

Abstract
BACKGROUND: High-flow oxygen therapy via tracheostomy (HFT) can be used in tracheostomized patients during ventilator disconnection. The physiologic effects of this technique are unknown. We hypothesized that HFT would reduce inspiratory effort and improve breathing pattern compared to conventional oxygen therapy via T-tube. This study aimed to evaluate the physiologic effects of HFT compared to conventional O2 in patients with prolonged mechanical ventilation.
METHODS: A randomized crossover physiologic study was conducted in adult tracheostomized patients who experienced temporary periods of ventilator disconnection. Subjects were ventilated with pressure support ventilation (PSV) for 15 min and were then randomly assigned to HFT or conventional O2 via T-tube for 30 min. After a washout period, subjects were switched to the other system. Esophageal pressure (Pes), breathing frequency, blood pressure, heart rate,  , and transcutaneously measured pressure of carbon dioxide (
, and transcutaneously measured pressure of carbon dioxide ( ) were recorded. The primary outcome was inspiratory effort as determined by the simplified esophageal pressure-time product (sPTPes). Secondary outcomes were Pes swing, breathing frequency, heart rate, mean arterial pressure,
) were recorded. The primary outcome was inspiratory effort as determined by the simplified esophageal pressure-time product (sPTPes). Secondary outcomes were Pes swing, breathing frequency, heart rate, mean arterial pressure,  , and
, and  between groups.
between groups.
RESULTS: Twenty-two subjects were enrolled: sPTPes per minute was significantly higher with HFT and conventional O2 compared to PSV (153.5 ± 97.9, 163.5 ± 111.3, and 86.8 ± 51.1 cm H2O × s/min, respectively, P = .001), but it was not different between HFT and conventional O2 (P = .72). Breathing frequency increased significantly after switching from PSV to HFT and conventional O2 (23 ± 4 vs 26 ± 6 and 23 ± 4 vs 27 ± 5 breaths/min, respectively, P = .001).  was higher with conventional O2 compared to HFT (P = .02). No differences in
was higher with conventional O2 compared to HFT (P = .02). No differences in  , mean arterial pressure, or heart rate were observed between HFT and conventional O2.
, mean arterial pressure, or heart rate were observed between HFT and conventional O2.
CONCLUSIONS: Inspiratory effort and breathing frequency increased significantly during unassisted breathing compared to PSV in tracheostomized subjects, but HFT via tracheostomy provided no measurable additional physiologic benefit compared to O2 therapy via T-tube.
Introduction
Tracheostomy is commonly performed in 10–15% of critically ill patients requiring prolonged mechanical ventilation to facilitate the weaning process,1,2 and it has been increasingly used during the past decade.3 A recent propensity-matched cohort study in subjects with ARDS reported that ICU and hospital length of stay were longer in those with tracheostomy.4 While subjects with tracheostomy had the highest survival probability, there was no difference in 60-d or 90-d mortality in the subjects who survived for ≥ 5 d in the ICU, or in a propensity-matched subsample.4 Many tracheostomized patients remain on mechanical ventilation for a substantial duration, which may increase the risk of developing complications of prolonged mechanical ventilation and increased mortality.5–7 Increases in ICU and hospital stay also impose a large economic burden. Interventions to shorten the duration of mechanical ventilation in tracheostomized patients are, therefore, welcome.
When tracheostomized patients are ready to wean, conventional oxygen therapy via T-tube or collar mask is often used.6 However, many patients do not tolerate prolonged periods of disconnection and may experience increased work of breathing and desaturation. In addition, hypoxemia may occur due to variable  with a low-flow oxygen delivery system. Clearance of secretions is frequently a major issue, and adequate humidification of the airway may benefit the mucociliary system and reduce dryness symptom.8–10 Therefore, optimizing patient's work of breathing, adequate humidification, and trying to improve respiratory muscle function by repeated disconnection periods may facilitate weaning in mechanically ventilated patients after tracheostomy.11
with a low-flow oxygen delivery system. Clearance of secretions is frequently a major issue, and adequate humidification of the airway may benefit the mucociliary system and reduce dryness symptom.8–10 Therefore, optimizing patient's work of breathing, adequate humidification, and trying to improve respiratory muscle function by repeated disconnection periods may facilitate weaning in mechanically ventilated patients after tracheostomy.11
High-flow oxygen therapy via nasal cannula (HFNC) has been increasingly used as ventilatory support. Physiological studies in subjects with acute hypoxemic respiratory failure have demonstrated significant reduction in patient work of breathing and improved gas exchange after administration of HFNC.12–14 HFNC may decrease the need for endotracheal intubation in patients with moderate to severe hypoxemia.15,16 Current high-flow oxygen systems can be applied with tracheostomy tube via a dedicated interface.17 However, the effect of high-flow oxygen via tracheostomy (HFT) is unclear and may differ from a conventional use of HFNC because the upper airway is bypassed by the tracheostomy.18–20 We hypothesized that HFT would reduce inspiratory effort and improve breathing pattern in tracheostomized patients on prolonged mechanical ventilation. Our objectives were to compare the physiologic effects of HFT and conventional O2 via T-tube in terms of inspiratory effort, breathing pattern, and hemodynamics.
Quick Look
Current Knowledge
Conventional oxygen therapy via T-tube or collar mask is often used in tracheostomized patients who are ready to wean. High-flow oxygen can be applied with a tracheostomy tube via a dedicated interface. The physiologic effects of high-flow oxygen therapy via tracheostomy may differ from conventional high-flow oxygen via nasal cannula because the tracheostomy bypasses the upper airway.
What This Paper Contributes to Our Knowledge
Inspiratory effort significantly increased after switching from pressure support ventilation to unassisted breathing in tracheostomized subjects on prolonged mechanical ventilation. High-flow oxygen therapy via tracheostomy did not decrease inspiratory effort and breathing frequency compared to conventional oxygen therapy via T-tube.
Methods
Study Design and Population
This was a randomized, crossover, physiologic study conducted in the respiratory ICU of the Department of Medicine, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand, from July 2018 to April 2019. This study was approved by the Siriraj Institutional Review Board (#Si 322/2018) and was registered in the Thai Clinical Trial Registry (#TCTR20180612001). Written informed consent to participate was obtained from each subject or their relatives.
We enrolled tracheostomized subjects aged 18 to 90 y who were mechanically ventilated with pressure support ventilation (PSV) with the following criteria: pressure support ≤ 10 cm H2O, PEEP ≤ 8 cm H2O,  ≤ 0.5, Glasgow coma score > 8, and able to tolerate transient periods of disconnection.21 Patients were excluded if they met any of the following criteria under PSV: unstable hemodynamics (eg, systolic blood pressure > 180 or < 90 mm Hg, diastolic blood pressure > 100 or < 60 mm Hg, heart rate > 140 or < 60 beats/min, or any sign of poor tissue perfusion); breathing frequency > 35 breaths/min;
≤ 0.5, Glasgow coma score > 8, and able to tolerate transient periods of disconnection.21 Patients were excluded if they met any of the following criteria under PSV: unstable hemodynamics (eg, systolic blood pressure > 180 or < 90 mm Hg, diastolic blood pressure > 100 or < 60 mm Hg, heart rate > 140 or < 60 beats/min, or any sign of poor tissue perfusion); breathing frequency > 35 breaths/min;  < 92%; severe acid/base disturbance (ie, arterial pH < 7.3 or > 7.55); contraindication for esophageal balloon catheter insertion; or pregnancy.
< 92%; severe acid/base disturbance (ie, arterial pH < 7.3 or > 7.55); contraindication for esophageal balloon catheter insertion; or pregnancy.
Device
The Airvo 2 high-flow oxygen device (Fisher & Paykel Healthcare, Auckland, New Zealand) used in this study consists of a flow generator (≤ 60 L/min), an air-oxygen blender that allows for adjustment of  from 21–100%, and an auto-fill MR290 heated chamber. The gas mixture at 37°C was delivered via a single-limb heated breathing tube to the patient via the Optiflow tracheostomy interface (Fisher & Paykel) (Fig. 1).
from 21–100%, and an auto-fill MR290 heated chamber. The gas mixture at 37°C was delivered via a single-limb heated breathing tube to the patient via the Optiflow tracheostomy interface (Fisher & Paykel) (Fig. 1).

Tracheostomy interface with high-flow oxygen delivery system.
An esophageal balloon catheter (CooperSurgical, Trumbull, Connecticut) was inserted through the nose and positioned in the lower third of the esophagus. The balloon was filled with 1 mL of air according to the manufacturer's instruction and connected to a pressure transducer (BIOPAC Systems, Goleta, California). The correct position of the esophageal balloon was checked by identifying cardiac artifact and applying gentle pressure on the abdomen to verify the absence of gastric pressure fluctuations; then an occlusion test was performed to confirm the position of the esophageal catheter.22 Esophageal pressure (Pes) was recorded with an MP150 Data Acquisition System and AcqKnowledge Data Acquisition and Analysis Software (BIOPAC Systems).
Study Protocol
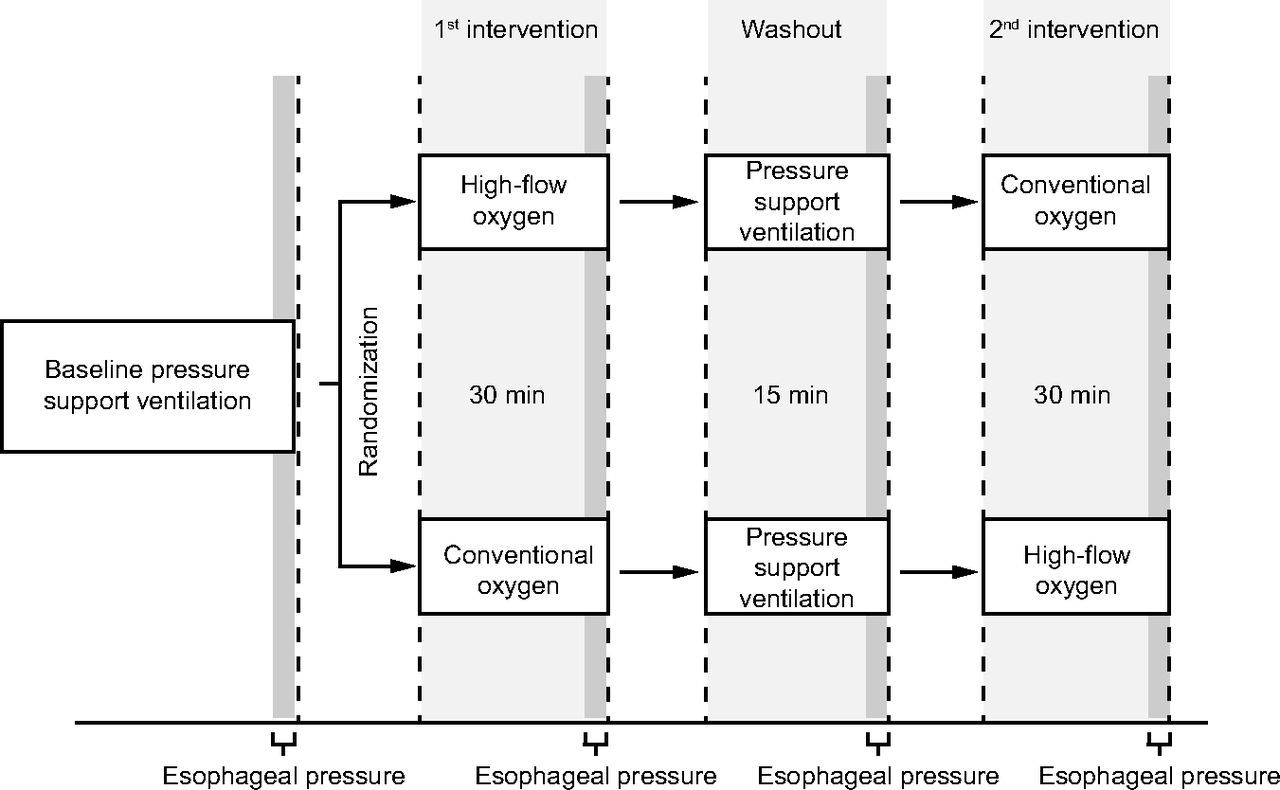
Subjects were initially ventilated with PSV using their clinical settings for 15 min. We randomized subjects using a sealed opaque envelope to receive in a randomized order either HFT at a flow of 50 L/min and  0.4, or conventional O2 via T-tube with 100% oxygen at a flow of 10 L/min through the AQUAPAK humidification system (Teleflex, Wayne, Pennsylvania). Each intervention was applied for 30 min. Baseline PSV was then applied for 15 min during the washout period following the first intervention. The second intervention (HFT or conventional O2) was applied in a crossover fashion for 30 min (Fig. 2). The cuff of the tracheostomy tube was inflated during the study intervention period to reduce the risk of aspiration of secretions above the cuff and to maximize the physiologic effects of HFT. After completion of the study protocol, the types and settings of ventilator support were decided by the attending physicians.
0.4, or conventional O2 via T-tube with 100% oxygen at a flow of 10 L/min through the AQUAPAK humidification system (Teleflex, Wayne, Pennsylvania). Each intervention was applied for 30 min. Baseline PSV was then applied for 15 min during the washout period following the first intervention. The second intervention (HFT or conventional O2) was applied in a crossover fashion for 30 min (Fig. 2). The cuff of the tracheostomy tube was inflated during the study intervention period to reduce the risk of aspiration of secretions above the cuff and to maximize the physiologic effects of HFT. After completion of the study protocol, the types and settings of ventilator support were decided by the attending physicians.

Flow chart.
Data Collection
Baseline demographic and clinical data were collected before randomization. During the study intervention period, heart rate and breathing frequency were recorded every 5 min, and blood pressure was recorded every 15 min, including at the beginning and the end of each step. The observed values of breathing frequency, heart rate, and mean arterial pressure in the last minute of recording were reported.  and transcutaneously measured pressure of carbon dioxide (
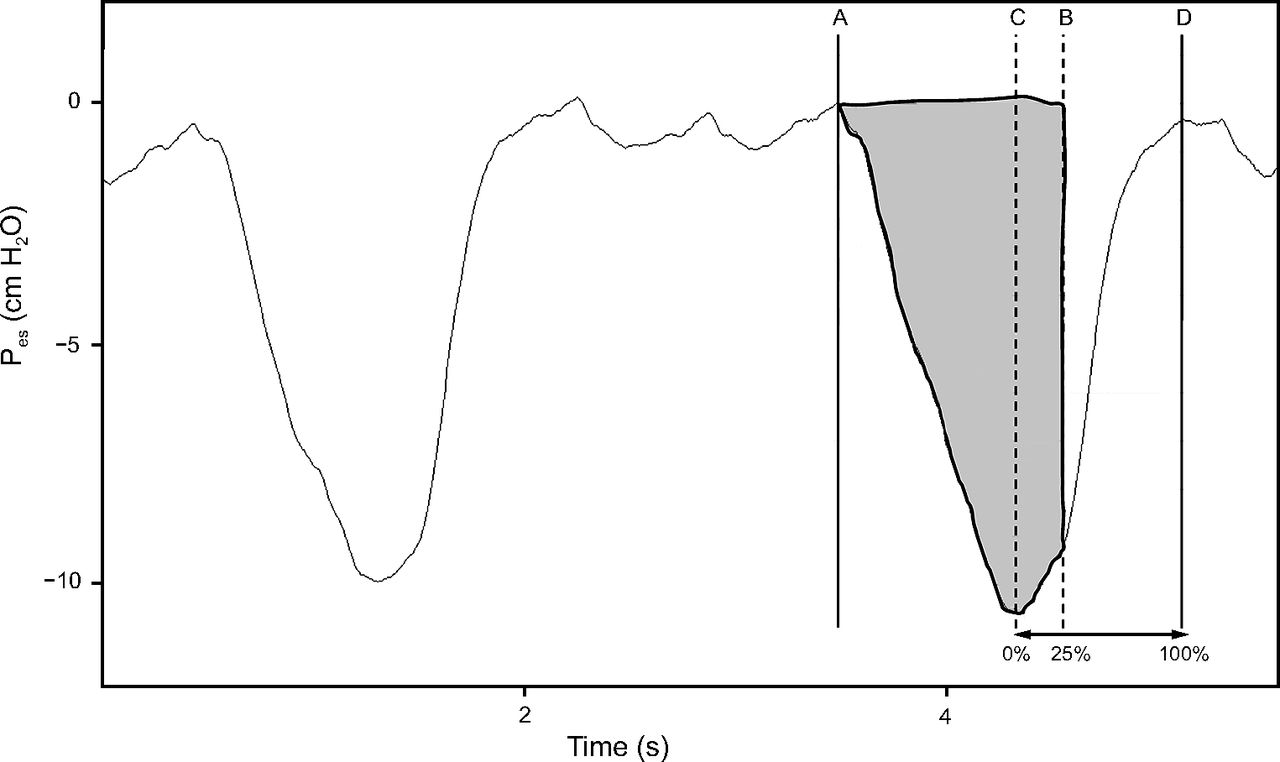
and transcutaneously measured pressure of carbon dioxide ( ) were recorded continuously using a SenTec Digital Monitoring System (SenTec, Therwil, Switzerland). We continuously recorded Pes waveforms for 5 min at the end of each step. Pes was analyzed offline with the investigator blinded to the mode of support using the waveforms of the last 2 min of recording to calculate Pes swing and esophageal pressure-time product (PTPes) per breath (cm H2O × s) and per minute (cm H2O × s/min) as an index of inspiratory effort using the dedicated AcqKnowledge Data Acquisition and Analysis Software. The measurement of chest wall elastance would need passive ventilation and was not obtained. Moreover, determining the end of inspiration requires an air flow signal, which cannot be obtained from a pneumotachograph during HFT. Therefore, we modified the calculation of PTPes per breath by integrating the area under the Pes signal from the onset of Pes decay to the point that Pes elapsed 25% of time from its maximum deflection to return to baseline (Fig. 3). This simplified technique has been used and reported in the previous studies,23–25 and we refer to it in this study as the simplified PTPes (sPTPes). sPTPes per minute was obtained by multiplying sPTPes per breath by breathing frequency. The average value of Pes swing, sPTPes per breath, and sPTPes per minute were reported.
) were recorded continuously using a SenTec Digital Monitoring System (SenTec, Therwil, Switzerland). We continuously recorded Pes waveforms for 5 min at the end of each step. Pes was analyzed offline with the investigator blinded to the mode of support using the waveforms of the last 2 min of recording to calculate Pes swing and esophageal pressure-time product (PTPes) per breath (cm H2O × s) and per minute (cm H2O × s/min) as an index of inspiratory effort using the dedicated AcqKnowledge Data Acquisition and Analysis Software. The measurement of chest wall elastance would need passive ventilation and was not obtained. Moreover, determining the end of inspiration requires an air flow signal, which cannot be obtained from a pneumotachograph during HFT. Therefore, we modified the calculation of PTPes per breath by integrating the area under the Pes signal from the onset of Pes decay to the point that Pes elapsed 25% of time from its maximum deflection to return to baseline (Fig. 3). This simplified technique has been used and reported in the previous studies,23–25 and we refer to it in this study as the simplified PTPes (sPTPes). sPTPes per minute was obtained by multiplying sPTPes per breath by breathing frequency. The average value of Pes swing, sPTPes per breath, and sPTPes per minute were reported.
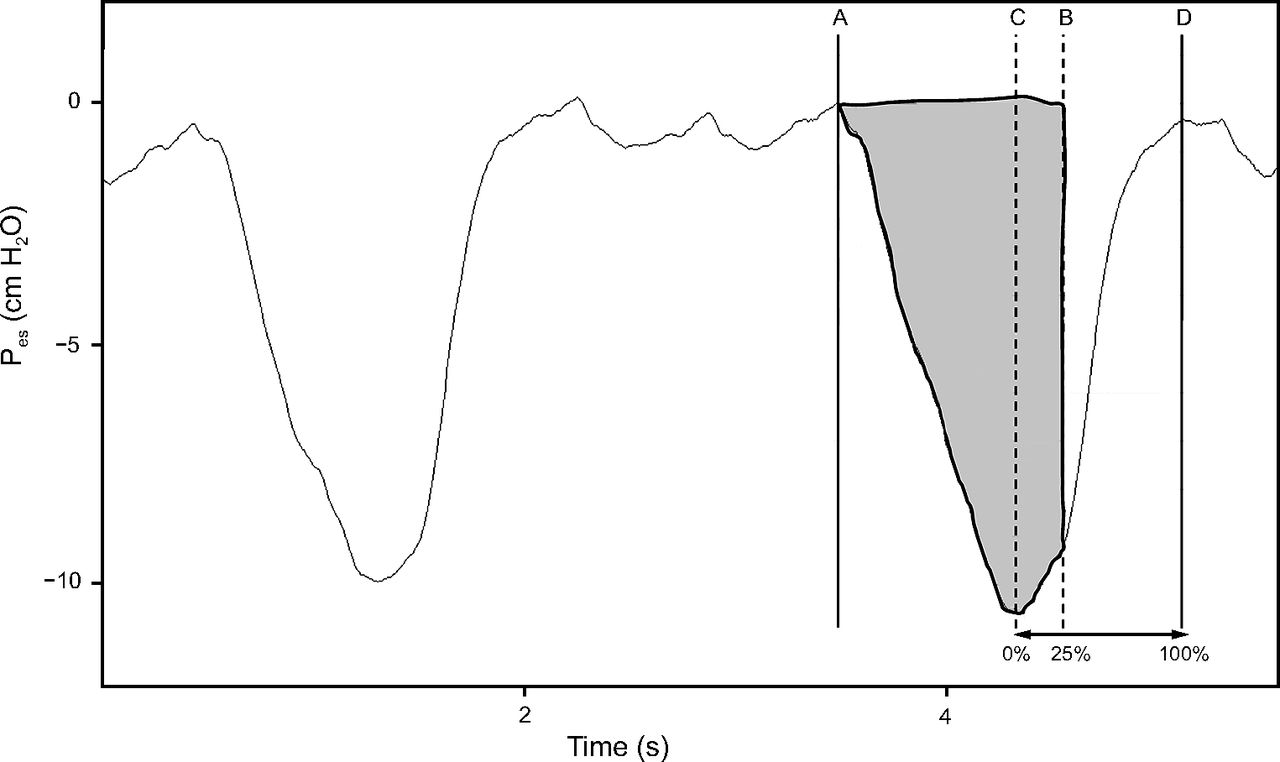
Calculation of simplified esophageal pressure-time product by integrating the area under the Pes signal (gray area). The beginning of the inspiration is the instant of the Pes decay (A), and the end of the inspiration is the point of Pes that elapsed 25% of time (B) from its maximum esophageal pressure deflection (C) to return to baseline (D). Pes = esophageal pressure.
Outcomes
The primary outcome was inspiratory effort as evaluated by sPTPes per minute between HFT and conventional O2 via T-tube as well as between baseline PSV and each intervention. Secondary outcomes were difference in sPTPes per breath, Pes swing, breathing frequency, heart rate, mean arterial pressure,  , and
, and  between HFT and conventional O2.
between HFT and conventional O2.
Statistical Analysis
The sample size was calculated on the basis of the previous study comparing HFNC with standard oxygen in subjects with acute hypoxemic respiratory failure12 and an estimated decrease in PTPes of 30% in the HFT group. With a 2-sided significance level of .05 and power of 80%, the estimated sample size was 22 subjects.
Continuous variables are presented as mean ± SD or median (interquartile range [IQR]). Categorical variables are presented as absolute number and percentage. Normality of data distribution was tested with the Kolmogorov-Smirnov test. For normally distributed data, we used an analysis of variance (ANOVA) with repeated measures followed by a post hoc pairwise comparison. Non-normally distributed data were compared with the Friedman 2-way ANOVA by ranks with a post hoc pairwise comparison. Data were analyzed using PASW Statistics 18 (SPSS, IBM, Armonk, New York). P < .05 was considered statistically significant.
Results
Twenty-two tracheostomized subjects with prolonged mechanical ventilation (mean ventilator days of 27 ± 21 d) were enrolled. The mean age was 73 ± 10 y, 15 subjects (68%) were male, and the mean Acute Physiologic and Chronic Health Evaluation (APACHE) II score was 20 ± 3. All subjects were ventilated in PSV mode at a mean pressure support level of 8 ± 1 cm H2O, PEEP of 5 ± 0 cm H2O, and  of 0.36 ± 0.06. Other baseline characteristics are detailed in Table 1.
of 0.36 ± 0.06. Other baseline characteristics are detailed in Table 1.
Baseline Demographic and Clinical Characteristics
Inspiratory Effort
During PSV, sPTPes per minute was 86.8 ± 51.1 cm H2O × s/min. During conventional O2 via T-tube and HFT, sPTPes per minute increased significantly (163.5 ± 111.3 and 153.5 ± 97.9 cm H2O × s/min, respectively) to a similar extent compared to PSV (P = .001). No significant difference in sPTPes per minute was observed between conventional O2 and HFT (P = .72) (Fig. 4). Changes in sPTPes per breath and Pes swing with conventional O2 and HFT compared to PSV were also in the same direction as sPTPes per minute (Table 2).

Individual data and mean value of simplified esophageal pressure-time product (sPTPes) per minute during pressure support ventilation, conventional oxygen therapy, and high-flow oxygen via tracheostomy.
Breathing Frequency and Gas Exchange
Breathing frequency was significantly higher with conventional O2 compared to PSV (27 ± 5 vs 23 ± 4 breaths/min, respectively, P = .001) and with HFT compared to PSV (26 ± 6 vs 23 ± 4 breaths/min, respectively, P = .006). There was no difference in breathing frequency between HFT versus conventional O2 (P = .90) (Table 2). The median  was significantly higher with conventional O2 than HFT (100% [IQR 100–100] vs 99% [IQR 99–100], respectively, P = .02), but no significant difference in
was significantly higher with conventional O2 than HFT (100% [IQR 100–100] vs 99% [IQR 99–100], respectively, P = .02), but no significant difference in  was observed between conventional O2 and PSV (P = .08) or HFT and PSV (P = .55). There was no significant difference in
was observed between conventional O2 and PSV (P = .08) or HFT and PSV (P = .55). There was no significant difference in  among PSV, conventional O2, and HFT (39.5 ± 6.5 vs 39.7 ± 6.3 vs 38.0 ± 11.4 mm Hg, respectively, P = .67) (Table 2).
among PSV, conventional O2, and HFT (39.5 ± 6.5 vs 39.7 ± 6.3 vs 38.0 ± 11.4 mm Hg, respectively, P = .67) (Table 2).
Hemodynamics
No significant differences in mean arterial pressure were found between PSV, conventional O2 via T-tube, and HFT (89 ± 13 vs 92 ± 13 vs 90 ± 11 mm Hg, respectively, P = .10) (Table 2). There was no significant difference in heart rate among PSV, conventional O2, and HFT (86 ± 19 vs 87 ± 17 vs 87 ± 17 beats/min, respectively, P = .55) (Table 2).
Adverse Events
No adverse event was observed during the study period and all subjects tolerated both interventions until the end of the study.
Discussion
Our results indicate that inspiratory effort as determined by sPTPes per minute, sPTPes per breath, and Pes swing and breathing frequency increased significantly after switching from mechanical ventilation with PSV to spontaneous breathing in tracheostomized subjects on prolonged mechanical ventilation. HFT did not decrease inspiratory effort or breathing frequency compared to conventional O2 via T-tube. No differences were observed in  , mean arterial pressure, and heart rate between conventional O2 and HFT.
, mean arterial pressure, and heart rate between conventional O2 and HFT.
The benefits of HFNC in patients with acute hypoxemic respiratory failure are well established. A large randomized controlled study by Frat et al15 reported lower 90-d mortality compared to standard oxygen and noninvasive ventilation in subjects with moderate to severe hypoxemic respiratory failure. In addition, a recent meta-analysis reported that HFNC may decrease the need for endotracheal intubation and escalation of oxygen therapy in subjects with moderate to severe hypoxemia.16 However, high-flow oxygen in these clinical studies was applied with nasal cannula. High-flow oxygen can also be used with tracheostomy tube via a dedicated interface,17 although data regarding physiologic effects and clinical outcomes are limited.18–20
We found no significant difference in inspiratory effort as determined by sPTPes per minute, sPTPes per breath, and Pes swing between HFT and conventional O2 via T-tube. A study by Corley et al18 compared HFT at 50 L/min with conventional O2 via T-tube at 15 L/min in 20 tracheostomized subjects who were weaned from mechanical ventilation in randomized crossover fashion. They reported significant improvement in oxygenation with HFT as determined by  , but no differences in breathing frequency, end-tidal CO2, end-expiratory lung volume, or heart rate between the 2 groups. The duration of each intervention was short (ie, only 20 min), and the effect on inspiratory effort was not investigated. Our findings are consistent with a recent prospective crossover study by Stripoli et al,19 who compared conventional O2 via T-tube at a flow of 10 L/min to HFT with a gas flow of 50 L/min) via tracheostomy cannula in 14 tracheostomized subjects at high risk for weaning failure. The authors reported no difference in neuro-ventilatory drive as determined by electrical activity of the diaphragm, the pressure-time product of inspiratory muscles calculated from the electrical activity of the diaphragm, breathing frequency, and gas exchange between conventional O2 and HFT. The effect of HFT on inspiratory effort observed in our study and in the study by Stripoli et al19 contrasts with the expectation that HFT might alleviate inspiratory effort and breathing pattern in tracheostomized patients. Physiological studies in subjects with acute hypoxemic respiratory failure reported significant reduction in inspiratory effort with HFNC.12,13,26,27 The physiologic benefit of HFNC to reduce inspiratory effort can be explained by mechanisms not present in tracheostomized patients, such as generation of positive airway pressure by high flow of gas, alteration of airway resistance, and washing out of the oropharyngeal dead space.28–30 Bypassing the normal respiratory passage with tracheostomy may diminish the physiologic effects of HFT compared to HFNC.31 Natalini et al20 evaluated the effect of high-flow oxygen therapy via tracheostomy with different flows (10, 30, and 50 L/min) compared to standard oxygen in 26 tracheostomized subjects. They found a small increase in peak and mean expiratory pressure with HFT, and HFT at a flow of 50 L/min was needed to increase the peak tracheal expiratory pressure to 1.8 cm H2O. Moreover, compared to HFT, Natalini et al20 reported significantly higher peak tracheal expiratory pressure with HFNC in 5 subjects who underwent tracheostomy decannulation (1.8 vs 5.1 cm H2O, respectively). The findings from that study support the different physiologic effect of HFT on positive airway pressure from HFNC. In addition, the dedicated HFT connector to the tracheostomy tube, which has a large outlet for exhaled air, may also affect the physiologic change as compared to the narrow space surrounding the nostrils when using HFNC. Moreover, the high flow of gas might not reach deeper into the tracheal lumen because of flow delivery outside of the trachea through a large outlet of tracheostomy interface. However, some patients might benefit from the effect of heat and humidification that may improve patient comfort and alleviate inspiratory effort, thus it should be tested in the future studies.
, but no differences in breathing frequency, end-tidal CO2, end-expiratory lung volume, or heart rate between the 2 groups. The duration of each intervention was short (ie, only 20 min), and the effect on inspiratory effort was not investigated. Our findings are consistent with a recent prospective crossover study by Stripoli et al,19 who compared conventional O2 via T-tube at a flow of 10 L/min to HFT with a gas flow of 50 L/min) via tracheostomy cannula in 14 tracheostomized subjects at high risk for weaning failure. The authors reported no difference in neuro-ventilatory drive as determined by electrical activity of the diaphragm, the pressure-time product of inspiratory muscles calculated from the electrical activity of the diaphragm, breathing frequency, and gas exchange between conventional O2 and HFT. The effect of HFT on inspiratory effort observed in our study and in the study by Stripoli et al19 contrasts with the expectation that HFT might alleviate inspiratory effort and breathing pattern in tracheostomized patients. Physiological studies in subjects with acute hypoxemic respiratory failure reported significant reduction in inspiratory effort with HFNC.12,13,26,27 The physiologic benefit of HFNC to reduce inspiratory effort can be explained by mechanisms not present in tracheostomized patients, such as generation of positive airway pressure by high flow of gas, alteration of airway resistance, and washing out of the oropharyngeal dead space.28–30 Bypassing the normal respiratory passage with tracheostomy may diminish the physiologic effects of HFT compared to HFNC.31 Natalini et al20 evaluated the effect of high-flow oxygen therapy via tracheostomy with different flows (10, 30, and 50 L/min) compared to standard oxygen in 26 tracheostomized subjects. They found a small increase in peak and mean expiratory pressure with HFT, and HFT at a flow of 50 L/min was needed to increase the peak tracheal expiratory pressure to 1.8 cm H2O. Moreover, compared to HFT, Natalini et al20 reported significantly higher peak tracheal expiratory pressure with HFNC in 5 subjects who underwent tracheostomy decannulation (1.8 vs 5.1 cm H2O, respectively). The findings from that study support the different physiologic effect of HFT on positive airway pressure from HFNC. In addition, the dedicated HFT connector to the tracheostomy tube, which has a large outlet for exhaled air, may also affect the physiologic change as compared to the narrow space surrounding the nostrils when using HFNC. Moreover, the high flow of gas might not reach deeper into the tracheal lumen because of flow delivery outside of the trachea through a large outlet of tracheostomy interface. However, some patients might benefit from the effect of heat and humidification that may improve patient comfort and alleviate inspiratory effort, thus it should be tested in the future studies.
We noted a significant increase in breathing frequency from PSV to noninvasive respiratory support. In addition, there was a trend toward increased breathing frequency between conventional O2 via T-tube and HFT, but the difference was not statistically significant. This finding was similar to previous studies, but comparison with the baseline value has not been reported.18,19 In contrast, we observed lower  with HFT compared to conventional O2. This discordance might be explained by the higher
with HFT compared to conventional O2. This discordance might be explained by the higher  in the conventional O2 group because we used a fixed flow of oxygen via T-tube; however, this difference might not be clinically important.
in the conventional O2 group because we used a fixed flow of oxygen via T-tube; however, this difference might not be clinically important.
Our study has limitations. First, the duration of each intervention was short. Second, we did not measure  during conventional O2 via T-tube due to technical limitations; therefore actual
during conventional O2 via T-tube due to technical limitations; therefore actual  secondary to room air entrainment cannot be reliably concluded. Third, the simple eligibility criteria for inclusion in our study facilitated the enrollment of a diverse study population; however, our randomized crossover design may compensate for this limitation. Finally, this study was designed to evaluate the physiologic effects of HFT via tracheostomy, and there was no focus on clinical outcomes. Future study is needed to elucidate the clinical effects of HFT via tracheostomy.
secondary to room air entrainment cannot be reliably concluded. Third, the simple eligibility criteria for inclusion in our study facilitated the enrollment of a diverse study population; however, our randomized crossover design may compensate for this limitation. Finally, this study was designed to evaluate the physiologic effects of HFT via tracheostomy, and there was no focus on clinical outcomes. Future study is needed to elucidate the clinical effects of HFT via tracheostomy.
Conclusions
Inspiratory effort and breathing frequency significantly increase during unassisted breathing in tracheostomized subjects compared to those treated with PSV. HFT provides no measurable additional benefit on inspiratory effort as determined by sPTPes, breathing pattern, and hemodynamics compared to conventional O2 via T-tube.
sPTPes, Pes Swing, Respiratory Variables, and Hemodynamic Variables During Ventilation
Acknowledgments
The authors thank Pattranan Vaidyakula (Division of Respiratory Diseases and Tuberculosis, Department of Medicine, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand) for her assistance in identifying and recruiting the subjects; as well as Khemajira Karaketklang (Department of Medicine, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand) and Suthipol Udompunthurak (Clinical Epidemiology Unit, Research Department, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand) for their assistance with statistical analysis.
Footnotes
- Correspondence: Nuttapol Rittayamai MD, Division of Respiratory Diseases and Tuberculosis, Department of Medicine, Faculty of Medicine Siriraj Hospital, Mahidol University, 2 Prannok Road, Siriraj, Bangkoknoi, Bangkok 10700, Thailand. E-mail: nuttapol.rit{at}mahidol.ac.th
This study was supported by the Faculty of Medicine Siriraj Hospital, Mahidol University (grant [IO]R016131048). Dr Brochard has disclosed relationships with Covidien, Air Liquide, Philips, Sentec, Fisher & Paykel, and GE Healthcare. The other authors have disclosed no conflicts of interest.
- Copyright © 2021 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}
{kind=link}