

Abstract
BACKGROUND: As part of efforts to decrease length of hospital stay, a protocol for weaning noninvasive respiratory support was implemented using quality improvement methodology. The objective of this study was to determine whether protocol implementation decreased the time to wean to no respiratory support by 24 h (30% reduction) over 3 months in preterm infants 30–34 weeks gestational age.
METHODS: A quality improvement project was conducted with the following outcome measures: primary outcome measured was hours to wean; secondary outcomes included duration of respiratory support, length of stay, and postmenstrual age at feeding milestones; and balance measures were duration of oxygen exposure and growth velocity.
RESULTS: Data from 89 subjects were included. Following implementation, decreases were seen in time to wean (40% reduction, P < .001), length of stay (25% reduction, P = .02), and growth velocity (21% reduction, P = .02).
CONCLUSIONS: Implementing a weaning protocol decreases duration of support and length of stay in infants 30–34 weeks gestational age. Weaning respiratory support more quickly may decrease growth velocity.
- quality improvement
- standardization
- noninvasive respiratory support
- continuous positive airway pressure
- high-flow nasal cannula
Introduction
Respiratory insufficiency is common among infants admitted to the neonatal ICU.1 Nasal CPAP and high-flow nasal cannula therapy are commonly used to treat infants with respiratory insufficiency.2 Prolonged use of these methods of support has been associated with a variety of problems, including nasal trauma/deformity, pneumothorax, gaseous bowel distention, increased cost, and prolonged hospitalization.3 Premature cessation of use has also been associated with problems, including increases in apneic events, oxygen requirement, work of breathing, need for escalation of support or intubation, and psychological distress to the family due to failure to wean.3 Despite these well-described risks of prolonged or curtailed support, the methods used to wean or discontinue support are highly variable and subjective. A 2008 survey of providers found that 56% weaned ad hoc.4
Limited data are available to guide the weaning of noninvasive support in neonates, but a 2011 systematic review found that, when using nasal CPAP, weaning pressure to a predefined level and then stopping achieves shorter weaning time, duration of oxygen, and length of stay compared to using a graded time-off approach.3,5 This systematic review included 3 studies and was primarily impacted by a 2010 study by Todd et al.5 This prospective, randomized controlled trial compared 3 nasal CPAP discontinuation strategies, the most effective of which achieved fewer days of nasal CPAP, lower gestational age off nasal CPAP, shorter duration of oxygen use, lower rates of bronchopulmonary dysplasia, shorter length of stay, and lower gestational age at discharge. A retrospective analysis found that using this protocol for the weaning of support was preferable to ad hoc weaning to decrease the duration of respiratory support.6 To standardize our practice and improve our local outcomes, we developed and implemented a protocol based on the one used by Todd et al5 for the weaning and discontinuation of noninvasive respiratory support in neonates. Quality improvement methodology was used as this protocol was implemented as a practice change; infants were not randomized to an intervention, and the primary goal of the project was to improve care for the infants at the institution rather than answer a broader question.7
QUICK LOOK
Current Knowledge
Nasal CPAP and high-flow nasal cannula therapy have been used to support neonates with respiratory insufficiency not requiring invasive ventilation. The optimal method of decreasing or discontinuing this support is not known, but the use of a protocol has been associated with improved short- and long-term respiratory outcomes. The effectiveness of implementing a protocol on decreasing duration of weaning and length of stay is unknown.
What This Paper Contributes to Our Knowledge
Using quality improvement methodology to implement a protocol and standardize the weaning of noninvasive respiratory support decreased the duration of weaning and length of stay. Growth velocity was also decreased.
Methods
The University of Arkansas for Medical Sciences (UAMS) neonatal ICU is a 68-bed, level III unit inside a 437-bed university hospital, which delivered approximately 3,800 and admitted 1,092 infants in 2015 (> 95% inborn) with an average daily census of 57. To achieve the desired change, 235 health care workers were expected to comply with the protocol whenever appropriate. This included approximately 22 neonatologists, 10 pediatricians, 6 neonatal fellows, 1 neonatal nurse practitioner, 10–12 residents per month, 26 respiratory therapists, and 160 bedside nurses.
Problem Description/Rationale
During 2015, the length of stay in the UAMS neonatal ICU was longer than the 75th percentile for most birthweight subgroups compared to similar centers in the Vermont Oxford Network and showed a consistent upward trend over the previous 3 y. Respiratory weaning protocols have been shown to decrease duration of respiratory support, oxygen exposure, length of hospital stay, and rates of bronchopulmonary dysplasia.3,5 A survey revealed the neonatology faculty at our institution to be highly in favor of developing a respiratory weaning protocol, with 14 of 22 (64%) responding that they felt a weaning protocol would decrease length of stay, predominantly by allowing earlier initiation of oral feeding attempts.
Overuse or extended use of respiratory support is associated with adverse clinical outcomes.3 In the previous model at the study facility, weaning of noninvasive support was primarily driven by the providers’ workflow rather than the patients’ condition. Assessment for weaning had been sporadic and subjective, with support often weaned only once daily on rounds and rarely at night. This model was felt to prolong the patients’ exposure to this potentially noxious therapy and increase the cost of hospitalization (Fig. 1). Therefore, in 2017, a protocol for weaning noninvasive respiratory support was implemented in the neonatal ICU at UAMS using quality improvement methodology.7
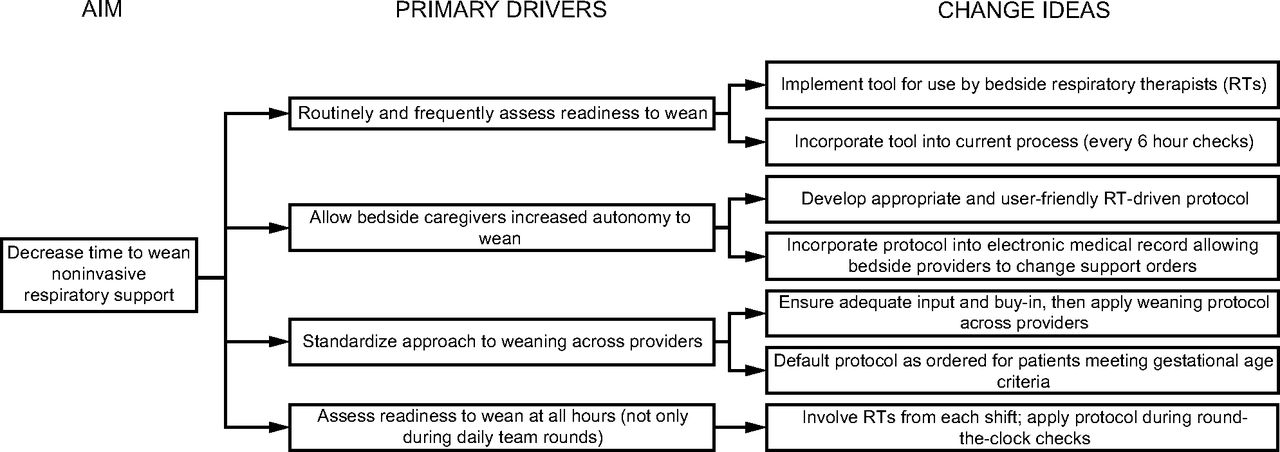
Driver Diagram.
Specific Aim
The objective of this study was to determine whether the implementation of a respiratory weaning protocol decreases the time to wean from nasal CPAP (≤ 8 cm H2O) or nasal cannula (≤ 3 L/min) to no respiratory support by 24 h (30% reduction) over 3 months in infants 30–34 weeks gestational age.
Interventions/Tests of Change
After surveying neonatology faculty, conducting a literature review, and discussing the topic at our neonatology section meeting, a task force was formed. This task force was led by a neonatal-perinatal medicine fellow and included representatives from the neonatology fellowship, pediatric residency, neonatology section, respiratory care, and nursing leadership. Although the task force did not include a parent/family representative, several members of the task force are parents of neonatal ICU graduates. This group developed a weaning protocol and plan for implementation, and drafts of the protocol were circulated for feedback.
The plan and protocol were refined and edited with input from the respiratory director, medical directors, nursing leadership, residents, fellows, faculty, and the task force. A version of the protocol used during implementation in included in the online supplementary material (see supplementary materials at http://www.rcjournal.com). The protocol was implemented using paper documentation in eligible infants on an opt-in basis in plan-do-study-act (PDSA) cycle 1 (Table 1). Respiratory therapists performed the assessments for readiness to wean using the criteria outlined in the protocol, and they implemented the wean, changing the settings at the bedside and in the order in the electronic medical record (EMR) without further input from the providers.
Plan-Do-Study-Act (PDSA) Cycles
After several weeks of success with the initial implementation, the protocol was universally implemented and ordered by default on all new admissions meeting gestational age criteria (> 30 weeks 0 d). With universal implementation, the documentation was integrated into the EMR in PDSA cycle 2 (Table 1). The institutional review board at UAMS was provided a summary of the project and determined that this is not human subject research. The revised standards for quality improvement reporting excellence (SQUIRE 2.0) were consulted in the preparation of this report.8
Measurements
The primary outcome measure was the time in hours to wean from nasal CPAP (≤ 8 cm H2O) or nasal cannula (≤ 3 L/min) to room air without nasal CPAP or nasal cannula (no respiratory support). This period was measured by manual review of the flow sheets in the EMR and defined as the time elapsed from the point an infant met criteria to wean until the respiratory support was discontinued and the infant was maintained off of respiratory support for at least 3 days. Additional outcome measures were the duration of any noninvasive respiratory support (including time on NIV or nasal cannula or CPAP at levels > 3 L/min or 8 cm H2O, respectively; measured in hours); length of stay (measured in days); and postmenstrual age at achievement of full enteral feeds (120 mL/kg/d), initiation of oral feeds, and achievement of full oral feedings. Covariate data included in the analysis were gestational age, birthweight, discharge weight, multiple gestation status, sex, race/ethnicity, mode of delivery, antenatal steroid administration, prolonged rupture, surfactant administration, and highest respiratory support required.
Process measures were the percentage of the time the weaning protocol was ordered by the provider and initiated by the therapist on appropriate patients, the percentage of time the periodic weaning assessments were documented appropriately on patients with the weaning protocol ordered, and the percentage of time the weaning protocol was appropriately applied and patients weaned. The balance measurements were the duration of oxygen exposure (hours of  > 0.21) and growth velocity during the entire hospitalization (g/d) measured by comparing birthweight and discharge weight and dividing by the number of days hospitalized.
> 0.21) and growth velocity during the entire hospitalization (g/d) measured by comparing birthweight and discharge weight and dividing by the number of days hospitalized.
These measures were obtained via monthly extraction from the EMR, which was completed by a manual review of the flow sheets. These data were reported locally in presentations to the team and updates at the Neonatal ICU Continuous Quality Improvement meetings, as well as nationally through formal poster sessions at professional meetings. Senior leaders (eg, division chief, medical director, respiratory coordinator, nursing director) were updated and engaged with the data.
Patients with gestational age at birth of 30 weeks 0 days to 34 weeks 6 days and discharged between September 1, 2016, and April 30, 2017, were included in the analysis if noninvasive respiratory support was required and support was discontinued before discharge or transfer. Infants were excluded if noninvasive support was needed > 10 d from the time infants met criteria to begin the protocol or if comorbidities were present (eg, major congenital anomaly, aneuploidy, congenital heart disease, pulmonary hypertension, or other condition requiring immediate transfer to another facility). Infants who failed the protocol were included in the analysis if they met the above criteria. Time to wean included any failed attempts at weaning and was calculated as the total time from when a subject met criteria to start the protocol (regardless of when the protocol was started) until a subject was first weaned off of respiratory support, as long as they remained off of support for at least 3 d (or hospital discharge).
Statistical Analysis
Available data were checked for outliers, extreme values, and distributional assumptions of the parametric statistical tests. Primary and secondary outcomes were compared using a 2-sample t test or Wilcoxon rank-sum test for continuous variables, and a chi-square test or Fisher exact test for categorical variables. Stata 9.4 (StataCorp, College Station, Texas) was used for statistical analyses.
Poisson regression was used to assess subject outcomes while adjusting for other covariates. Poisson regression was used because the outcome variables were non-normally distributed and skewed to the right. We determined skew by plotting histograms and assessing normality with the Shapiro-Wilk test. If the P value obtained from the Shapiro-Wilk test is < .05, then the variable is concluded not to be normally distributed. Table 2 is a summary table displaying the exponentiated coefficients of the protocol implementation only.
Poisson Regression Analysis of the Effect of Protocol Implementation on Subject Outcomes
Results
A total of 89 infants meeting criteria for inclusion were identified, and data from these infants were included in the analysis. Fifty-seven infants were admitted prior to protocol implementation and were weaned according to the previous method (ad hoc). Thirty-two infants were admitted after implementation and were weaned according to the protocol. The protocol was initially implemented on January 17, 2017, with full-scale implementation on February 14, 2017.
The run chart for our primary outcome measure of time to wean in hours illustrates a mean ± SD reduction that exceeded our goal (76 ± 39 h vs 45 ± 40 h, P < .001) (Fig. 2). Run charts for our secondary measures indicated significant changes in 2 areas. Figure 3 demonstrates a reduction in stay seen most prominently after PDSA cycle 1, which involved initial protocol implementation (32 ± 14 d vs 26 ± 14 d, P = .02). Figure 4 demonstrates an unexpected finding that growth velocity also decreased after PDSA cycle 1 (19 ± 8 g/d vs 15 ± 8 g/d, P = .02).

Annotated run chart depicting timing of interventions relative to the duration of respiratory support weaning. A signal was noted starting January 2017 with the majority of data points since that time below the initial goal (24-h reduction). Each point represents a single subject. The desired direction is downwards.

Annotated run chart depicting timing of interventions relative to the neonatal ICU length of stay. A signal was noted starting January 2017 with the majority of data points since that time below the baseline median. Each point represents a single subject. The desired direction is downwards.

Annotated run chart depicting timing of interventions relative to the growth velocity during hospitalization. A signal was noted starting January 2017 with the majority of data points since that time below the baseline median. Each point represents a single subject. The desired direction is upwards.
Table 3 illustrates that subject characteristics were similar before and after protocol introduction (PDSA cycle 1), including gestational age, birthweight, multiple gestation status, sex, race/ethnicity, delivery mode, antenatal corticosteroid administration, prolonged rupture of membranes, surfactant administration, and highest respiratory support required. The team has not identified other significant variability in secondary outcomes (see Table 4). The process measures indicated near 100% compliance.
Subject Characteristics Pre- and Post-Universal Protocol Implementation
Secondary Outcomes
Discussion
The interventions influenced the primary outcome by decreasing the duration of weaning. The trends were both statistically significant and clinically relevant. PDSA cycle 1, which involved initial implementation of the weaning protocol, appeared to have the greatest effect on the primary outcome. PDSA cycle 2, which involved universal implementation and EMR integration, produced sustained improvement. We have achieved our aim of decreasing the duration of respiratory support by > 24 h. It remains to be seen whether this will be a sustained improvement in our neonatal ICU. This project illustrates that establishing and implementing a protocol to wean noninvasive respiratory support in neonates can decrease the duration of support and neonatal ICU length of stay.
Patients are often billed according to the level of respiratory support required by respiratory care services and neonatology providers. Therefore, each additional day on nasal CPAP incurs an added cost. Reducing the duration of respiratory support by > 24 h is likely to produce significant cost reduction. This savings estimate is conservative, considering that providers and hospitals frequently bill for critical care days when infants are on nasal CPAP support, and that we observed a decrease in length of stay.
Our project raises concern that weaning respiratory support more quickly may negatively affect growth velocity, perhaps by impacting work of breathing and caloric expenditure. This finding warrants further investigation and was not reported in previous studies.2,4 This finding emphasizes the importance of considering the impact that weaning respiratory support may have on caloric expenditure and therefore carefully optimizing caloric intake in this setting.
Time to full feeds was included as a secondary outcome measure because gaseous bowel distention (ie, so-called CPAP belly) is a well-described complication of noninvasive respiratory support in neonates. This distention is a familiar clinical phenomenon that can interfere with feeding advancement in preterm newborns.9,10 It is for this reason that postmenstrual age at full enteral feeds was included as a secondary outcome measure. We did not, however, demonstrate a difference in this outcome.
We also did not demonstrate a difference in postmenstrual age at the relevant milestones (wean from respiratory support, wean to  of 0.21, first enteral feed, first oral attempt, full oral attempt, and discharge). The sample size may not have been powered to detect these differences.
of 0.21, first enteral feed, first oral attempt, full oral attempt, and discharge). The sample size may not have been powered to detect these differences.
Our results confirm those of earlier studies regarding the use of a protocol to wean noninvasive respiratory support. Our previous method of weaning has been used and reported by others; a 2008 survey of neonatal providers in New Zealand reported that 56% of providers weaned ad hoc, using criteria such as work of breathing, tachypnea, apnea, and blood gas values to guide weaning strategy.4 A meta-analysis indicated that sequential reduction and cessation of nasal CPAP is preferable to a graded time-off strategy for nasal CPAP weaning.3 Graded time-off refers to a weaning method that involves increasing periods off CPAP and “sprinting” on either no respiratory support or low-flow nasal cannula. Sequential reduction followed by cessation achieved less total time on nasal CPAP, shorter duration of oxygen therapy, and shorter length of stay compared to the graded time-off approach.3
The largest and most recent trial of nasal CPAP weaning techniques was conducted by Todd et al,5 published in 2010. This trial randomized infants to 1 of 3 nasal CPAP discontinuation strategies, the most effective of which achieved fewer days of nasal CPAP, lower gestational age off nasal CPAP, shorter duration of oxygen use, lower rates of bronchopulmonary dysplasia, shorter length of stay, and lower gestational age at discharge. This effective technique was later termed CICADA, an acronym for ceasing CPAP at standard criteria, and was used in a subsequent study. Heath Jeffery et al6 compared outcomes during 3 time periods and reported decreased nasal CPAP days, chronic lung disease, mechanical ventilation days, and fewer infants with surgically- and medically-treated patent ductus arteriosus after implementing the CICADA protocol. We modeled our protocol to resemble the CICADA criteria, with adaptations to make the protocol clearly understandable and seamlessly integrated into our respiratory therapists’ current workflow.
Strengths and Limitations
These observational data were collected in a small number of infants at a single institution. Data were collected only in infants 30–34 weeks gestational age at birth. All infants were supported using a nasal cannula interface for CPAP and high flow delivery (RAM cannula, Neotech, Valencia, California). Simultaneous initiatives to transition to a cue-based oral feeding system and standardization of discharge practices related to caffeine and apneic events were implemented. It is likely these other changes also impacted length of stay and infant outcomes, including growth velocity. These factors limit the generalizability of our results; however, infants 30–34 weeks gestational age with mild to moderate lung disease in level III neonatal ICUs comprise a large number of admissions and hospital days.6 If these findings are confirmed in future studies, the impact of appropriate weaning of noninvasive respiratory support will be substantial.
The data were obtained via manual extraction from the flow sheets entered into the EMR by bedside providers. This extraction, however, was time consuming, making it difficult to sustain over a long collection period and to keep updated for real-time reporting and analysis. An automated collection system integrated into the EMR would be preferable to maintain data collection for this type of intervention. The before-and-after analysis is another limitation of the study. The exclusion of infants requiring prolonged noninvasive respiratory support limits the generalizability of these findings to infants with bronchopulmonary dysplasia or other diseases of chronic respiratory insufficiency in infants. A weaning protocol such as this is may be most effective in infants with transient tachypnea of the newborn or mild respiratory distress syndrome of the newborn.
Conclusions
Implementing an evidence-based protocol for the systematic gradual reduction and discontinuation of noninvasive respiratory support in preterm neonates reduced duration of respiratory support and length of stay in infants 30–34 weeks gestational age at birth. Weaning respiratory support more quickly may be associated with decreased growth velocity. This protocol can be adapted and spread to other contexts, including community hospitals where noninvasive respiratory support may be used but providers may not be present for 24-h in-house coverage. Next steps should include using this protocol in additional settings while continuing to evaluate its effectiveness.
Further integration into the EMR with automated decision support and improved data reporting should also be tested to determine if infant outcomes are affected. This study evaluated the use of a weaning protocol in infants 30–34 weeks gestational age predominantly affected by respiratory distress syndrome or transient tachypnea of the newborn. Further research should evaluate this or similar protocols as they are implemented in infants at younger and older gestational ages or with different underlying pathologies contributing to their respiratory distress.
Footnotes
- Correspondence: David N Matlock MD, University of Arkansas for Medical Sciences, 4301 W Markham St, Slot 512-5B, Little Rock, AR 72205. E-mail: DMatlock{at}uams.edu
Dr Matlock presented a version of this paper at the 2017 annual meeting for the Vermont Oxford Network, held in Chicago, IL; by Dr Matlock at the 2017 annual meeting for Southern Society for Pediatric Research, held in New Orleans, LA; by Dr Matlock at the 2018 annual meeting for Society for Pediatric Research, held in Toronto, Ontario; and by Dr Ross at the 2018 annual meeting for Children’s Hospitals Neonatal Consortium, held in Columbus, OH.
Supplementary material related to this paper is available at http://www.rcjournal.com.
The authors have disclosed no conflicts of interest.
- Copyright © 2021 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}
{kind=link}