

Abstract
BACKGROUND: We sought to evaluate the acute effects of different inspiratory loads using nasal and oral interfaces on the volumes of the chest wall and its compartments, breathing pattern, and respiratory muscle activation in children with mouth-breathing syndrome.
METHODS: Children with mouth-breathing syndrome were randomized into 2 groups, one with an inspiratory load intensity 20% of maximum inspiratory pressure (n = 14), and the other with an inspiratory load intensity 40% of maximum inspiratory pressure (n = 15). The chest wall volumes and electromyography of sternocleidomastoid, rectus abdominis, scalene, and internal intercostal muscles were used to analyze respiration against the 2 load intensities and using 2 interfaces (ie, nasal and oral).
RESULTS: A total of 72 children with mouth-breathing syndrome were recruited, and 29 were evaluated in this study. The use of inspiratory load promoted improvement in the components of the breathing pattern: breathing frequency (P = .039), inspiratory time (P = .03), and total respiratory time (P = .043); and increases in tidal volume (P < .001), end-inspiratory volume (P < .001), and electrical activity of scalene muscles and sternocleidomastoid muscles (P < .001) when compared to quiet breathing. The load imposed via a nasal interface versus an oral interface provided an increase in tidal volume (P = .030), end-inspiratory volume (P = .02), and electrical activity of scalene muscles (P < .001) and sternocleidomastoid muscles (P = .02).
CONCLUSIONS: The use of acute inspiratory loads improved the breathing pattern and increased lung volume and electrical activity of inspiratory muscles. This work brings new perspective to the investigation of using nasal interfaces during the application of inspiratory loads. The nasal interface was more effective compared to the oral interface commonly used in clinical practice.
Introduction
Oral breathing is characterized by a shift in the physiological mode of exclusively nasal breathing to oral or mixed breathing for a period of > 6 months.1,2 It is more common in childhood and, due to its various causes, is classified as mouth-breathing syndrome (MBS)3. The main factors responsible for the development of MBS are genetic, biochemical, immunological, and physiological and may lead to modifications in several systems such as stomatognathic, musculoskeletal, and respiratory.2,4,5
Oral breathing generates a change in the positioning of the tongue, which may negatively influence the position and direction of the mandible growth, and can cause oral and perioral muscle imbalances as well as postural disorders.5–8 These modifications influence the spatial positioning of the posterior muscle chains of the spine. This contributes to the increase of thoracic kyphosis and compromises the volume generation of the chest wall.9 Additionally, the postural disorder may negatively influence the contraction of the diaphragm and abdominal muscles, thus impacting their synergism. This leads to a reduction of muscular effort, chest wall expansion, and respiratory muscle weakness.1,2
The act of breathing is a vital process that occurs normally via the nose, with the objective to filter, moisten, and warm the inspired air. Despite this, respiratory resistance devices available in the market only use mouthpieces (oral airway) rather than a nasal interface. According to Held et al,10 respiratory muscle training using nasal breathing in MBS children lead to an increase in respiratory muscle strength and nasal respiratory flow. However, this study used a simplistic methodology in which the effects of training on respiratory muscle strength were verified by measuring only maximal inspiratory pressures. This prevented the muscles from being assessed individually.
The respiratory repercussions resulting from MBS in children have been previously reported. However, little is known about the interventions focusing on respiratory therapy for this syndrome. This study aimed to clarify the implications of using inspiratory loads in MBS children via the nasal airway. Therefore, we evaluated the acute effects of inspiratory loads imposed using different interfaces (ie, nasal and oral) on the volumes of the chest wall and its compartments, breathing pattern, and respiratory muscle activity using optoelectronic plethysmography and surface electromyography, respectively.
QUICK LOOK
Current Knowledge
The benefits of the use of inspiratory loads have been observed in several studies among healthy subjects and subjects with inefficient respiratory function, using an oral interface. It has been suggested that children with mouth-breathing syndrome have differentiated posture (eg, anteriority of the head), respiratory muscle weakness, and reduced lung volume. The ability of nasal interfaces to perform inspiratory muscle training, as well as its use as therapy in children with mouth-breathing syndrome, has not been studied.
What This Paper Contributes to Our Knowledge
The immediate application of inspiratory loads was able to favor chest wall volumes, breathing pattern, and respiratory muscle activity in children with mouth-breathing syndrome. These findings were more effective when using the nasal interface.
Methods
Type of Study and Subjects
We performed a cross-sectional, observational, analytical study that followed the CONSORT precepts. The project was approved by the Research Ethics Committee of Hospital Universitário Onofre Lopes (1.251.451/2015). Subjects' legal guardians signed a consent form drafted according to the Helsinki Declaration.
We recruited children with a diagnosis of MBS who visited the Otorhinolaryngology Out-patient Clinic of the Onofre Lopes University Hospital/Brazilian Hospital Services Company, Natal, Brazil. Selected subjects were of both genders, with ages ranging from 6 to 13 y, body mass index classified according to the World Health Organization normality standard,11 and an FEV1/FVC > 80% of predicted.12 Subjects who failed to perform the tests or voluntarily removed themselves from the study were excluded (Fig. 1).
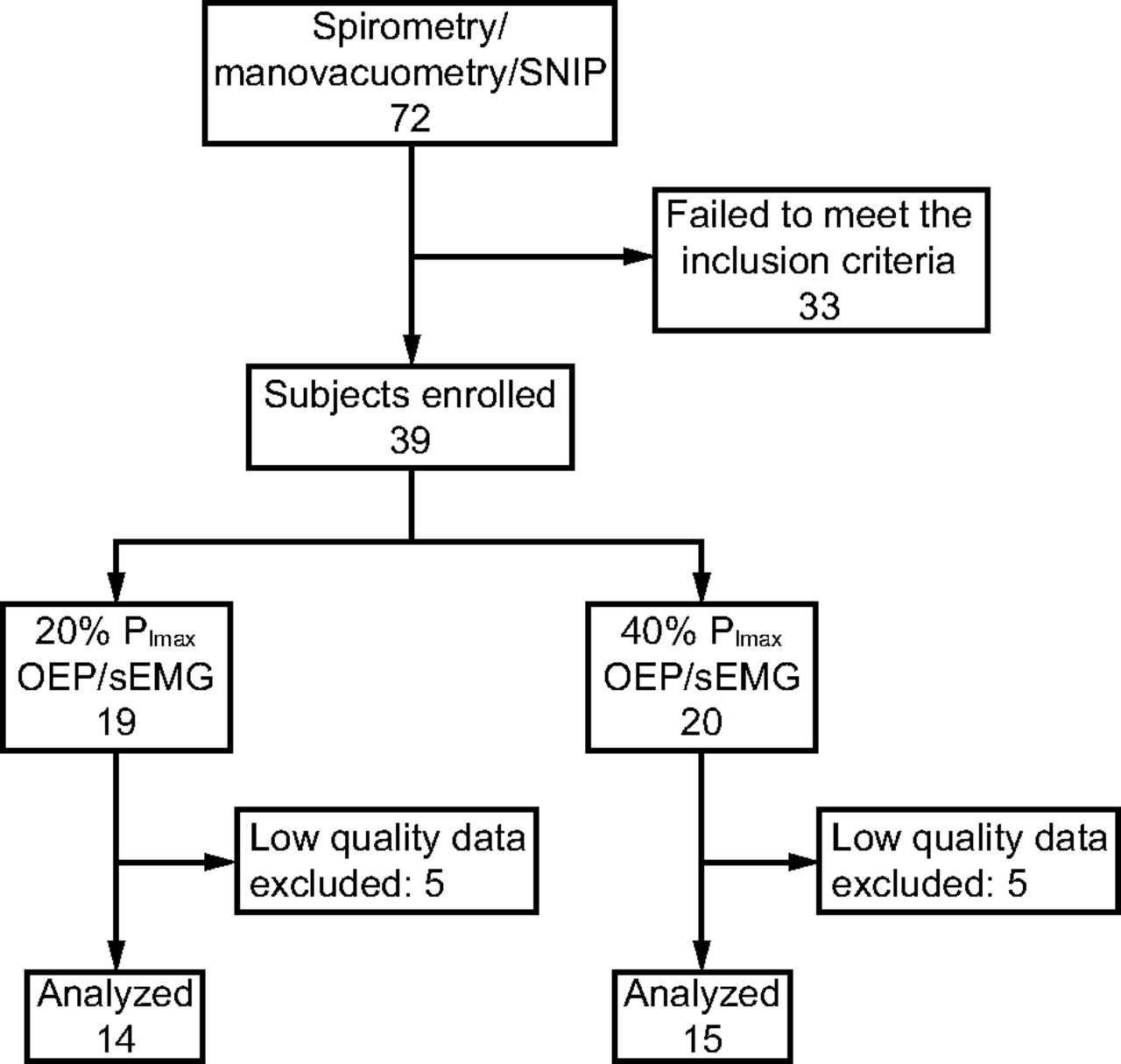
Flow chart of study design. SNIP = sniff nasal inspiratory pressure; PImax = maximum inspiratory pressure; OEP = optoelectronic plethysmography; sEMG = surface electromyography.
Pulmonary Function and Respiratory Muscle Strength
Spirometry was performed using the KoKo DigiDoser spirometer (nSpire Health, Longmont, Colorado). The evaluations were performed according to the criteria of acceptability and reproducibility of the American Thoracic Society/European Respiratory Society (ATS/ERS),13 and the reference values were derived according to the recommendations of the Brazilian Guidelines for pulmonary function testing.12
Respiratory muscle strength was measured in terms of maximum inspiratory pressure (PImax), maximum expiratory pressure (PEmax), and sniff nasal inspiratory pressure (SNIP) using a digital manometer (NEPEB-LabCare/UFMG, Belo Horizonte, Brazil). The evaluations were performed according to the acceptability and reproducibility criteria of the ATS/ERS.13 Reference values previously published by Lanza et al14 were used for PImax and PEmax, whereas the reference values of Stefanutti and Fitting15 were used for SNIP.
Chest Wall and Compartmental Volumes
The evaluation of the volumes of the chest wall and its compartments (ie, pulmonary rib cage, abdominal rib cage, and abdomen) was performed with optoelectronic plethysmography (BTS, Milan, Italy) in which volumes were obtained following an experimental model according to the Gauss theorem.16 Before each data acquisition, the equipment was calibrated at a frequency of 60 Hz. Six photosensitive cameras positioned around the subject (3 in the anterior region and 3 in the posterior region) captured the movement variation of 89 reflexive markers fixed at specific points of the thorax and abdomen of the subjects.17
From optoelectronic plethysmography data, the following variables were analyzed for the chest wall and its compartments: tidal volume (VT) in the chest wall, the pulmonary rib cage, the abdominal rib cage, and the abdomen; end-inspiratory volume in the chest wall, the pulmonary rib cage, the abdominal rib cage, and the abdomen; end-expiratory volume in the chest wall, the pulmonary rib cage, the abdominal rib cage, and the abdomen; as well as breathing frequency, inspiratory time; expiratory time, and total time of respiratory cycle.
Surface Electromyographic Activity
Surface electromyography was performed following the recommendations of the International Society of Electrophysiology and Kinesiology.18 Myoelectric signals were recorded using the electromyographic TeleMyo DTS Desk Receiver (Noraxon, Scottsdale, Arizona) and 4 wireless Clinical DTS sensors (Noraxon) with a 20–500 Hz pass filter-band, 1,000 gain, 16-bit resolution, and a common mode rejection rate > 120 dB.
Signals were obtained using double hall Ag/AgCl passive surface self-adhesive electrodes (Miotec, Porto Alegre, Brazil). The electrodes were placed on the following muscles: scalene muscles (at 5 cm from the sternum-clavicular joint and 2 cm above this point),19 sternocleidomastoid muscles (in the lower third of the distance between the mastoid process and the sternum-clavicular joint),20 rectus abdominis muscles (at 4 cm from the umbilical scar), and intercostal muscles (over the second intercostal space and 3 cm from the sternum).21 All electrodes were positioned on the right side of the body to minimize cardiac noise interference. Before placing the electrodes, the skin region was trichotomized and cleaned with alcohol to reduce the impedance to capture the electrical signal. Data acquisition and analysis were performed using MR 3.2 software (Noraxon). Raw data were analyzed by means of root mean squares (RMS) and standardized from respiratory baseline values.22
Inspiratory Load
An electronic variable flow resistance training device (POWERBreathe K5, International, Warwickshire, United Kingdom) was used to assess the acute effects of different inspiratory loads and different interfaces. The POWERBreathe is an electronically controlled, variable flow resistance device generally used for inspiratory muscle training. At first, an absolute initial load was assigned and successively reduced depending on the inspiratory flow generated by the subject. The POWERBreath device was used simultaneously with the surface electromyography and optoelectronic plethysmography data acquisition.
Randomization and Study Design
The sample was randomized and allocated into 2 groups by way of a simple draw. Subjects were grouped according to the intensity of load applied, either 20% or 40% of the maximum inspiratory pressure (PImax). Assessments were carried out in 2 stages, with no more than 20 d between assessments: in stage 1, clinical, spirometric and respiratory muscle strength evaluation occurred; in stage 2, assessment of chest wall volumes and respiratory muscles activity during inspiratory load occurred. During stage 2, the assessment consisted of 3 steps, each lasting 30 s: quiet spontaneous breathing, breathing against inspiratory load (ie, load), and recovery.
The protocol consisted of applying 2 load intensities (ie, 20% and 40% of PImax) using 2 different interfaces (ie, oral and nasal) in both groups; the order of these steps was randomized with the same process. The POWERBreathe was used as the resistive valve (Fig. 2A). For the nasal interface, a patented device (PI 0164278 – INPI) consisting of an orofacial mask connected to the resistive valve was used (Fig. 2B). During the assessment, subjects were asked to breath exclusively through the nose.

A: POWERBreathe K5, and B: a device consisting of an orofacial mask connected to the resistive valve; patented as a utility model (PI 0164278, INPI).
Sample Size and Statistical Analysis
Sample size was established considering the VT as the main variable. Five subjects of each group (total of 10 subjects) were evaluated using hypothetical one-way analysis of variance during all 3 steps. A sample size medium of 11 subjects for each group was estimated using and alpha error of 0.05 with bilateral distribution and test power of 80%.
Data normality was verified with the Shapiro-Wilk test. The Mann-Whitney test was used to analyze differences between the 20% PImax and 40% PImax groups. Differences between the quiet spontaneous breathing, load, and recovery steps were analyzed using the Friedman test, and in case of a significant difference, the Dunn post hoc test was applied. Comparisons between the oral and nasal interfaces were performed using the Wilcoxon test.
For data analysis, GraphPad Prism 6.0 (GraphPad Software, San Diego) was used. The sample size calculation, power (β), and effect size of the study were calculated with GPower 3.1.9.2 (University of Düsseldorf, Kiel, Germany). Cohen's dz for intergroup analysis was used to calculate the effect size between the 20% PImax group and the 40% PImax group, and partial eta for intergroup analysis was used to calculate the effect size between steps.23 For all statistical analyzes, a significance level of P < .05 with bilateral distribution was adopted.
Results
A total of 72 patients were recruited, of whom 33 did not meet the inclusion criteria. Ten children were excluded due to the low quality of data acquisition, resulting in a final sample of 29 subjects who were randomized and allocated into 2 groups: 14 children in the 20% PImax group and 15 children in the 40% PImax group (Fig. 1). No significant differences were observed between groups regarding anthropometric, pulmonary function, and respiratory muscle strength data. PImax, PEmax, and SNIP values were reduced compared to predicted values (Table 1).14,15
Anthropometric, Pulmonary Function and Respiratory Muscle Strength Characteristics of Both Groups
Chest Wall and Compartmental Volumes
As shown in Figure 3A, regardless of the imposed load and interface used, significant increases of VT in the chest wall were observed during the load step compared to the quiet spontaneous breathing and recovery steps (P < .001). These changes occurred in the rib cage compartments (ie, pulmonary rib cage and abdominal rib cage) in the 20% PImax group and in all compartments in the 40% PImax group. VT in the chest wall was higher when using the nasal interface compared to the oral interface during the quiet spontaneous breathing step (20% PImax: P = .028; 40% PImax: P = .036) and the load step (P = .030 for the 20% PImax group and the 40% PImax group). No statistical differences were observed between inspiratory load intensities.
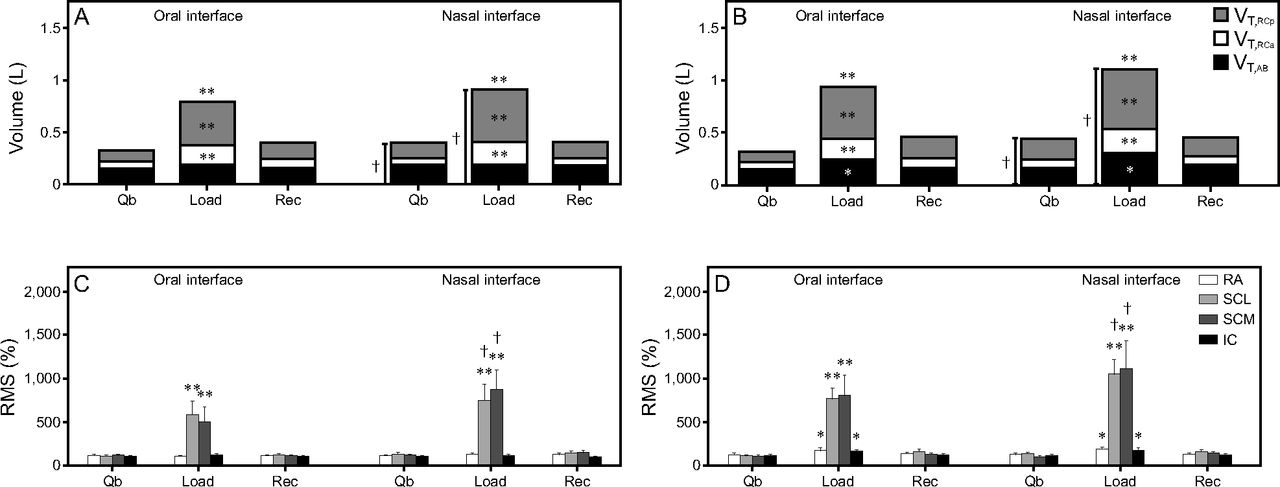
(A) and (B) Effects of different loads and respiratory interfaces on the tidal volume of the chest wall and its compartments (VT,Rcp = pulmonary rib cage; VT,Rca = abdominal rib cage; and VT,AB = abdominal). (A) 20%PImax group and (B) 40%PImax group. (C) and (D) Respiratory muscles root mean square (RMS) normalized values (RA = rectus abdominis; SCL = scalene; SCM = sternocleidomastoid; IC = intercostal). Microvolt values were normalized and are shown as mean percentage of RMS. (C) 20%PImax group and (D) 40%PImax group.
Regarding the operational volumes, a significantly higher end-inspiratory volume in chest wall (P < .001 regardless of load intensity and interface used) was observed during the load step compared to the quiet spontaneous breathing and recovery steps. The pulmonary rib cage and abdominal rib cage compartments were the main determinants for this increase. In addition, a significant decrease in the end-expiratory volume of the abdomen (oral interface: P = .047; nasal interface: P = .02) was observed when the 40% load was imposed. In both groups, significant increases in end-inspiratory volume in chest wall were observed with the use of nasal and oral interfaces (20% PImax: P = .01; 40% PImax: P = .02) (Fig. 4).
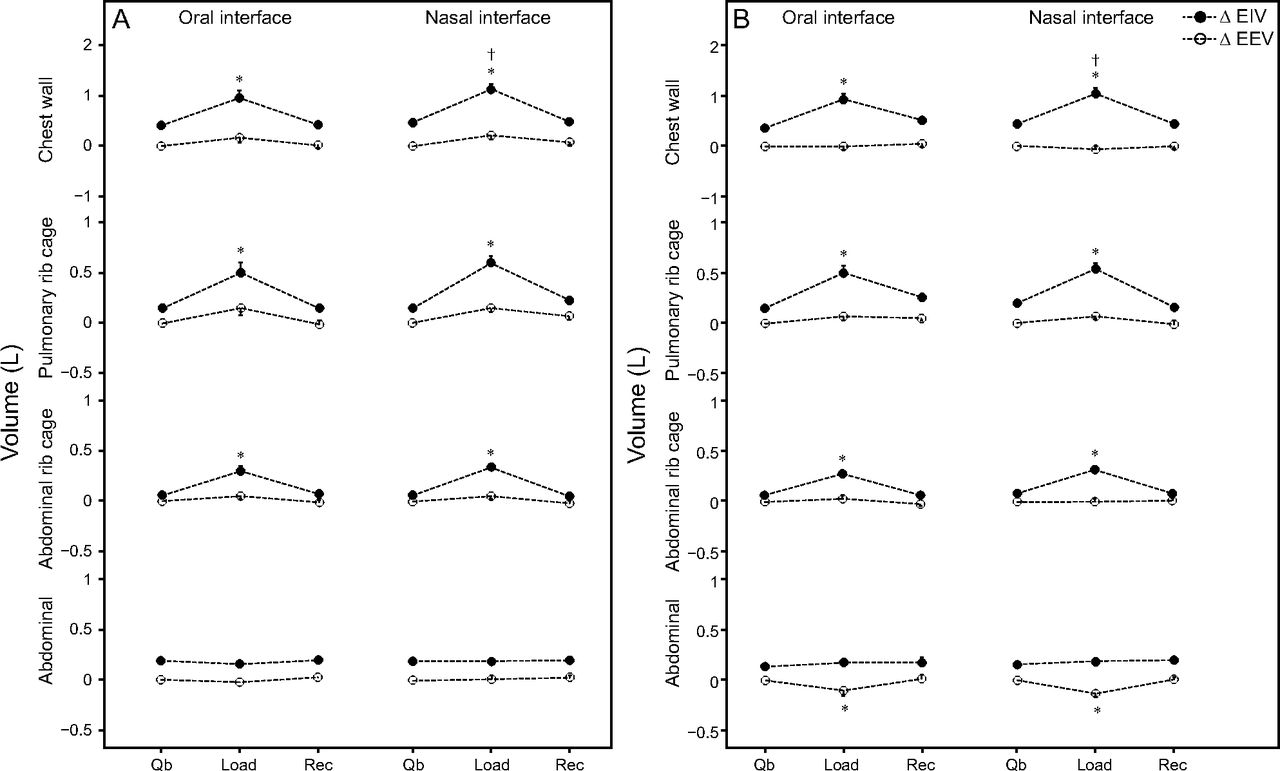
A: 20% PImax group and B: 40% PImax group. Data are shown as mean (standard error of the mean) for operational chest wall and compartmental volume variations during quiet spontaneous breathing (Qb), load, and recovery (Rec) moments. * P < .05 (Friedman test with Dunn post hoc analysis was used for comparisons between different moments: Qb vs Load and Rec). † P < 0.05 (Wilcoxon test was used for intragroup comparisons: oral interface vs nasal interface). ΔEIV = end-inspiratory volume variation; ΔEEV = end-expiratory volume variation.
When comparing the breathing pattern during the load step, we observed a significant increase in inspiratory time (20% PImax: oral and nasal interface, P < .001; 40% PImax: oral interface, P = .03, nasal interface, P = .01) and subsequently in total time of the respiratory cycle (20% PImax: oral and nasal interface, P < .001; 40% PImax: oral interface, P = .043, nasal interface, P = .03), as well as a decrease in breathing frequency (20% PImax: oral interface, P < .001, nasal interface, P = .02; 40% PImax: oral interface, P = .02, nasal interface, P = .039). During the recovery step, inspiratory time, total time of the respiratory cycle, and breathing frequency returned to baseline values. No significant changes were observed in expiratory time when comparing interfaces and inspiratory load intensities (Table 2).
Breathing Pattern of Both Groups During Quiet Spontaneous Breathing, Load, and Recovery Steps
Surface Electrical Activity of Respiratory Muscles
The signals obtained from surface electromyography were normalized, and their representation are shown in Figure 3B. During breathing against both inspiratory loads, %RMS of sternocleidomastoid and scalene muscles increased in relation to the quiet spontaneous breathing and recovery steps (P < .001 for 20% PImax and 40% PImax groups with oral and nasal interfaces); however, the intercostal and rectus abdominis muscles only showed this activity with the intensity of 40% of PImax load (intercostal: oral interface, P = .001, nasal interface, P = .02; rectus abdominis: oral and nasal interface, P = .001). The comparison between interfaces revealed greater values of muscle electrical activity for the scalene muscles (P < .001 for 20% PImax and 40% PImax groups) and sternocleidomastoid muscles (20% PImax: P = .007 and 40% PImax: P = .02) when using the nasal interface during the imposition of both inspiratory loads. Comparing the load step when using the nasal and oral interfaces, %RMS of the scalene muscles was increased (P = .039) when 40% of PImax load was imposed via the nasal airway (P value not shown in Fig. 3B).
Power and Effect Size
Table 3 summarizes the effect sizes and power test for VT in the chest wall, end-inspiratory volume in chest wall, end-expiratory volume in the chest wall, and the %RMS of sternocleidomastoid and scalene muscle activation during the comparison of the quiet spontaneous breathing, load, and recovery steps. It also shows the comparison between nasal and oral interfaces.
Effect Size and Power of the Comparisons Between Steps and Interfaces
Discussion
The objective of this study was to evaluate the acute responses of different inspiratory loads, using nasal and oral interfaces, on the volumes of the chest wall and its compartments, as well as breathing pattern and respiratory muscle activation, in children with mouth-breathing syndrome. The use of inspiratory loads promoted an increase in chest wall volumes, and these changes were more evident with the nasal interface. These changes were also accompanied by increased inspiratory muscle activity, mainly of the scalene and sternocleidomastoid muscles.
It was possible to confirm that children with MBS present with reduced respiratory muscle strength compared to their predicted values.14 Despite the absence of clinical evidence about respiratory muscle strength in this population,24 Okuro et al1 corroborated our findings in reporting reductions in PImax and PEmax in children with MBS compared to nose-breathing children. These authors also associated these results with respiratory dynamics disorganization (ie, inefficient contraction of the diaphragm and the abdominal muscles, due to a postural disorder and reduction of nasal reflexes). In addition, we also observed a reduction in SNIP ‘in our’ subjects; no previous scientific evidence about the evaluation of this variable was found. Milanesi et al25 evaluated adults who had clinical diagnosis of MBS during childhood and observed a reduction in maximum respiratory pressures and functional capacity when compared to healthy adults. This observation demonstrated that the repercussions of this syndrome may remain during adult life if not corrected in childhood.
No changes were observed in the spirometric values of our sample; however, a literature review carried out by Veron et al26 contrasts our findings by suggesting that disorders resulting from oral breathing contributes to muscle imbalance and poorer lung function. In another study, Trevisan et al27 reported that mouth-breathing adults exhibit a reduction in diaphragmatic amplitude compared to nose-breathing adults, a result that is consistent with pulmonary restriction.
The inspiratory loads imposed via the nasal interface were more effective in increasing VT in the chest wall compared to the oral interface. This response was also evidenced during the quiet spontaneous breathing moment. This indicates that the use of a nasal interface in children with MBS, even in the absence of inspiratory load, promotes an increase in chest wall volume, most likely due to the anatomical higher resistance in the nasal airway.28–30 However, during the imposition of inspiratory loads, chest wall VT increased due to the combined contributions of the chest wall compartments. For 20% of PImax, only the rib cage compartments (ie, pulmonary rib cage and abdominal rib cage) were involved, whereas, for 40% of PImax, the pulmonary rib cage, abdominal rib cage, and abdominal compartments were involved. Because VT is a result of the variation between end-inspiratory volume and end-expiratory volume in the chest wall,31 we may infer 3 conclusions about the mechanisms behind the use of inspiratory loads in children with MBS. First, the primary responses to increased inspiratory load are the activation of inspiratory muscles and recruitment of the rib cage compartments (ie, increase in end-inspiratory volume in pulmonary rib cage and end-inspiratory volume in abdominal rib cage), which is more pronounced when using a nasal interface. Second, with the increase in inspiratory load (from 20% to 40%), VT is increased due to the activation of rectus abdominis muscles, which leads to a decrease in end-expiratory volume in the abdomen. Third, no significant increases in end-expiratory volume in the chest wall were observed, indicating that the imposition of inspiratory loads does not cause hyperinflation.
The breathing pattern became more efficient in response to the use of inspiratory load, showing increases in VT, total time of respiratory cycle, and inspiratory time, as well as a reduction in breathing frequency. A previous study that aimed to characterize the breathing pattern and the thoracoabdominal movement of children at rest through respiratory induction plethysmography reported results similar to ours when observing the volume variation and breathing pattern of children with MBS compared to nose-breathing children.32 Another study, conducted in healthy adults and using optoelectronic plethysmography, also corroborates our findings with similar increases in chest wall VT (due to VT increases in the pulmonary rib cage and in the abdominal rib cage), inspiratory time, and total time of the respiratory cycle in response to the use of inspiratory loads, which ranged from 0 to 40 cm H2O).33 We correlate the increase in inspiratory time to a greater time for lung filling, which also increases the end-inspiratory volume. We found association between the maintenance of the expiratory time to the absence of ventilatory repercussions, thus avoiding the increase of the end-expiratory volume and not causing dynamic hyperinflation. Lastly, we associate a breathing frequency reduction to the increase in the total time of the respiratory cycle.
No studies have been found in the literature regarding the assessment of electrical activity of respiratory muscles during the use of resistive inspiratory load in children with MBS, thus precluding the possibility of comparing our data to data derived from a similar population. Our results indicate that the scalene and sternocleidomastoid muscles substantially increase their activity when exposed to inspiratory loads, accompanying the increase in volume variation of the chest wall and its compartments. This increase did not show any difference between the groups; however, the load imposed via the nasal interface showed significantly greater activity when compared to the oral interface, which suggests that the former may be more effective for treatments targeting inspiratory muscle activation. Results reported by Held et al10 align with our results, indicating that a protocol of respiratory muscle training and nasal breathing performed in children with MBS improved respiratory muscle strength and nasal inspiratory flow. Held et al10 revealed the importance of nasal respiratory training for the reestablishment of lung volume and the elasticity of the nostrils in the studied subjects. Increases in electrical activity of the intercostal and rectus abdominis muscles were observed only when the load of 40% was set. This suggests that, in response to the increase of inspiratory load, the recruitment of the intercostal increases the force generation on the rib cage, optimizes diaphragmatic length,34 and improves respiratory synergy,35 Simultaneously, the rectus abdominis minimizes rib cage distortion, regulates ventilatory response, and places the diaphragm muscle in an improved mechanical advantage to assist subsequent inspiration.36
Moreover, Yokoba et al37 evaluated the behavior of the scalene, sternocleidomastoid, transverse abdominal, and trapezius muscles during high-intensity loads. They reported that the scalene muscle is recruited first, followed by a progressive increase of the sternocleidomastoid muscle, and finally the trapezius muscle is recruited. Thus, we hypothesize that the resistance of 20% PImax would already be sufficient to promote recruitment of the scalene and sternocleidomastoid muscles, whereas the intercostal muscle only increases its activity in response to higher loads (eg, 40% of PImax). This is likely due to the need to increase muscle recruitment and generate more effort to overcome the higher imposed resistance.
Because MBS is a complex syndrome and a large number of patients did not meet the inclusion criteria, this study has some limitations. First, we did not include nose-breathing children to be directly compared to the children with MBS. Second, due to the short evaluation period and study design, it was not possible to measure information such as ventilation and work of breathing. Another possible limitation is that the optoelectronic plethysmography technique, although widely validated in studies with healthy and pathological subjects, is not yet widespread in clinical practice. The great advantage of optoelectronic plethysmography, however, is that accurate measurements of the volumes of the chest wall and its compartments can be obtained noninvasively and with nonvolitional tests. Despite these limitations, our results add new perspectives regarding the use of inspiratory loads, as well as new aspects related to its application via nasal interfaces. Longitudinal studies must be performed to identify the long-term effects on ventilation and respiratory muscle strength.
Conclusions
The results of our study indicate a better efficiency in applying inspiratory loads using the nasal interface compared to the oral interface to increase inspiratory muscle activity and the volume of the chest wall and its compartments. Furthermore, these results were observed regardless of the load applied, indicating that an inspiratory load of 20% PImax would be sufficient to reach a specific therapeutic goal by generating an increase in lung volume, which may act as a protective factor for respiratory tract infections.
Footnotes
- Correspondence: Guilherme Augusto de Freitas Fregonezi PhD, PneumoCardioVascular Lab Departamento de Fisioterapia, Universidade Federal do Rio Grande do Norte, Campus Universitário, Caixa-postal 1524, Lagoa Nova, CEP 59072970, Natal, RN, Brazil. E-mail: fregonezi.guilherme{at}gmail.com
The study received financial support from the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), PGCI CAPES 054/2014 - 23038.007514/2014-78 and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) process: 400316/2012-9. Guilherme Augusto de Freitas Fregonezi received a grant from CNPq number 312876/2018-1, and Vanessa Resqueti received a grant from CNPq number 315580/2018-6.
- Copyright © 2020 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}
{kind=link}