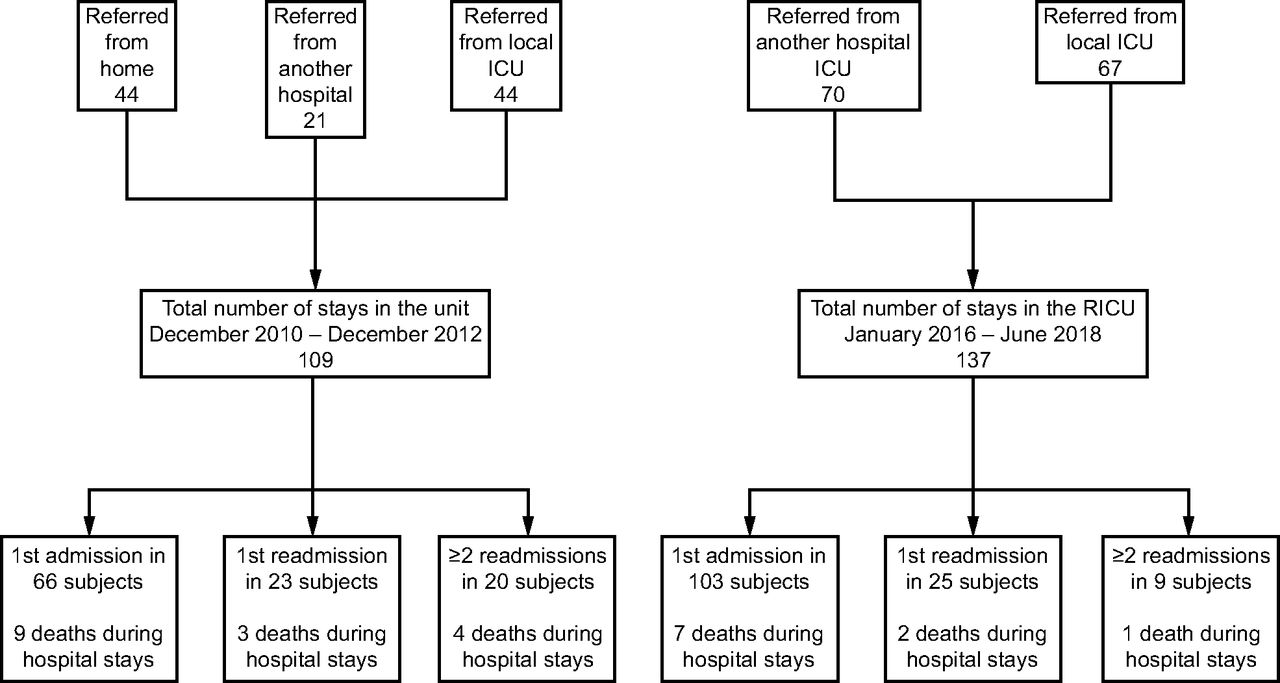
Flow chart.
Subject Outcomes During Hospital Stays

Shewhart p-control chart of the stay (A and B) and 1-year survival (C and D) according to the pre–respiratory ICU (RICU) (A and C) and RICU periods (B and D). Gray lines show mean, dotted lines denote SD, and dashed lines are upper and lower control limits (±3 SD). Violated runs according to Shewhart rules are indicated by red squares (large shifts above the upper control limit).
Discharge destinations were mainly home (71.6%) during the pre-RICU period or the ICU (29.9%) and skilled nursing facility (45.3%) during the RICU period (P < .001). During these periods, the occurrence of complications differed: fewer cases of respiratory sepsis and more cases of non-respiratory sepsis, and more cases of hypercapnic encephalopathy and pressure ulcers were observed during the RICU period than during the pre-RICU period. There was a trend toward higher C-reactive protein levels according to the origin of sepsis, either respiratory or non-respiratory: in cohort 1: 35.02 ± 7.77 mg/L versus 21.80 ± 7.04 mg/L, respectively; and in cohort 2: 51.23 ± 7.03 mg/L versus 39.40 ± 5.04 mg/L, respectively (P = .01 according to the cohort; P = .067 according to the origin of sepsis).
Survival Analysis
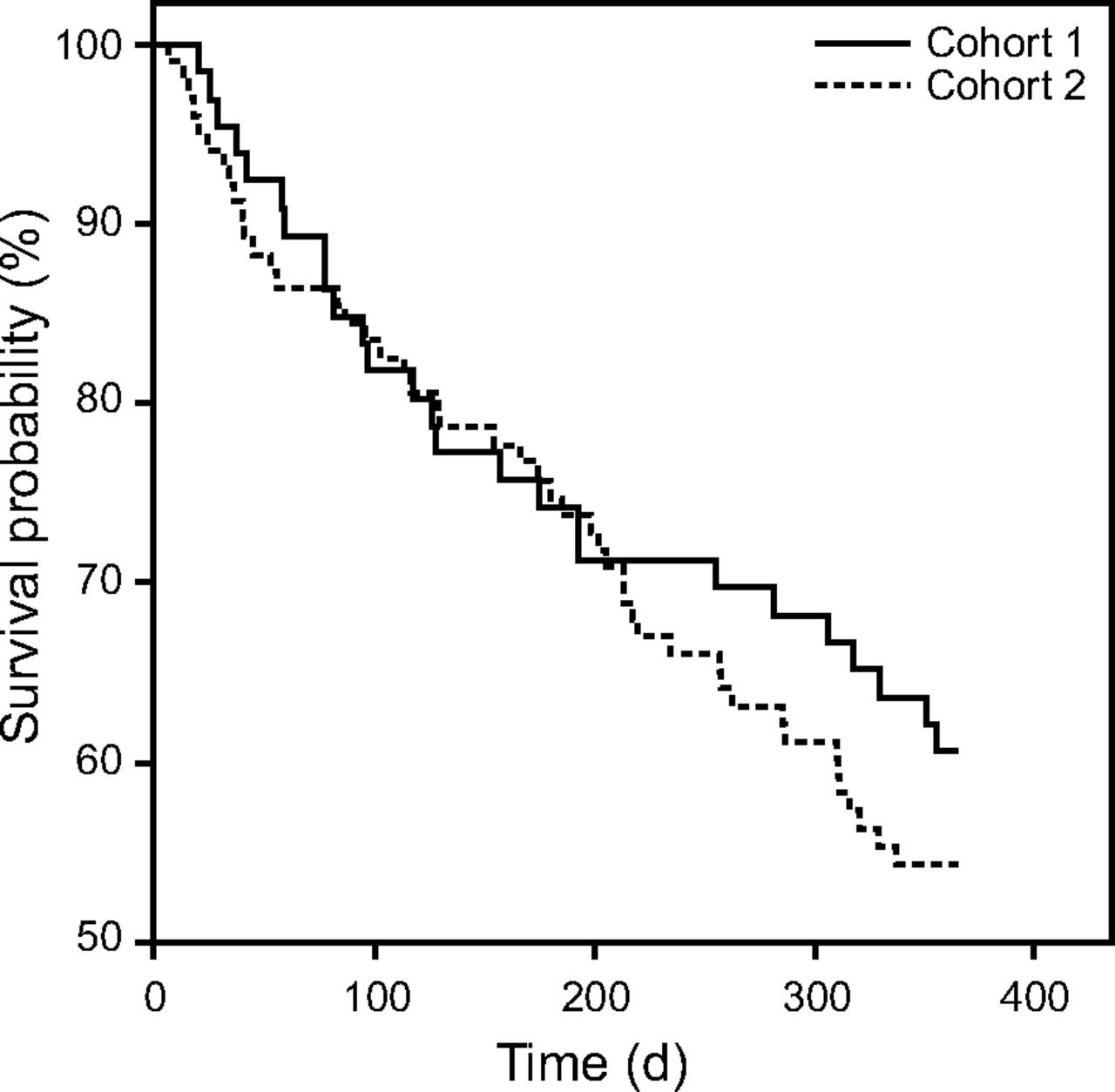
There was no statistical difference in 1-year survival between cohort 1 and cohort 2 (60.6% and 53.9%, respectively; P = .42). The Shewhart p-control chart showed no shift in the 1-year survival (days) after implementation of the RICU (Fig. 2). The Kaplan-Meier survival curve of the subjects according to this criterion is shown in Figure 3. The following predictors of 1-year survival were identified by a multivariate Cox regression analysis according to the variables shown in Table 1, which shows statistical differences between both cohorts: better outcomes were associated with the cause of chronic respiratory failure (subjects with neuromuscular disease had a longer survival, relative risk 1.57, 95% CI 1.19–2.08; P = .01) and if weaning was obtained at the time of hospital discharge (relative risk 0.50, 95% CI 0.31–0.80; P = .002); poorer outcomes were associated with a Charlson score > 5 (relative risk 2.41, 95% CI 1.50–3.89; P < .001). The following variables were not included in the model because of statistical insignificance: age ≥ 65 y, cardiovascular comorbidity, cohort, C-reactive protein, hematocrit,  , and pH.
, and pH.

Kaplan-Meier survival plot (in days) of subjects according to cohort. Cohort 1, 66 subjects included from December 2010 to December 2012; Cohort 2, 103 subjects included from January 2016 to June 2017.
Discussion
Results of this study showed that, in a community-based general hospital, the implementation of a RICU improved the in-hospital LOS and weaning success but did not change the 1-year mortality rate compared with the previous use of a specialized intermediate care facility in the same setting. Implementing RICUs in general hospitals has been found to reduce in-hospital mortality and LOS of subjects with acute respiratory diseases.20
The pathway of admission in a RICU is a major determinant of patient outcomes.21 It may be classified as follows: step-down pathway, which corresponds to an admission from an ICU; step-up pathway, which corresponds to an admission from a hospital ward; or direct pathway, which corresponds to an admission from the emergency department.22 These patterns differed in our hospital according to the pre-RICU period or RICU period in that the 3 previously described patterns were possible during the pre-RICU period, whereas the step-down pattern was the one authorized by the Regional Health Agency. Patients admitted in a RICU according to a step-up pattern usually have a poorer prognosis than those admitted according to the step-down pattern.22 This notion could explain the differences in subject characteristics observed in our 2 cohorts.
We also observed an important increase in the rate of activity devoted to the management of subjects who required PMV between our 2 cohorts: from 19% in our previously described unit16 to 68% in our RICU. This increase could be explained by the facilitation of discharge from acute care ICUs to an alternate care setting that was offered by the opening of our RICU.23 The time between the initiation of invasive mandatory ventilation and tracheostomy differed between cohorts 1 and 2: median 10 (95% CI 0–19) d versus median 21 (95% CI 16–23) d (P < .001). In cohort 1, this duration was in line with the data reported by Mehta et al,24 whereas the value observed in cohort 2 was much higher. Saiphoklang and Auttajaroon25 also recently found that this duration was high (24 ± 6 days, mean ± SD) in case of weaning difficulties in the subjects admitted to medical wards.
Despite similar Charlson scores between both cohorts, lung and airway diseases (mainly pneumonia and/or ARDS) as well as cardiovascular comorbidities were more often reported in cohort 2. The comparison of biologic data also showed that, compared with cohort 1, the C-reactive protein and pH were higher and the hematocrit and  were lower in cohort 2. In addition, the occurrence of complications during the pre-RICU and RICU periods differed: fewer cases of respiratory sepsis and more cases of non-respiratory sepsis as well as more cases of hypercapnic encephalopathy and pressure ulcers were observed in the RICU than in the pre-RICU period. In the subjects in whom infectious complications occurred, we found a trend toward higher C-reactive protein (CRP) levels according to the origin of sepsis, either respiratory or non-respiratory (P = .07). Vargas et al26 reported that 7 d after tracheostomy, the C-reactive protein level ranges between 10 mg/L and 30 mg/L, which was the case in cohort 1 but not in cohort 2.
were lower in cohort 2. In addition, the occurrence of complications during the pre-RICU and RICU periods differed: fewer cases of respiratory sepsis and more cases of non-respiratory sepsis as well as more cases of hypercapnic encephalopathy and pressure ulcers were observed in the RICU than in the pre-RICU period. In the subjects in whom infectious complications occurred, we found a trend toward higher C-reactive protein (CRP) levels according to the origin of sepsis, either respiratory or non-respiratory (P = .07). Vargas et al26 reported that 7 d after tracheostomy, the C-reactive protein level ranges between 10 mg/L and 30 mg/L, which was the case in cohort 1 but not in cohort 2.
Haja Mydin et al27 found that the C-reactive protein level and anemia were associated with increased in-hospital mortality. However, in the multivariate analysis, we did not find that the C-reactive protein level and the hematocrit were statistically significant predictors of 1-year survival. We observed differences in blood gases at the time of admission between both cohorts, and a lower number of subjects who were acidotic was found in cohort 2. This finding could be related to a lower proportion of subjects with rib cage abnormalities and neuromuscular diseases, which could induce severe acidotic hypoventilation.28 Analysis of these data could reflect changes in the profile of patients admitted for PMV management after an ICU stay, depending on whether a RICU is implemented.29
We found a significantly higher number of subjects who achieved a partial or complete weaning from PMV before and after implementation of the RICU (P < .001). The rate of 30.3% obtained during the 109 hospital stays that we found during the pre-RICU period16 was lower than in specialized weaning centers.30 Higher proportions of partial or complete weaning were obtained by specialized teams in patient populations that were probably not representative of units that were managing unselected subjects who were ventilator dependent because these units excluded subjects not likely to be weaned.30 Indeed, the rate of 69.3% of partial or complete weaning obtained during the 137 hospital stays over the RICU period was in line with the previously reported rate of 63% of subjects liberated from the ventilator in non-US countries.24
The 1-year mortality rate was not different between the pre-RICU and RICU periods in this study, that is, 60.6% and 53.9%, respectively. This finding was in line with the 1-year mortality rate of 59% reported in a recent systematic review and meta-analysis.24 However, our data were pooled from subjects who survive ICU originating from multiple hospital locations and cannot be duplicated for a specific ICU location. For example, Vargas et al31 found, in a prospective, single-center cohort study, that the 1-year survival after tracheostomy in the ICU was much lower (29.2%), and this could be due to the severity of the underlying condition of their subjects.
With regard to the predictors of survival, we found that better outcomes were associated with the cause of chronic respiratory failure (subjects with neuromuscular disease had a longer survival). Davies et al28 also found that subjects with neuromuscular disease experienced low mortality rates (4%). Weaning success at the time of hospital discharge has also been found to be associated with a longer survival by Engoren et al32 and, more recently, by Vitacca et al,33 who showed that subjects on ventilation had an 8.44-fold higher risk of mortality at 1 year than subjects who were not on ventilation. We confirmed our previous finding that a Charlson score > 5 is inversely correlated with the 1-year survival.16 The usefulness of this assessment has also been reported by Kojicic et al34 and, more recently, by Depuydt et al6 in subjects who were ventilator dependent.
As suggested by Damuth et al,35 efforts should now focus on multidimensional, subject-centered outcomes, including assessments of the quality of life, cognitive function, functional dependence, and caregiver burden. Given the scarcity of studies focused on these issues, especially in France and, notably, in non-academic settings, we recognized the lack of such data in our study and that these priorities should now be taken into account in future studies in the specialty. Indeed, these assessments are difficult to implement, because it is difficult to record information from psychological and quality-of-life assessments6,31 and because of information communication issues between physicians and patients and their family.36
Our study had some limitations. First, it had a retrospective design, with all associated methodological issues for data assessment. Second, subject data were recorded in a single institution, and the comparison between values reported for different care settings in patients with PMV is complicated by highly variable definitions and care delivery methods in RICUs.37 As previously indicated, we did not assess subjects’ functional status and quality of life, although these factors have been shown to be severely impaired in patients undergoing PMV.9 Also, we did not perform a cost analysis, although costs remain an important issue to be taken into account in the decision of implementing RICUs. The fact that the French institutional decisions concerning the implementation of RICUs are recent should not delay thorough studies on this point, which remains controversial.21
Conclusions
This study showed that the opening of a RICU to replace our previously described intermediate care facility improved the outcomes of subjects with tracheostomy and with PMV by reducing the LOS and by increasing the rate of complete or partial weaning. However, subjects’ 1-year survival remained unchanged, probably because of possible changes in the profile of subjects admitted for PMV management after an ICU stay related to changes in their step-down pathway.
ACKNOWLEDGMENTS
The author thanks Christian Darné MD, Françoise Haniez MD, Hélène Jaillet MD, C Karanfilovic MD, Henri Maas MD, for their assistance with data collection.
Footnotes
- Correspondence: Bertrand Herer MD, Centre Hospitalier de Bligny, F-91640 Briis-Sous-Forges, France. E-mail: b.herer{at}chbligny.fr
Dr Herer has no conflicts to disclose.
- Copyright © 2020 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}