

Abstract
BACKGROUND: Although guidelines for inhaled therapies for individuals with cystic fibrosis (CF) are available, recommendations for compressors/nebulizers to optimize care are lacking. The CF Foundation (CFF) convened a multidisciplinary task force to assess the use, durability, accessibility, and cost burden of compressors/nebulizers.
METHODS: Online surveys were developed and distributed to 287 CFF programs and adults with CF and parents of children with CF (adults with CF/parents).
RESULTS: Health care providers from 38 states completed the survey (59% response rate). Respiratory therapists were mostly responsible to coordinate ordering nebulizers and compressors. Durable medical equipment companies were the most common source of acquisition of compressors (71.8%) and nebulizers (45.9%). A majority of health care providers did not feel the compressors were durable (51.1%) or that they could get enough nebulizers to their patients (69.2%). Barriers to procure compressors were reported. The survey was completed by 734 adults with CF/parents from 48 states. Most adults with CF/parents rated their compressor as durable (65.8%); however, 85.5% of respondents reported some user-experience problem(s). “Hoses popping off” and “increased nebulization time” were most commonly reported. Almost 20% of respondents did not have access to a compressor at some point in the previous year. Most adults with CF/parents did not change compressor filters per manufacturer’s recommendation (40% never). Adults with CF/parents reported performing a median of 4 inhaled treatments per day. Median use of nebulizers was 6 months. Most adults with CF/parents thought they had enough nebulizers (53.7%). Individuals with CF doing more inhaled treatments reported more compressor malfunctions. The median out-of-pocket expense was $75–99 and $50–74 for compressors and nebulizers, respectively.
CONCLUSIONS: Although the perceptions of health care providers and adults with CF/parents differed to a certain extent, the surveys uncovered several significant issues that may compromise quality of care. Improvement in access to devices and education are needed.
Introduction
Cystic fibrosis (CF) is a genetic multi-organ disease caused by absence or malfunction of the CF transmembrane regulator protein.1 This results in several pulmonary problems: dehydration of the airway surface liquid of airway cells, abnormal clearance of pulmonary secretions, and frequent pulmonary infections. Clinical practice guidelines developed by the CF Foundation (CFF) recommend the use of several inhaled medications (eg, mucolytics and airway hydrators for mucus thinning and antibiotics for eradication and chronic suppression of bacteria in the airway to prevent, treat, and delay progression of the disease).2-3 These inhaled medications when coupled with airway clearance techniques are a primary and critical component in slowing the progression of CF lung disease. These treatments are given 1–4 times per day, thus increasing the burden of care of individuals with CF. Some of these medications cannot be administered in the same nebulizer cup due to potential loss of biological activity. This results in the need for several nebulizers per day to be able to complete therapies as well as the required cleaning and disinfection. Also, some drugs such as dornase alfa and inhaled tobramycin have been approved as a drug-device combination, therefore requiring a specific nebulizer and compressor to be used.4
The most common types of nebulizers used by individuals with CF are jet (continuous output and breath enhanced) and vibrating mesh.5 The latter requires special care of the mesh membrane. If not cleaned and disinfected properly, clogging of the pores and malfunctioning may occur.6 These devices are self-contained, expensive, and available as drug-device formulation or as open source. Jet nebulizers are significantly less expensive, require a gas source (ie, a compressor for home use), and are available as disposable or reusable units. The daily inhaled medication routine for individuals with CF can add up to 2 h per day or more, thus reducing the useful life of the compressor.7-8 Awad et al8 reported that nebulizer performance deteriorated over time when used with similar frequency as with individuals with CF. The same group reported that substituting the nebulizer recommended for a specific compressor resulted in changes of the characteristics of the released aerosol.9 This could result in changes in distribution of lung deposition.5 Moreover, several studies reported that compressors have different output flows and pressures, thus releasing aerosols of different characterisitics.8,10 The repeated cleaning and disinfection of nebulizers could affect their performance.11-12 These studies demonstrate the importance of having durable and reliable nebulizers and compressors to deliver inhaled medications to individuals with CF.
Although CF care in the United States is standardized through accreditation of care centers and use of care guidelines, regional and insurance variance in outcome have been reported.13 Individuals with CF with state-funded insurance experienced worse outcomes than those with private insurance.13 Lester et al14 surveyed individuals with CF and respiratory therapists and reported problems with device replacement practices. Nebulizers and compressors are prescribed at care centers and can be acquired at the centers, at durable medical equipment (DME) companies, or online. In addition, these prescriptions are frequently treated as generics by DME companies; thus, individuals with CF are not receiving the devices they are prescribed. This may be due to low reimbursement for DME companies by third-party payers and/or limited availability to DME companies from distributors of these devices. The presence and amount of out-of-pocket expenses have been previously correlated to poor adherence to therapies.15 An already high burden of care can be increased by the lack of devices and/or use of inefficient/deteriorating devices, thus resulting in even lower adherence.16 This is crucial given the high cost of some of the medications used by individuals with CF. In addition, this could result in deteriorating health leading to hospitalizations and even higher health care cost.
Although clear guidelines for pulmonary treatments for individuals with CF are available, recommendations for type and number of nebulizers and compressors that are required to optimize care are lacking. The CFF convened a multidisciplinary task force to identify the key issues surrounding these concerns.
QUICK LOOK
Current Knowledge
Treatment of individuals with cystic fibrosis (CF) includes the use of several inhaled medications. Accessibility of nebulizers and compressors by this population is unknown.
What This Paper Contributes to Our Knowledge
A survey to health care providers and adults with CF/parents of children with CF revealed that perceptions regarding accessibility can be different at times. Most adults with CF/parents of children with CF reported problems with their compressors. An educational gap regarding care of nebulizers and compressors was found. Compressors and nebulizers able to withstand the continuous extended use by individuals with CF are needed.
Methods
The Nebulizer and Compressor Accessibility Task Force included various members of both pediatric and adult CF teams: respiratory therapists, a CF center director specialized in aerosol science, a nurse program coordinator, a social worker, an adult living with CF, and a parent of a child living with CF. Key representatives from the CFF were actively involved as well.
Several meetings were held to develop and refine the content of surveys targeting health care providers, adults with CF, and parents of children with CF (adults with CF/parents). The surveys were designed to address use, durability, accessibility, and cost burden of compressors and nebulizers, and the content was approved by all authors. The term health care providers refers to members of the CF multidisciplinary care team that could be involved in the process of acquisition of compressors and nebulizers (physicians, nurse practitioners, respiratory therapists, nurses, pharmacists, and social workers).
The surveys were administered online (SurveyMonkey), allowing respondents to skip questions. Participation was voluntary without provision of financial incentive for its completion. The study (Pro00040483) was reviewed by Advarra Institutional Review Board and deemed not human research.
The health care provider survey comprised nebulizer and compressor components and was distributed to all 287 CF programs through the CFF listservs (Supplementary Survey 1). This includes 48 states since there are no CF-accredited centers in the states of Hawaii and Wyoming. The adults with CF/parents survey was distributed online through the CF centers and through a CFF online platform (Community Voice) (Supplementary Survey 2). The latter group was comprised in 2019 of 1,153 individuals with CF and family members who have self-identified as wanting to participate in surveys and ongoing research done by the CFF.
All responses collected from the surveys were analyzed, including those with partial data. Some survey items allowed more than one response. Overall responses for both surveys were reported. Proportions were compared using chi-square statistics. Continuous variables were compared with unpaired t test. A P value < .05 was considered statistically significant. A statistical software was used for all calculations (KaleidaGraph 4.5.4, Synergy Software, Reading, Pennsylvania).
Results
Health Care Provider Surveys
Response rates to nebulizer and compressor surveys were 55.4% (159/287) and 62.4% (179/287), respectively. Responses were completed between November 8, 2018, and December 6, 2018. Respondents to the compressor survey worked at adult 30.2% (54/179), pediatric 41.9% (75/179), or combined pediatric/adult CF programs 30.2% (54/179), with one program that did not specify, 0.6% (1/179). Respondents to the nebulizer survey worked at adult 28.9% (46/159), pediatric 38.4% (61/159), or combined pediatric/adult CF programs 32.1% (51/159), with one program that did not specify, 0.6% (1/159). Respondents from 81.3% (39/48) of states with CFF CF programs completed the survey (Fig. 1).

Geographical distribution of survey respondents.
Compressor Survey Results
The coordination of ordering the compressors was done by respiratory therapists (47.5%, 85/179), nurses (41.3%, 74/179), respiratory therapists and nurses (2.2%, 4/179), and others (physician, pharmacist, social worker, clinic manager, medical assistant, case manager, 8.9%, 16/179).
Health care providers reported that Medicaid provided compressors for individuals with CF at different time intervals: 7.9% (14/178) every 2 y, 7.9% (14/178) every 3 y, 56.2% (100/178) every 5 y, 6.7% (12/178) at other intervals including 1 per lifetime in 2 respondents, and 21.3% (38/178) were not sure. Health care providers reported that private insurance provided compressors for individuals with CF at different intervals: 9% (16/178) every 2 y, 8.4% (15/178) every 3 y, 38.2% (68/178) every 5 y, 9.6% (17/178) at other intervals, and 34.3% (61/178) were not sure. Compressors were procured from different sources: DME companies 71.8% (127/177), clinic 8.5% (15/177), specialty pharmacy 6.8% (12/177), online 3.4% (6/177), and combination of all 9.6% (17/177).
Reported barriers to procure compressors though DME companies included limited supply option, limited-service areas, automatic substitution, standard limited reimbursement rates, and out-of-pocket cost. Barriers related to the warranty of the compressors included delays in delivery, and some manufacturer warranties are voided if used with hypertonic saline, a commonly prescribed therapy for CF.
Most health care providers (51.1%, 91/178) did not feel that the compressors used by their patients were durable and able to appropriately handle their inhaled treatment load. Device failure was the most common reason that supported this assessment. Pari Vios and Pari Vios PRO (Pari Respiratory Equipment, Midlothian, Virginia) were prescribed by 13.8% (24/174) and 50% (87/174), respectively, followed by 50 psi compressor (12.1%, 21/174), and other brands (24.1%, 42/174).
Nebulizer Survey Results
The coordination of ordering nebulizers was done by respiratory therapists (48.4%, 77/159), nurses (40.9%, 65/159), respiratory therapists and nurses (3.8%, 6/159), and others (physician, pharmacist, social worker, clinic manager, medical assistant, case manager, 6.9%, 11/159).
Most health care providers (69.2%, 108/156) expressed that they were not able to obtain enough nebulizers for their patients. Insurance restrictions were the most cited reason. The number of nebulizer units that practitioners would like to have for their patients in a 6-month period was 1–4 (44.7%, 71/159), 4–8 (41.5%, 66/159), > 8 (9.4%, 15/159), and other number (4.4%, 7/159).
The number of nebulizers covered every 6 months by Medicaid was 1 (38.2%, 60/157), 2 (13.4%, 21/157), 3 (1.9%, 3/157), 4–6 (3.8%, 6/157), other (8.9%, 14/157), and not sure (33.8%, 53/157). The number of nebulizers covered every 6 months by private insurance was 1 (19.7%, 31/157), 2 (10.2%, 16/157), 3 (2.5%, 4/157), 4–6 (3.2%, 5/157), other (12.1%, 19/157), and not sure (51%, 80/157).
Nebulizer were procured from different sources: DME companies (45.9%, 72/157), clinic (18.5%, 29/157), specialty pharmacy (9.6%, 15/157), online (4.5%, 7/157), and combination of all (23.6%, 37/157). Respondents reported that 57.3% (90/157) was able to give free nebulizers cups in clinic. The sources for free nebulizers were donations/fundraising, hospitals, and samples from vendors. The most common medical assistance program used by health care providers to procure nebulizers was HealthWell 37.7% (52/131).
Adults With CF/Parents Surveys
The CF community survey had a response rate of 63.7% (734/1,153) and included responses from 48 states (Fig. 1) and equal number of respondents of adults with CF/partner (49.2%, 361/734) and parents of children with CF (50.8%, 373/734). Responses were collected between March 25, 2019, to April 22, 2019. Respondents obtained health insurance through different sources including 73% (501/686) from private insurance through employer, family member, or self-purchased; 38% (261/686) from Medicaid/Medicare; and 15% (103/686) reporting more than one insurance.
Compressor Survey Results
Most adults with CF/parents (50.3%, 369/734) used Pari brand compressors, with Vios PRO being the most reported (33.4%, 245/734) (Supplementary Table 1, see related supplementary material at http://rc.rcjournal.com/). The second most used brand was Philips Respironics (11.2%, 82/734). Most adults with CF/parents (54.6% 395/723) did not replace the nebulizer filter every 6 months as recommended. Forty percent of respondents (260/723) never changed it, with 57.7% (150/260) of them stating they did not know they were supposed to change the filter.
Most adults with CF/parents (65.8%, 468/711) rated their compressor durable and able to withstand the treatment load. The following actions were reported related to their compressors: change hoses (78.5%, 508/647), place the compressor off the floor and away from fabrics (71.4%, 462/647), place compressor behind the individual during nebulization (28.3%, 183/647), and dusting the compressor (14.7%, 95/647).
Most adults with CF/parents (85.5%, 602/704) reported problems with their compressors. The two most commonly reported problems were “hoses popping off” (67.8%, 408/602) and “increased nebulization time” (62.5%, 376/602). A full list of reported problems can be seen in Table 1.
Problems With Compressors Reported by Adults With CF/Parents
Almost a quarter of adults with CF/parents (22.8%, 159/698) somewhat or strongly agreed that problems with their compressor prevented them from doing daily therapies. Coincidently, 19.8% (138/697) of respondents did not have access to a compressor at some point in the previous year, with 48.6% (67/138) reporting a duration > one week.
Almost half of the respondents (48.5%, 234/482) had an out-of-pocket expense in the previous 12 months related to compressors (median $75–99).
Nebulizer Survey Results
Adults with CF/parents used several nebulizer brands, with Pari nebulizers being the most used brand (64.1%, 785/1225), with Pari LC Plus the most commonly reported device (45.7%, 560/1225) (Supplementary Fig. 1, see related supplementary material at http://rc.rcjournal.com/). The second most used brand was Philips Respironics (18.9%, 232/1225), with most individuals with CF using SideStream and fewer using SideStream Plus (184/232, and 48/232, respectively).
Almost a quarter of adults with CF/parents (22.7%, 158/695) somewhat or strongly agreed that problems with their nebulizer prevented them from doing daily therapies. There was a 64.7% overlap between adults with CF/parents reporting somewhat or strong agreement that problems with their nebulizers and compressors prevented them from doing daily therapies. Almost half (49.5%, 362/731) of the respondents had an out-of-pocket expense in the previous 12 months related to nebulizers (median $50–74).
Adults with CF/parents (n = 696) reported doing a median (99% CI) of 4 (4–5) treatments per day. Respondents reported using inhaled aerosols at different rates: albuterol (55.5%, 372/698), hypertonic saline (88.5%, 530/675), dornase alfa (88.6%, 601/678), and inhaled antibiotics (45.8%, 289/660). A list of frequency of use of different inhaled medications is presented in Table 2.
Frequency of Administration of Inhaled Medications Reported by CF Patients
Adults with CF/parents obtained their nebulizer from different sources: through the CF center (282/974), online (253/974), through DME companies (149/974), at a pharmacy (144/974), and other (146/974). There was a wide variation in the reported length of use of an individual nebulizer, ranging from 1–12 months, with a median of 6 months. The median (99% CI) number of nebulizers that respondents thought it was ideal to have was 4 (4–4). Almost half of the respondents (46.3%, 319/689) thought that they did not have an adequate number of nebulizers for a 6-month period.
Respondents (n = 446) cleaned and washed with soapy water their nebulizers at different time intervals (65.2, 18.6, and 16.2% after each use, daily, and one per week, respectively). Respondents reported a wide variation of frequency of disinfection of the nebulizers: 65.2% (291/446) after each use, 18.6% (83/446) once per day, and 16.1% (72/446) once per week. Most respondents exclusively used a heat-based or a cold-based method of disinfection 86.7% (554/639) and 4.9% (31/639), respectively. Respondents used several disinfection methods (Fig. 2). The proportion of respondents who reported increase in nebulization time was similar between those using cold- (18/31) and heat-based methods (318/608) (P = .58). The proportion of respondents who reported compressor malfunction was similar between those using cold- (20/31) and heat-based methods (400/608) (P = .99). The number (mean, SD) of nebulizer treatments per day was higher in those reporting compressor malfunction (4.7, 2.4) than in those who did not (4.1, 2.4) (P = .007).
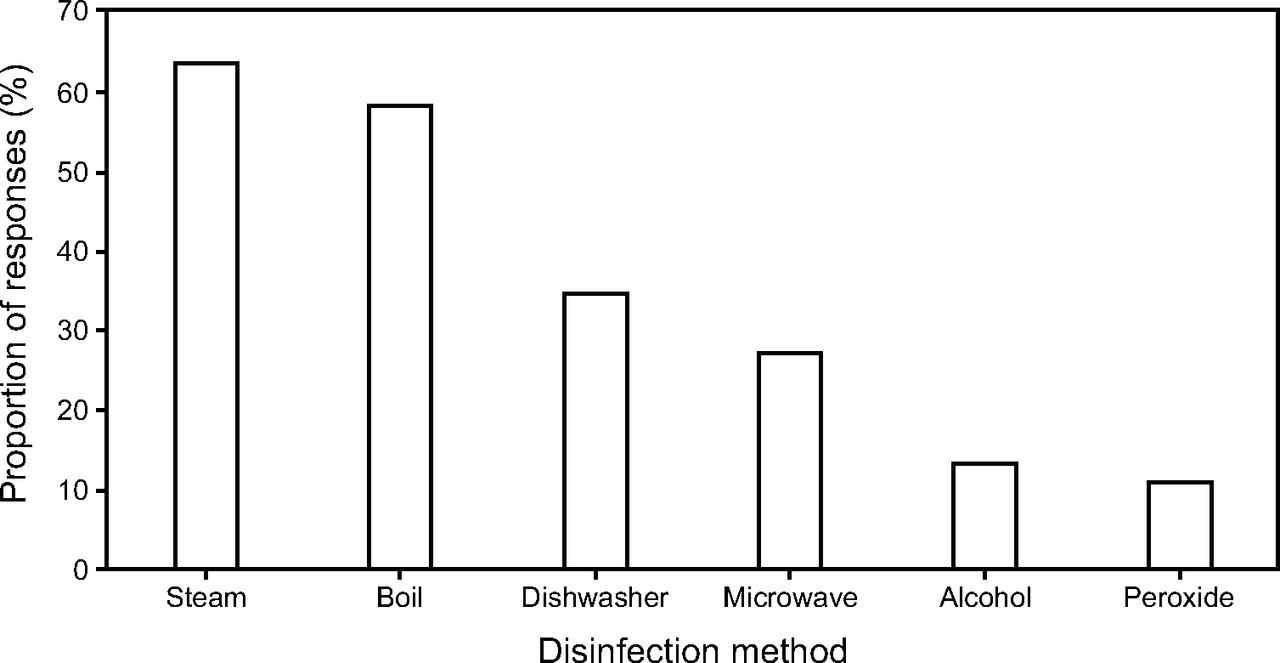
Nebulizer disinfection methods used by individuals with CF.
Discussion
These surveys completed by health care providers and adults with CF/parents of children with CF revealed opportunities for improvement in the use, accessibility, durability, and cost burden of compressors and nebulizers used by individuals with CF. Discrepancies between health care providers’ and adults with CF/parents’ perceptions on many aspects were noted. Most adults with CF/parents reported problems with their compressors. Areas for improvement in education and access to equipment were identified.
The health care provider’s survey had a high response rate and represented most CF programs (62.4% and 55.4% for compressor and nebulizer survey, respectively) and states (79.6%) in the United States. Moreover, the states represented by the respondents are home to 91% of all United States CF programs and follow 93.6% of all individuals with CF. Respiratory therapists and nurses were responsible for coordinating procurement of compressors and nebulizers. The adults with CF/parents responses were equally distributed between adults with CF and parents of children with CF and represented most states in the United States.
A wide variation in frequency of replacement of compressors by third-party payers was reported by health care providers, with one program reporting that individuals with CF were allowed only one compressor per lifetime. A significant number of health care providers was unaware of the allowed frequency for replacement (21–34%). This highlights the importance of adults with CF/parents serving as advocates for themselves by actively learning the rules of their health coverage to inform their treatment decisions. Health care providers reported that 71.8% of compressors was procured through a DME company.
Health care providers reported a higher percentage of prescription of Pari compressors (63.8%) than adults with CF/parents (50.3%). This difference could be because compressor prescriptions written for a specific brand/model are frequently treated as generics by DME companies, resulting in automatic substitution. This is mostly due to low reimbursement by third-party payers. We speculated that if better reimbursement rates were paid by third-party payers for compressors that are able to withstand the extended use seen in individuals with CF manufacturers will be motivated to build better devices.
Adults with CF/parents rated their compressor as more durable than health care providers. We speculated that this could be due to recall bias from the health care providers who only hear about the problems with compressors. This could also stem from a lack of understanding or knowledge on the user’s end of what determines proper function of a compressor. Interestingly, of adults with CF/parents who reported problems with their compressors, almost two-thirds reported increased nebulization time. This is consistent with recent report by Aquino et al,17 except they found a lower proportion of malfunctioning compressors. This difference could be attributed to the fact that their study measured the outcome and our survey inquired about user complaints of device function. Inquiring about prolonged duration of nebulization could serve as a screening tool for potential malfunctioning compressors. Care of the compressors was suboptimal, with a large number of adults with CF/parents not changing the filter as recommended. A knowledge gap was found with users not knowing they were supposed to perform maintenance care. Health care providers could use this knowledge to provide education to adults with CF/parents and review compressor operation, maintenance, and replacement both at the time of setup and annually to overcome this knowledge gap. A concerning finding was that about 20% of individuals with CF spent time without a compressor, with 10% of total respondents reporting a length more than a week. This finding highlights the importance of purchasing compressor units that have manufacturer warranty for replacement of defective equipment. The CF care team is a valuable resource regarding compressor acquisition for adults with CF/parents. In addition, individuals with CF with advanced lung disease could benefit from having a backup compressor to avoid potential interruptions of care.18
The adults with CF/parents reported a high burden of treatment with a median 4 inhaled treatments per day. These findings are consistent with previously published literature.7-8 As expected, a higher number of treatments was more frequent in those reporting compressor malfunction.
Health care providers overestimated the proportion of nebulizers obtained through DME companies. This could be due to differential pricing seen when traditional DME companies are compared to online services.
A wide variation in the number of nebulizers covered by insurances was reported. Similar to the compressor replacement lengths of time, a significant number of health care providers was unaware of the number of covered nebulizers (33–51%). Again, the importance of adults with CF/parents participating in the coproduction of their care is highlighted.19 The term coproduction of care refers to the interdependent cooperative work between health care providers and adults with CF/parents. In the case of compressors and nebulizers, it requires adults with CF/parents be familiar with their benefits and health care providers to advise on preferred devices and to educate on what financial resources are available.
Most health care providers thought that the number of nebulizers patients had on hand was not sufficient. However, the number of recommended nebulizers was lower than those recommended by adults with CF/parents. This could be confounded by the fact that there was a wide range of reported use of individual nebulizers by adults with CF/parents.
As expected, heat-based methods were the most frequently used means of disinfecting nebulizers. In contrast to reported studies, the use of a heat-based disinfection method was not associated with prolongation of nebulization time.11
Cleaning and disinfection were not done as frequently as recommended by CF infection control guidelines.20 Re-curring standardized education regarding the infection risks associated with improper cleaning and disinfecting nebulizers may help change this behavior. Also, having enough devices to be able to do a daily batch disinfection may be helpful with adherence to current recommendations.20
Almost half of the adults with CF/parents reported out-of-pocket expenses, with more money spent for compressors than for nebulizers. Health care providers should be familiar with available resources that can offset some of these costs.
One limitation of the study is that the participation of adults with CF/parents could be biased by their interest in participating in research. Another limitation is that the payer mix reported by the respondents is different from the data reported by the CFF in their 2019 Patient Registry Annual Data Report.21 The latter reported 58.6% and 52.2% for private and Medicaid/Medicare, respectively.
These survey results highlight the high burden of therapy, the need for compressors that withstand the number of treatments done by individuals with CF, the need for enough reusable nebulizer units covered every 6 months (one per prescribed medication), and the need for standardized education regarding compressor and nebulizers tailored to adults with CF/parents and health care providers. The education portfolio should include leaflets, videos, and web-based formats to be able to reach different type of learners. Frequent review of proficiency in cleaning and maintaining compressors and nebulizers is of utmost importance for delivery of inhaled medications. A summary of recommended practices of home nebulizer use and compressor care and their rationale is provided in Supplementary Table 2 (see related supplementary material at http://rc.rcjournal.com/). These recommendations were based on manufacturer’s recommendations of devices used by individuals with CF and on adults with CF/parents and health care provider experience.
Conclusions
Perceptions of health care providers and adults with CF/parents regarding compressors and nebulizers can be different at times. Individuals with CF need ongoing access to devices that can withstand the high burden of use required for optimal outcomes. Equipment malfunction was identified as a barrier to adherence to inhaled therapies. Discrepancies in survey results indicate there is opportunity for improved education and communication between adults with CF/parents and the CF care team regarding these devices.
Acknowledgments
We are thankful to the adults with CF/parents and health care providers who completed the surveys. We are thankful to Azi S Kaider from the Cystic Fibrosis Foundation who reviewed the manuscript.
Footnotes
- Correspondence: Ariel Berlinski MD, University of Arkansas for Medical Sciences, Department of Pediatrics, Pulmonary Medicine, 1 Children’s Way, Slot 512–17, Little Rock, Arkansas 72202. E-mail: BerlinskiAriel{at}uams.edu
Ms Blair discloses a relationship with Cystic Fibrosis Foundation, Boomer Esiason Foundation and Indiana University. Dr Marshall is an employee of Cystic Fibrosis Foundation. Dr Berlinski discloses relationships with AbbVie, Allergan, Anthera, DCI, Cempra, the Cystic Fibrosis Foundation, Mylan, the National Institutes of Health, Therapeutic Development Network, Trudell Medical, Vertex, Vivus, and the International Pharmaceutical Aerosol Consortium on Regulation and Science. The remaining authors have no conflict to disclose.
Ms Lester presented a version of this paper at the 2019 North American Cystic Fibrosis Conference, held October 31-November 2, 2019, in Nashville, Tennessee.
Supplementary material related to this paper is available at http://rc.rcjournal.com/.
- Copyright © 2021 by Daedalus Enterprises









{kind=link}
{kind=link}