

Abstract
BACKGROUND: Until now, transfusion-related acute lung injury (TRALI) has been considered the leading cause of blood transfusion-related diseases and death. In addition, there is no clinically effective treatment plan for TRALI. The aim of this study was to systematically summarize the literature on risk factors for TRALI in critical patients.
METHODS: Electronic searches (up to March 2020) were performed in the Cochrane Library, Web of Knowledge, Embase, and PubMed databases. We included studies reporting on the risk factors of TRALI for critical patients and extracted risk factors. A total of 13 studies met the inclusion criteria.
RESULTS: We summarized and analyzed the potential risk factors of TRALI for critical patients in 13 existing studies. Host-related factors were age (odds ratio [OR] 1.16 [95% CI 1.08–1.24]), female sex (OR 1.26 [95% CI 1.16–1.38]), tobacco use status (OR 3.82 [95% CI 1.91–7.65]), chronic alcohol abuse (OR 3.82 [95% CI 2.97–26.83]), positive fluid balance (OR 1.24 [95% CI 1.08-1.42]), shock before transfusion (OR 4.41 [95% CI 2.38–8.20]), and American Society of Anesthesiologists (ASA) score of the recipients (OR 2.72 [95% CI 1.43–5.16]). The transfusion-related factors were the number of transfusions (OR 1.40 [95% CI 1.14–1.72]) and units of fresh frozen plasma (OR 1.21 [95% CI 1.01–1.46]). The device-related factor was mechanical ventilation (OR 4.13 [95% CI 2.20–7.76]).
CONCLUSIONS: The risk factors that were positively correlated with TRALI in this study included number of transfusions and units of fresh frozen plasma. Age, female sex, tobacco use, chronic alcohol abuse, positive fluid balance, shock before transfusion, ASA score, and mechanical ventilation may be potential risk factors for TRALI. Our results suggest that host-related risk factors may play a more important role in the occurrence and development of TRALI than risk factors related to blood transfusions.
Introduction
Many severely injured patients often suffer from hemorrhagic shock, requiring transfusion therapy. However, blood transfusion is a double-edged sword. Transfusion-related acute lung injury (TRALI) that occasionally occurs during blood transfusion can be life-threatening.1,2 TRALI has been the leading cause of transfusion-related deaths since 2003, according to the United States Food and Drug Administration.3
According to the standardized definition of TRALI, based on the consensus conference of the Canadian Blood Services (CBS) in 2004, TRALI was defined as respiratory distress and acute lung injury that develops during blood transfusion or within 6 h after blood transfusion, manifested as acute hypoxemia and non-cardiogenic pulmonary edema in the absence of other risk factors for acute lung injury.4-6 TRALI has traditionally been considered to be a combination of 2 events. The first event is the inflammatory state of the recipient, which leads to the activation of neutrophils in the lungs. The second event is further activation of neutrophils caused by biologically active lipids or sensitizing antibodies contained in blood products, with subsequent pulmonary leakage.7-9 TRALI is particularly evident in critically ill patients because most of them have different degrees of inflammation, so it is very easy to trigger the activation of neutrophils. This 2-event model of TRALI may explain the high incidence rate of TRALI in this population.10,11
Until now, TRALI has been considered the leading cause of blood transfusion-related diseases and death.12-14 Generally, the incidence of TRALI varies between 0.08% and 15%.15 The mortality rate of TRALI ranges between 5% and 14%.16-18 This wide difference may be due to the lack of a unified standard definition of TRALI and differences in research design. TRALI is often underestimated and underreported.19,20 Similar to acute lung injury/ARDS, supportive care measures and restrictive blood transfusion policies are mainly adopted in cases of TRALI because there is no clinically effective treatment plan.6
By clarifying the risk factors of a disease and their significance, it is possible to put forward practical and effective intervention strategies to prevent the occurrence and development of that disease.21 Some previous retrospective studies have attempted to identify risk factors associated with TRALI in critically ill patients. Prior studies have reported that routine exclusion of fresh frozen plasma from the blood of female blood donors can reduce the incidence of TRALI.22,23 There was also evidence that cardiac surgery increased the risk of TRALI.7,9 However, most of these studies were limited because they had a retrospective study design, single-center design, and examined one or several variables. The sample size of some studies was also relatively small, and it was difficult to obtain statistically significant results.18,24-28 To solve these problems, we performed a systematic review and meta-analysis of risk factors related to TRALI in critically ill patients.
Methods
Two reviewers (LYH and BLW) independently conducted systematic literature searches of the Cochrane Library, Web of Knowledge, Embase, and PubMed databases from inception up to March 2020 according to the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) guidelines. The following search terms were used: (blood transfusion* or transfusion reaction*) and (acute respiratory distress syndrome* or acute lung injury*) and (risk or predict*). The references of relevant articles were searched to find other relevant researches. There were no restrictions on year of publication. The detailed literature search strategy can be found in the supplementary materials (available at http://www.rcjournal.com).
The studies had to meet the following inclusion criteria: (1) all subjects were admitted to the ICU and received blood transfusion therapy; (2) provided clear definition and diagnosis according to the international definition of TRALI developed by the American-European Consensus Conference in 2004; (3) examined ≥ 1 indicators of the risk of TRALI; (4) examined potential risk factors for TRALI that have been previously examined by ≥ 2 studies, and (5) published in English. Both prospective and retrospective studies were considered eligible. Overlapping studies were included in this systematic review only after studying the different risk factors. Reviews and case reports were excluded.
The following data were independently extracted by 2 reviewers (LYH and BLW): first author, study design, year of study, country of study, definition of TRALI, study population characteristics, types of blood transfusion products, risk factors, and indexes representing clinical outcomes. Differences between the authors were resolved by consensus at a meeting. When the research data were not fully available, the corresponding author was contacted to request more information via email.
Two reviewers (LYH and BLW) used the Newcastle-Ottawa Scale to independently assess the quality of the research in this meta-analysis.29 The scale has the following 3 columns: quality of selection (3 items, 3 points), comparability (3 items, 3 points), and assessment of outcome (3 items, 3 points). A total score of 9 points can be obtained. Studies with scores of 1–3 were classified as low-quality literature, and studies with scores of 4–6 were classified as medium-quality literature; studies with scores of 7–9 were considered high-quality literature.30 Differences arising in the scoring process were resolved through a discussion until consensus was reached.
After extracting the data, the basic information of subjects who received blood transfusions and the important risk factors of TRALI identified in the individual studies were integrated. Review Manager 5.1 (Cochrane, London, United Kingdom) and Stata 11.0 (StataCorp, College Station, Texas) were used for the meta-analysis and analysis of the risk factors related to TRALI, respectively. Continuous variables were analyzed by calculating the weighted average difference and 95% CIs. Odds ratios (ORs) and 95% CI were used to analyze the categorical variables. Quantitative meta-analysis of factors detected in ≥ 2 studies was performed. The Cochrane I2 index and Q test P value were used to assess the heterogeneity across included studies. Fixed-effect models and random-effect models were used to analyze and calculate the overall effects. I2 values > 50% indicated significant heterogeneity, and the random-effect model was applied, which used the DerSimonian and Laird estimate. When no statistical heterogeneity was detected, a fixed-effect model was used. Egger regression asymmetry test and Begg funnel plot method were used to evaluate publication bias. If the funnel plot was visually symmetrical or P > .05, it indicated no publication bias. All statistical tests were 2-sided, with P values < .05 indicating statistical significance.
Results
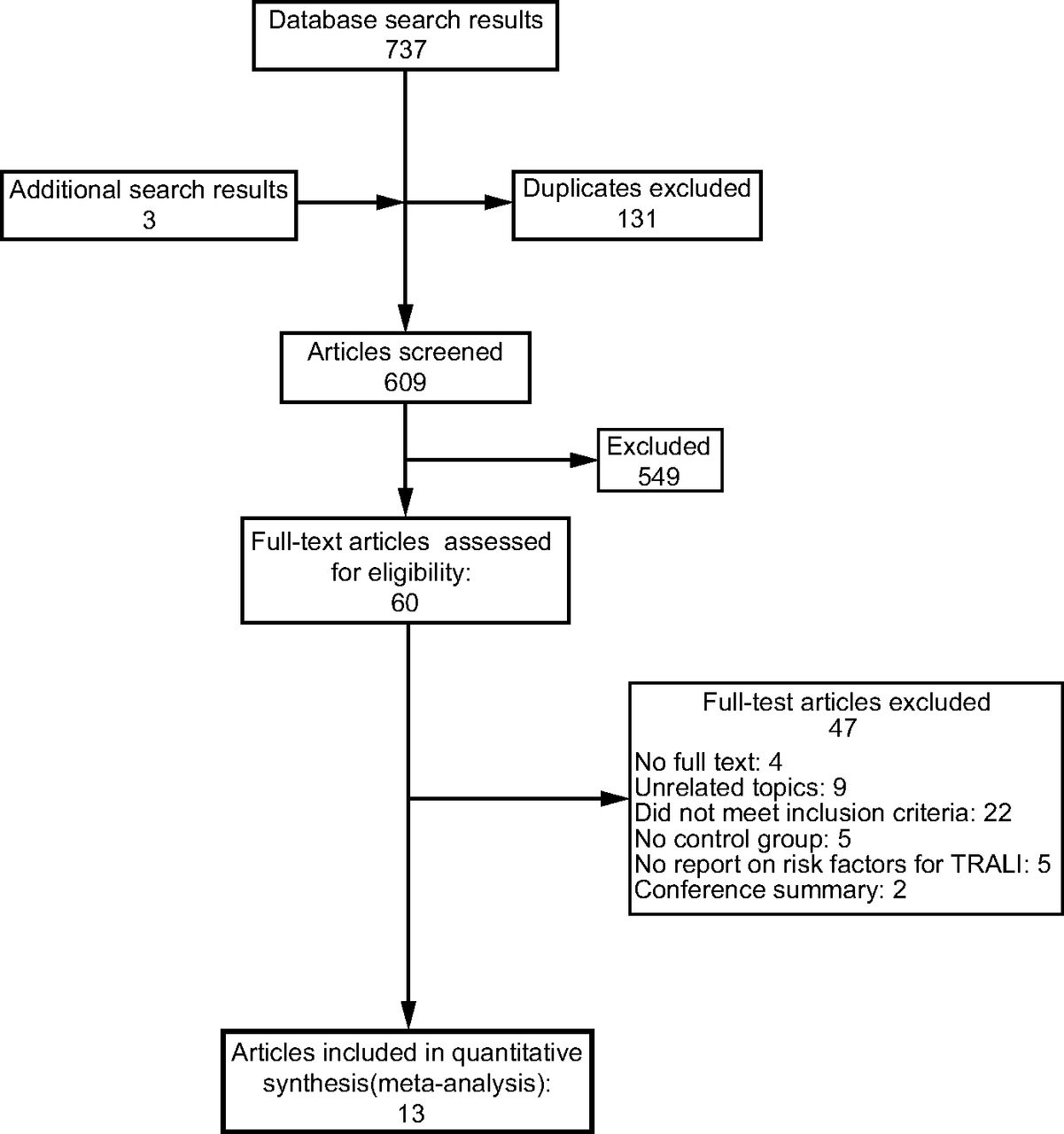
We retrieved 800 potentially relevant documents from PubMed (no. = 81), Embase (no. = 244), Web of Science (no. = 324), Cochrane Library (no. = 88), or via manual search (no. = 3). After combining and deleting duplicate documents, 609 studies were retained. According to the title and abstract, preliminary screening was conducted to further exclude 549 articles. Subsequently, we obtained the full text of the remaining 60 articles and screened them by reading. Four of these studies were excluded because they did not provide access to the full text; 9 studies were not relevant to our theme. The inclusion and exclusion criteria of the research groups of 22 studies did not meet the conditions we defined. Furthermore, 5 studies did not establish a control group, 5 studies did not report on TRALI-related risk factors, and 2 studies were conference summaries. Finally, we included 13 articles in the meta-analysis. The details of the screening are shown in Figure 1.
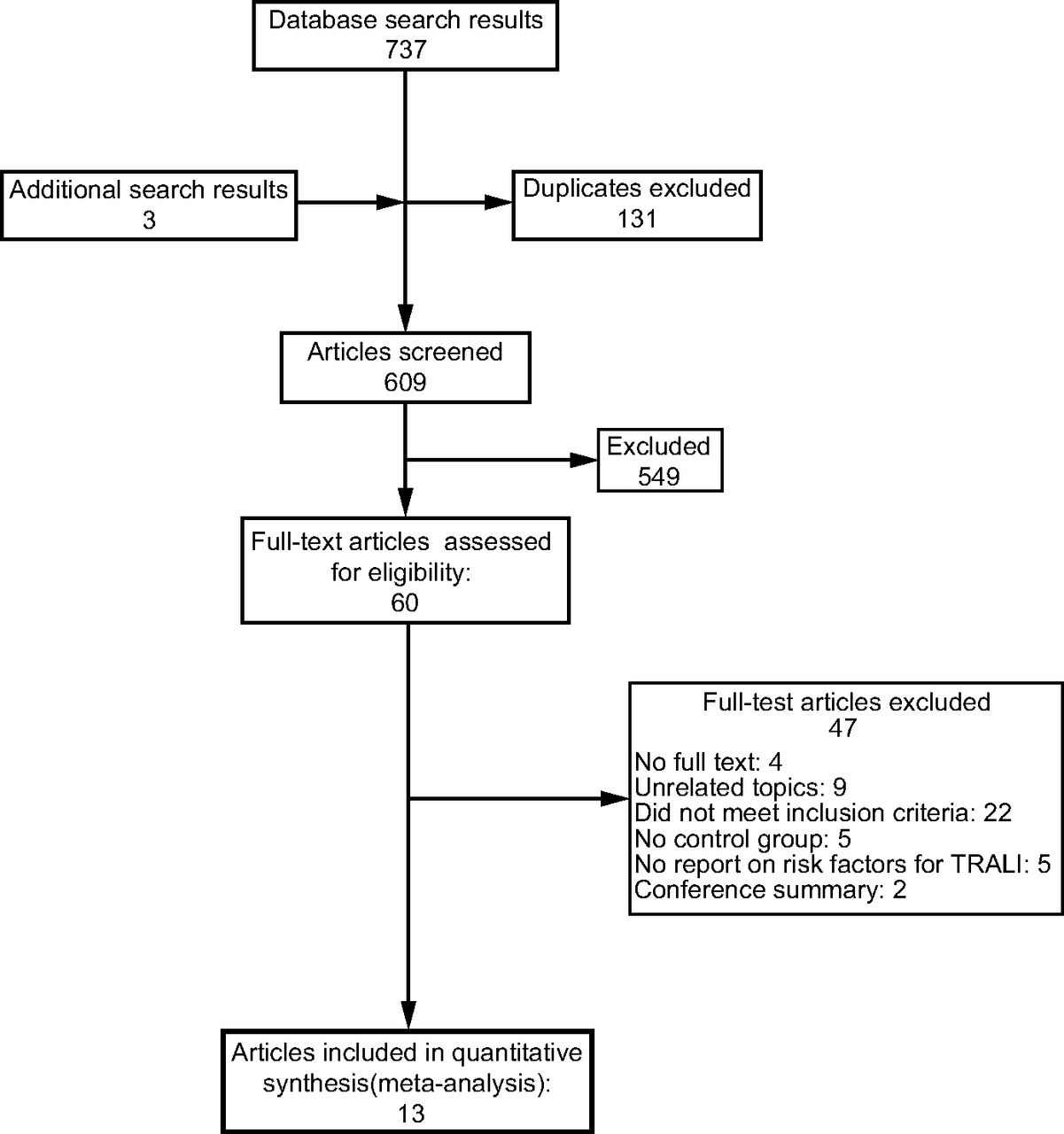
Flow chart. TRALI = transfusion-related acute lung injury.
The 13 articles included in this study included a total of 11,380,242 subjects: 3,179 case subjects and 11,377,063 control subjects. These studies were published between 2004 and 2015. The research subjects originated 4 countries: the United States, The Netherlands, Croatia, and Italy. The sample sizes varied from 26 to 11,378,264. Three articles were multicenter studies, and all 13 studies were case-control studies. We used the Newcastle-Ottawa Scale to assess the quality of each study. Three studies scored 7 points, 8 studies scored 8 points, and 2 studies scored 9 points. Quality assessments indicated that all included studies had high quality. Table 1 and Supplementary Table E2 (available at http://www.rcjournal.com) show the basic characteristics of all included studies and the Newcastle-Ottawa Scale scoring results.
Characteristics of Included Studies
The current meta-analysis summarizes 20 potential risk factors from 4 aspects that have been reported in ≥ 2 studies: host-related, blood transfusion-related, device-related, and surgery-related factors (see Supplementary Table E3 at http://www.rcjournal.com). The risk factors, which have been reported in ≥ 5 studies, have been closely related to the occurrence and development of TRALI. Figure 2 and Figure 3 show the forest plots of these TRALI risk factors (P < .05). Other forest plots of factors (P < .05) are shown in Supplementary Figure E1 (available at http://www.rcjournal.com). Forest plots results of other risk factors (P > .05) are shown in Table 2.

Forest plots of amount of transfusions for TRALI with data available in 7 studies. TRALI = transfusion-related acute lung injury; OR = odds ratio; D+L = random-effect model; I-V = fixed-effect model.
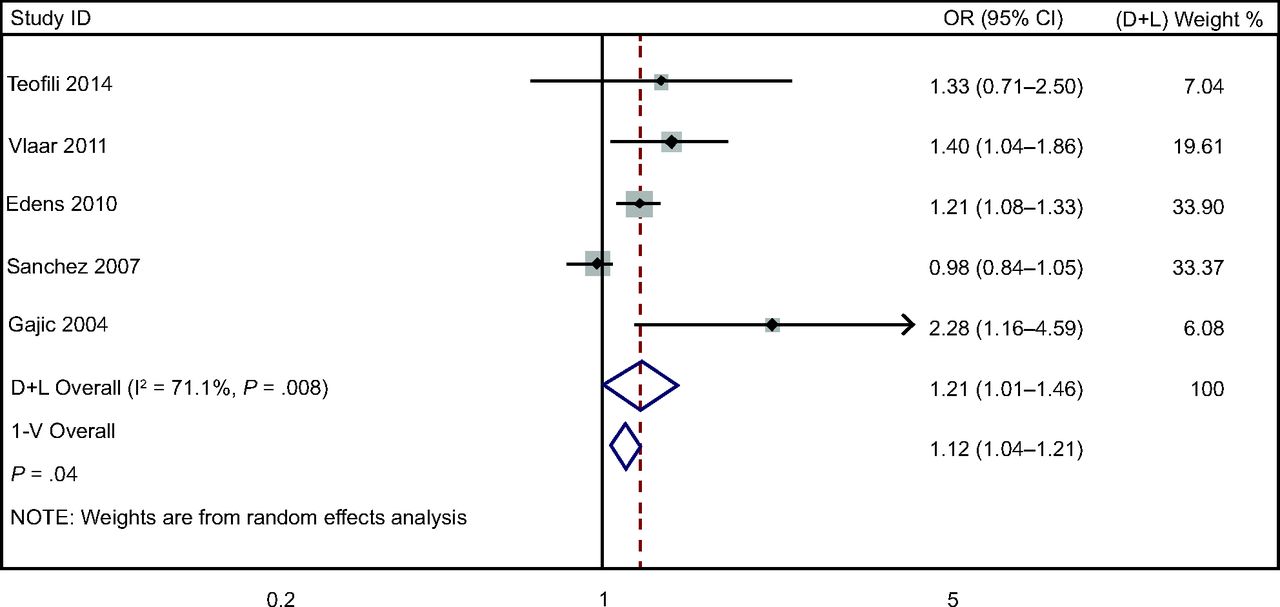
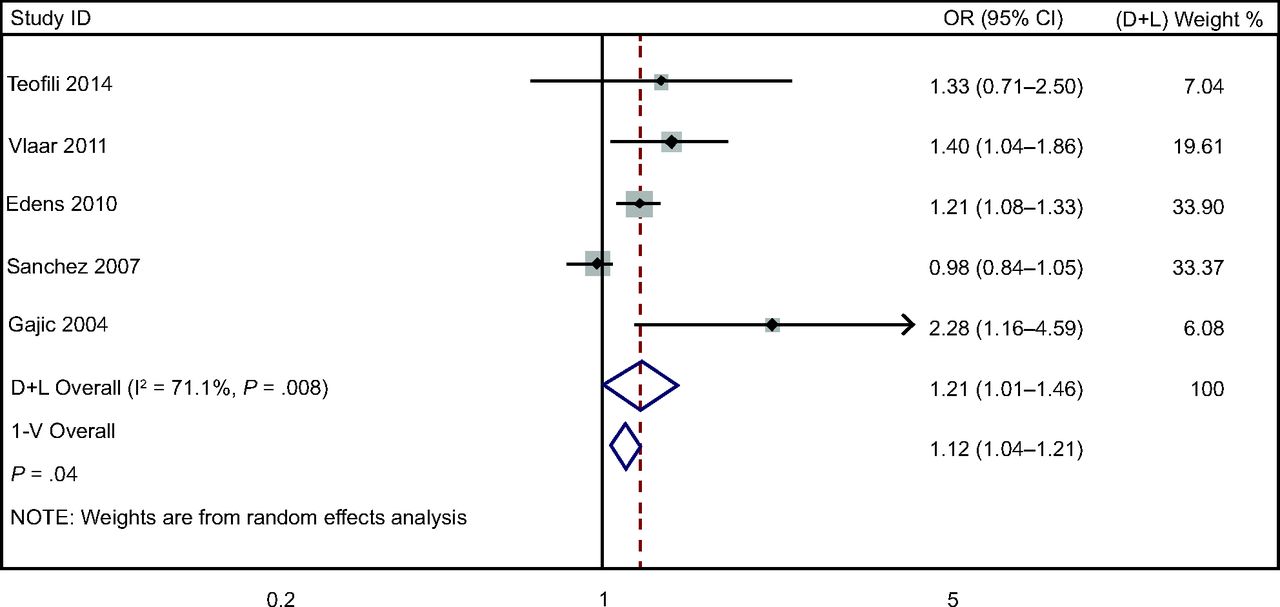
Forest plots of fresh frozen plasma units for TRALI with data available in 5 studies. TRALI = transfusion-related acute lung injury; OR = odds ratio; D+L = random-effect model; I-V = fixed-effect model.
Other Results of Forest Plots of Risk Factors for TRALI
Host-Related Factors
For the host-related factors, some factors were potentially related to the occurrence of TRALI: age (2 studies, 11,378,312 subjects; fixed-effect model, I2 = 15.9%; OR 1.16 [95% CI 1.08–1.24], P < 0.01); female sex (2 studies, 11,378,290 subjects; fixed-effect model, I2 = 0%; OR 1.26 [95% CI 1.16–1.38], P < 0.01); tobacco use (3 studies, 11,378,825 subjects; fixed-effect model, I2 = 0%; OR 3.82 [95% CI 1.91–7.65], P < 0.01); chronic alcohol abuse (2 studies, 561 subjects; fixed-effect model, I2 = 0%; OR 3.82 [95% CI 2.97–26.83], P < 0.01); positive fluid balance (2 studies, 561 subjects; random-effect model, I2 = 71.3%; OR 1.24 [95% CI 1.08–1.42], P < 0.01); shock before transfusion (2 studies, 561 subjects; fixed-effect model, I2 = 0%; OR 4.41 [95% CI 2.38–8.20], P < 0.01); and American Society of Anesthesiologists (ASA) score (2 studies, 300 subjects; fixed-effect model, I2 = 0%; OR 2.72 [95% CI 1.43–5.16], P < 0.01) (see Supplementary Fig. 1A–G, available at http://www.rcjournal.com). Some factors were not associated with the occurrence of TRALI (ie, P > .05): tidal volume (2 studies; 248 subjects; random-effect model, I2 = 52.2%; OR 1.37 [95% CI 0.89–2.11], P = .16); liver disease (2 studies, 505 subjects; random-effect model, I2 = 85.5%; OR 1.51 [95% CI 0.48–4.78], P = .48); sepsis (3 studies, 11,378,786 subjects; random-effect model, I2 = 93.9%; OR 2.08 [95% CI 0.46–9.28], P = .34); and hematology-oncology (3 studies, 11,378,543 subjects; random-effect model, I2 = 87.9%; OR 1.40 [95% CI 0.25–7.80], P = .70) (Table 2).
Transfusion-Related Factors
Some transfusion-related factors were related to the occurrence of TRALI: number of transfusions (7 studies, 976 subjects; random-effect model, I2 = 77.4%; OR 1.40 [95% CI 1.14–1.72], P < .01) (Fig. 2); units of fresh frozen plasma (5 studies, 393 subjects; random-effect model, I2 = 71.1%; OR 1.21 [95% CI 1.01–1.46], P = .04) (Fig. 3); and mechanical ventilation (3 studies, 775 subjects; fixed-effect model, I2 = 0%; OR 4.13 [95% CI 2.20–7.76], P < .01) (Supplementary Fig. 1H; available at http://www.rcjournal.com). Some factors were not associated with the occurrence of TRALI (ie, P > .05): blood products from female donors (4 studies, 553 subjects; fixed-effect model, I2 = 20.0%; OR 1.09 [95% CI 0.94–1.27], P = .32); red blood cell units (5 studies, 519 subjects; random-effect model, I2 = 58.8%; OR 0.97 [95% CI 0.72–1.31], P = .86); platelet units (5 studies, 11,378,475 subjects; random-effect model, I2 = 69.6%; OR 1.38 [95% CI 0.27–1.26], P = .16); and pump time during cardiopulmonary bypass (2 studies, 300 subjects; random-effect model, I2 = 95.6%; OR 1.04 [95% CI 0.96–1.12], P = .33) (Table 2).
Procedure-Related Factors
Neither of the following procedure-related factors associated with the occurrence of TRALI (ie, P > .05): surgical intervention (2 studies, 97 subjects; fixed-effect model, I2 = 0%; OR 1.21 [95% CI 0.17–8.63], P = .85); and liver transplantation (3 studies, 587 subjects; fixed-effect model, I2 = 15.1%; OR 2.95 [95% CI 0.80–10.84], P = .19) (Table 2).
Publication Bias
We used the Begg funnel plot and Egger linear regression test to evaluate the publication bias in these studies (Supplementary Table E4 available at http://www.rcjournal.com). Because each factor was generally included in a few studies, we only conducted a bias test for risk factors that were included in > 3 studies. Among the factors that had a significant correlation with the occurrence of TRALI, the number of transfusions had some publication bias, whereas the number of fresh frozen plasma units did not. Among the factors that were not significantly related to TRALI, there was no publication bias for blood products from female donors and number of red blood cell units and platelet units (Supplementary Fig. 2 available at http://www.rcjournal.com). Because the number of studies included was small, we did not conduct a sensitivity analysis.
Discussion
To our knowledge, this is the first meta-analysis of risk factors of TRALI in critically ill patients. We summarized and analyzed the potential risk factors of TRALI for critical patients in 13 studies. The number of transfusions and units of fresh frozen plasma were risk factors related to blood transfusion. Age, female sex, tobacco use, chronic alcohol abuse, positive fluid balance, shock before transfusion, ASA score, and mechanical ventilation may be potential risk factors for TRALI, although < 5 studies were included. More studies are expected to be included for analysis. Tidal volume, liver disease, sepsis, blood tumor disease, blood products from female blood donors, red blood cell units, platelet units, pumping time during extracorporeal circulation, surgery, and liver transplantation were not identified as risk factors of TRALI. Some of these conclusions seem to be logical, but our research findings strengthen previous evidence. However, some evidence was contrary to previous conclusions.
In 1951, Barnard31 reported that a patient with acute leukemia died because of the acute lung reaction caused by an allergic reaction to blood transfusion, which was the first report of lung injury due to blood transfusion. After that, several scientists reported similar cases. Until the 1980s, TRALI was officially recognized as an independent disease.32 In 2004, the consensus meeting held by the CBS Agency standardized 2 entities for the first time: TRALI and possible TRALI (pTRALI), in which the cause of acute lung injury is not clear (ie, it could be ARDS or blood transfusion).3,33 In 2005, the definition of the CBS was expanded to include patients with acute lung injury deterioration due to blood transfusion, and physicians were expected to determine whether a patient had TRALI or ARDS according to clinical standards and judgments.33 In 2019, researchers used the Delphi Methodology to re-classify TRALI into 2 types: TRALI I (without risk factors of ARDS) and TRALI II (with risk factors of ARDS or existing mild ARDS).34,35 In the 14 years after the CBS published the guideline, a large amount of information from prospective and retrospective research related to TRALI has been accumulated. A careful reading of the literature will show that previous definitions have not been strictly applied, and there is a large degree of heterogeneity in the incidence rates and mortality rates. In conclusion, there are several problems with the current body of evidence. First, the clinical manifestations and laboratory tests of TRALI were not independent pathological features, so it was difficult to differentiate diagnosis; in addition, the tools to perform the diagnostic analysis were not extensive enough.36 Second, except for the measurement of blood oxygen saturation ( ), there was no objective laboratory test in the diagnostic criteria, so the diagnosis was rather subjective.2 Next, some previous studies indicate that the risk factors of ARDS and TRALI may be similar, and some host-related factors were positively correlated with ARDS, such as mechanical ventilation, tobacco use, age, and shock. These led to unclear taxonomic boundaries between TRALI and ARDS and made it almost impossible to distinguish TRALI from other acute lung injuries in clinical practice.34 Finally, according to the definition, TRALI appears temporarily within 6 h after blood transfusion, but a few cases have been reported to occur between 6 h and 48 h after blood transfusion, emphasizing the need for a standardized definition of TRALI.37 To date, although there is a relatively large number of studies on TRALI, the inclusion criteria for the TRALI population were not uniform among the studies; in addition, the sample size in some studies is relatively small, the pathogenesis is unclear, and the research results are different.
), there was no objective laboratory test in the diagnostic criteria, so the diagnosis was rather subjective.2 Next, some previous studies indicate that the risk factors of ARDS and TRALI may be similar, and some host-related factors were positively correlated with ARDS, such as mechanical ventilation, tobacco use, age, and shock. These led to unclear taxonomic boundaries between TRALI and ARDS and made it almost impossible to distinguish TRALI from other acute lung injuries in clinical practice.34 Finally, according to the definition, TRALI appears temporarily within 6 h after blood transfusion, but a few cases have been reported to occur between 6 h and 48 h after blood transfusion, emphasizing the need for a standardized definition of TRALI.37 To date, although there is a relatively large number of studies on TRALI, the inclusion criteria for the TRALI population were not uniform among the studies; in addition, the sample size in some studies is relatively small, the pathogenesis is unclear, and the research results are different.
Because the diagnostic criteria of TRALI in previous studies are not uniform, and to understand the risk factors of TRALI comprehensively, this study included studies on TRALI and pTRALI as per the definition of the CBS. According to the Berlin standard published in 2012, the term “acute lung injury” has been eliminated, and, according to the degree of hypoxia, ARDS was divided into mild, moderate, and severe.35 For this reason, we also included cases of transfusion-related ARDS in the case group.
In terms of host-related risk factors, our results indicate that as patients aged, the risk of TRALI increased. Some studies have reported that most subjects in the elderly population exhibited chronic low-grade inflammation, which is manifested by high baseline levels of pro-inflammatory cytokines in the body, which are likely to cause TRALI.38 In addition, women who receive blood transfusions are more likely than men to develop TRALI. Previous studies have reported that human leukocyte antigen I (HLA I), HLA II, and granulocyte antibodies are common in women who have given birth. When these antibodies encounter homologous antigens from the transfusion plasma, it can lead to neutrophil activation and oxidative substance release, which can damage the lung endothelium.39,40 This shows that previous pregnancy experience is a very important factor leading to TRALI. Chronic alcohol abuse may also increase the risk, possibly because the level of glutathione, an antioxidant in the lungs, decreases, which in turn reduces the phagocytic function of the apoptotic cells, resulting in increased inflammation in the lungs.27 Patients with a history of smoking have varying degrees of respiratory problems, which may increase the risk of disease.41 Shock can cause tissue damage and may induce TRALI by activating the patient's neutrophils.34 The ASA score reflects the physical condition of the patient, and a high score may increase the risk of illness.42
In terms of transfusion-related factors, our results indicate that the amount of transfusion and number of fresh frozen plasma units were significantly related to the occurrence of TRALI, while female sex of the donors and number of red blood cell units and platelet units did not seem to significantly increase the risk of TRALI. Since 2003, the British government mandated that female plasma be used in manufacturing to reduce the incidence of TRALI. Since the implementation of this approach, the number of TRALI cases in the United Kingdom has indeed decreased.18 The only test that can be used to diagnose TRALI is to monitor the content of HLA and granulocyte antibodies in the plasma of the recipient or donor. The principle is that the relevant antigens and antibodies contained in the donor and recipient will induce related inflammatory reactions, which will lead to lung injury. The discovery of antigen-antibody reactions strongly supports the diagnosis of TRALI. However, in one study, we did not find consistency between antigens and antibodies in 15% of TRALI cases, suggesting that a simple antigen-antibody reaction does not necessarily lead to clinical TRALI.43 In a retrospective study, Toy et al44 investigated a group of female donors with a history of pregnancy and had multiple antibodies related to HLA antigens. TRALI did not occur when the donated blood was transfused to 55 subjects with non-neutropenia of known HLA type.44 In this regard, some researchers believe that the occurrence of TRALI may require 2 different events: one related to the clinical situation of the recipient (such as active infection), and the other related to the infusion of blood products containing HLA antibodies, granulocyte antibodies, or other biological response regulators.43
In this study, we found that most host-related risk factors are characterized by a pro-inflammatory state, which may stimulate lung neutrophils as the “first attack” in the development of TRALI.45 Therefore, the clinical state of the host may lead to a decrease in lung compliance before blood transfusion, as well as a deterioration in lung compliance after blood transfusion, which may lead to lung injury.46 More studies indicate that host-related risk factors may play a more critical role in the development of TRALI than transfusion-related risk factors. This conclusion highlights the importance of the “first attack” mentioned above.9
In terms of device-related risk factors, our results indicate that mechanical ventilation may be related to the occurrence of TRALI. A previous study reported that mechanical ventilation accelerates and aggravates lung injury.47 When the peak airway pressure is > 30 cm H2O, the risk of acute lung injury increases significantly.48,49 The above conclusions suggest that mechanical ventilation also plays an important role in triggering TRALI in the early stage and a synergistic role in the later stage with blood transfusion in the development of lung injury.
In terms of the mitigation strategies for disease prevention, through the analysis and summary of the included studies, we have drawn the following conclusions. First, in the future, it is necessary to have a more reasonable definition and classification of TRALI. Previous studies have reported that TRALI and pTRALI seem to have different etiologies, strategies, and clinical outcomes.27 For TRALI, a restrictive transfusion policy was still strongly recommended.6 Compared with TRALI, ARDS risk factors and not blood transfusion risk factors were important driving factors of clinical outcomes in patients with pTRALI.27 In the future, we need to further study the role of blood transfusion in the pathophysiology of pTRALI, and more rigorous prospective studies are needed for these patients. Second, many studies have shown the importance of host-related factors in the prevention of TRALI. For patients in poor condition, doctors may need to reconsider the restrictive transfusion policy.13 Studies have noted that, in critically ill patients, even if the restrictive transfusion strategy was well implemented, it may also lead to the occurrence of TRALI.2 According to the 2 events model, most critical patients are characterized by a pro-inflammatory state, which plays an important role in the pathogenesis of TRALI, stimulating pulmonary neutrophils and acting as a “first event” in the occurrence of TRALI. The severity of their condition may contribute to a lower threshold to develop TRALI.7-9 It is suggested that for patients in better condition, the mitigation strategy is biased in favor of the restrictive transfusion policy, but for patients in poor condition, the mitigation strategy may be biased in favor of the control of host-related factors.
Our study has some advantages and limitations. By formulating a systematic research plan, a comprehensive search strategy, and strict inclusion and exclusion criteria, as well as by evaluating the research quality, the objectivity and consistency of this study can be considered high. The findings could help both clinicians and patients interpret the current evidence.
Although the research is innovative, some limitations should be recognized. First, the majority of the studies included in the analysis were retrospective studies, and the diversity and complexity of TRALI-related influencing factors were affected to a certain extent by selection bias. Second, there were very few studies on some risk factors. In this case, the power of these factors is too weak to find a significant association with a relatively small impact. We believe that as the number of powerful cohort studies increases, clearer and higher levels of evidence will become available. Third, because some data are lacking (such as APACHE II scores), some potential risk factors could not be analyzed in groups. Finally, because the diagnostic criteria of TRALI have not been completely unified, there is variability in the diagnosis of TRALI in some studies. In this regard, we formulated the inclusion criteria for meta-analysis according to the needs of this study to provide guidance for clinicians as soon as possible.
Conclusions
TRALI is considered the main cause of blood transfusion-related illness and death in critically ill patients. The number of transfusions and the number of units of fresh frozen plasma were risk factors for TRALI. Age, female sex, tobacco use, chronic alcohol abuse, positive fluid balance, shock before transfusion, ASA score, and mechanical ventilation may be potential risk factors for TRALI, although fewer than 5 studies were included. This review suggests that host-related risk factors may play a more important role in the occurrence and development of TRALI than risk factors related to blood transfusions. More studies are expected to be included for analysis. Our findings may help clinicians formulate accurate and effective prevention and treatment strategies and provide appropriate and timely treatment. Furthermore, it is necessary to establish clear and unified diagnosis criteria for TRALI, to study the pathogenesis of TRALI, and to conduct studies with larger sample sizes on the prevalence and risk factors of TRALI.
Footnotes
- Correspondence: Zhaofan Xia. E-mail: xiazhaofan_smmu{at}163.com
Supplementary material related to this paper is available at http://www.rcjournal.com.
This work was supported by the National Natural Science Foundation of China (81930057, 81772076), CAMS Innovation Fund for Medical Sciences (2019-I2M-5-076), and Achievements Supportive Fund (2018-CGPZ-B03). The authors have disclosed no conflicts of interest.
- Copyright © 2021 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}