

Abstract
BACKGROUND: The assessment of diaphragmatic kinetics through tissue Doppler imaging (dTDI) was recently proposed as a means to describe diaphragmatic activity in both healthy individuals and intubated patients undergoing weaning from mechanical ventilation. Our primary aim was to investigate whether the diaphragmatic excursion velocity measured with dTDI at the end of a spontaneous breathing trial (SBT) was different in subjects successfully extubated versus those who passed the trial but exhibited extubation failure within 48 h after extubation.
METHODS: We enrolled 100 adult subjects, all of whom had successfully passed a 30-min SBT conducted in CPAP of 5 cm H2O. In cases of extubation failure within 48 h after liberation from invasive mechanical ventilation, subjects were re-intubated or supported through noninvasive ventilation. dTDI was performed at the end of the SBT to assess excursion, velocity, and acceleration.
RESULTS: Extubation was successful in 79 subjects, whereas it failed in 21 subjects. The median (interquartile range [IQR]) inspiratory peak excursion velocity (3.1 [IQR 2.0–4.3] vs 1.8 [1.3–2.6] cm/s, P < .001), mean velocity (1.6 [IQR 1.2–2.4] vs 1.1 [IQR 0.8–1.4] cm/s, P < .001), and acceleration (8.8 [IQR 5.0–17.8] vs 4.2 [IQR 2.4–8.0] cm/s2, P = .002) were all significantly higher in subjects who failed extubation compared with those who were successfully extubated. Similarly, the median expiratory peak relaxation velocity (2.6 [IQR 1.9–4.5] vs 1.8 [IQR 1.2–2.5] cm/s, P < .001), mean velocity (1.1 [IQR 0.7–1.7] vs 0.9 [IQR 0.6–1.0] cm/s, P = .002), and acceleration (11.2 [IQR 9.1–19.0] vs 7.1 [IQR 4.6–12.0] cm/s2, P = .004) were also higher in the subjects who failed extubation.
CONCLUSIONS: In our setting, at the end of SBT, subjects who developed extubation failure within 48 h after extubation experienced a greater diaphragmatic activation compared with subjects who were successfully extubated. (ClinicalTrials.gov registration NCT03962322.)
Introduction
Invasive mechanical ventilation is a lifesaving therapy in critically ill patients. After recovery from the acute phase of illness, a spontaneous breathing trial (SBT) is commonly performed to ascertain whether mechanical ventilation can be withdrawn and the patient extubated.1 The reported rates of extubation failure range between 10% and 25%, reflecting the variety in causes that may lead to failed extubation.2 Unfortunately, the failure of a planned extubation is associated with worse outcomes and increased mortality.3,4 Thus, identifying patients with a high risk for extubation failure is crucial for improving clinical outcome.
Several conditions are associated with extubation failure. The inability to manage tracheobronchial secretions, age > 65 y, and the presence of underlying chronic respiratory or cardiac disease are factors considered to increase the risk of extubation failure.2,5-11 Additional factors, such as mechanical ventilation ≥ 7 d, delirium, ICU-acquired paresis, acute heart dysfunction, increased rapid shallow breathing index (RSBI), and a positive fluid balance the day before extubation, have been demonstrated to increase the risk of extubation failure.4,12-15
Diaphragm ultrasound has been proposed as a technique capable of identifying patients more likely to experience extubation failure after passing an SBT; however, conflicting results have been reported.16-18 In addition, the diaphragmatic thickening fraction appears to be a less reliable method for quantifying (in healthy volunteers) diaphragmatic effort.19,20 Previous data suggest that the displacement velocity of the diaphragm correlates with the extent of muscle activity.21 Moreover, diaphragmatic tissue Doppler imaging (dTDI) has been recently employed to assess diaphragmatic activity, both in healthy volunteers and in subjects being weaned off invasive mechanical ventilation.22 However, the potential role of the diaphragmatic excursion kinetics variables (ie, velocity and acceleration) as predictors of extubation failure has never been investigated.
We designed this prospective observational study to test the hypothesis that the sonographic characteristics of diaphragmatic excursion kinetics (ie, velocity and acceleration) assessed through dTDI at the end of an SBT may be different in subjects who go on to be successfully extubated compared with those who exhibit extubation failure. Thus, our primary aim was to evaluate the velocities of diaphragmatic excursion and relaxation, assessed by means of dTDI at the end of the SBT, and to compare the values obtained in individuals successfully extubated with those of subjects exhibiting extubation failure within 48 h after withdrawal of invasive mechanical ventilation. Secondarily, we aimed to ascertain whether the variables assessed with dTDI can be used to predict extubation failure.
Quick look
Current Knowledge
Diaphragm ultrasound has been proposed as a technique capable of identifying patients more likely to experience extubation failure after passing a spontaneous breathing trial, though there are conflicting results. Diaphragmatic tissue Doppler imaging has been utilized recently to assess diaphragmatic activity, both in healthy volunteers and in individuals being weaned from invasive mechanical ventilation.
What This Paper Contributes to Our Knowledge
Diaphragmatic excursion kinetics assessed with tissue Doppler imaging has the potential role to predict extubation failure as early as at the end of a spontaneous breathing trial. In particular, inspiratory peak and mean velocity, in combination with other well-defined risk factors for extubation failure, might play an important role in identifying subjects at risk of re-intubation within 48 h after extubation. Greater diaphragmatic activation was associated with extubation failure.
Methods
Our observational cohort study, approved by local the ethics committee on March 22, 2019 (CE 23/19) and subsequently registered with ClinicalTrials.gov (NCT03962322) was conducted in accordance with the Helsinki Declaration principles in the ICU of “Maggiore della Carità” University Hospital, Novara, Italy. Written informed consent was obtained from all subjects according to local regulations.
Subjects
Adult patients who had undergone invasive mechanical ventilation for > 24 h and were extubated after passing a 30-min SBT on CPAP of 5 cm H2O according to our institutional weaning protocol, conducted using the ventilator circuit, were eligible for enrollment (to view our detailed institutional weaning protocol, see the supplementary materials at http://www.rcjournal.com). Exclusion criteria were a failed SBT, a previous diagnosis of diaphragmatic palsy, recent thoracotomy or sternotomy (within the previous year), diagnosis of pneumothorax or pneumomediastinum, consent refusal, a poor diaphragmatic ultrasound window, pregnancy, and end-of-life extubation.
Ultrasound
dTDI measurements were obtained at the bedside with subjects in a 30° semi-recumbent position using a portable ultrasound machine equipped with a sectorial probe (1.8–4.2 MHz) and a dedicated cardiac tissue Doppler application (Xario 200, Canon Medical Systems, Zoetermeer, The Netherlands).22,23 Using the right side only (due to the poor acoustic window of the left side resulting from the presence of the spleen and impairments deriving from gastric or colic meteorism24,25), the transducer was positioned between the midclavicular and anterior axillary line in the subcostal region and oriented to find the confluence of the hepatic veins into the inferior vena cava via the liver.23,26,27 With the ultrasound beam perpendicularly oriented toward the middle or posterior third of the diaphragm, the tissue Doppler application was switched on and a clear diaphragm signal was attained by gain fading and excluding high-frequency signals. Once the Doppler cursor had been aligned to the diaphragmatic displacement direction, the maximum amplitude sample box (20 mm) was positioned on the diaphragmatic line to acquire its excursion.22,23 The velocity scale was set as low as possible to catch the slower velocity of diaphragmatic excursion with respect to the beating heart (Fig. 1A).22 From the dTDI waveforms, the following parameters were acquired (Fig. 1B): inspiratory peak velocity (the maximum velocity during inspiration; cm/s), inspiratory mean velocity (the mean velocity computed across the whole inspiration; cm/s), velocity-time integral (excursion) (the area under the velocity curve for the entire inspiration; cm), inspiratory acceleration (the slope of the steepest portion of the inspiratory velocity curve from baseline to inspiratory peak velocity; cm/s2), peak relaxation velocity (the maximum diaphragmatic velocity during expiration; cm/s), expiratory mean velocity (the mean velocity computed over the full expiration; cm/s), and expiratory acceleration (relaxation rate) (the slope of the steepest portion of the expiratory velocity curve from baseline to peak relaxation velocity; cm/s2). The values of these parameters were averaged for 3 consecutive breaths and stored electronically.

Diaphragmatic excursion velocity assessment through tissue Doppler imaging. The spectrum of diaphragmatic excursion velocity is reported during inspiration and expiration. A: Diaphragmatic kinetics variables during inspiration and expiration. B: Inspiratory peak velocity = the maximal velocity during inspiration (cm/s); inspiratory mean velocity = the mean velocity computed across the whole inspiration (cm/s); velocity-time integral (excursion) = the area under the velocity curve for the entire inspiration (cm); inspiratory acceleration = the slope of the steepest portion of the inspiratory velocity curve from baseline to inspiratory peak velocity (cm/s2); peak relaxation velocity = the maximum diaphragmatic velocity during expiration (cm/s); expiratory mean velocity = the mean velocity computed over the full expiration (cm/s); expiratory acceleration (relaxation rate) = the slope of the steepest portion of the expiratory velocity curve from baseline to peak relaxation velocity (cm/s2).
Protocol
dTDI was performed by a single operator, who was not involved in the subjects’ care, at the end of the SBT. After extubation, subjects were allowed to breathe spontaneously with additional oxygen to maintain  between 90% and 94%. Subjects at high risk for extubation failure subsequently received noninvasive ventilation (NIV), either in CPAP or pressure support ventilation mode.28,29 Extubation failure was defined as the need for re-intubation or NIV as a rescue therapy within 48 h after extubation29,30 (for NIV application and re-intubation criteria in the case of extubation failure, see the supplementary materials at http://www.rcjournal.com). Subjects receiving prophylactic NIV or high-flow nasal cannula were not considered as extubation failures.
between 90% and 94%. Subjects at high risk for extubation failure subsequently received noninvasive ventilation (NIV), either in CPAP or pressure support ventilation mode.28,29 Extubation failure was defined as the need for re-intubation or NIV as a rescue therapy within 48 h after extubation29,30 (for NIV application and re-intubation criteria in the case of extubation failure, see the supplementary materials at http://www.rcjournal.com). Subjects receiving prophylactic NIV or high-flow nasal cannula were not considered as extubation failures.
Measurements
Subject demographics, admission diagnosis, and Simplified Acute Physiologic Score II (SAPS II) were acquired for all individuals.  , electrocardiogram, invasive arterial blood pressure, breathing frequency, and tidal volume were monitored throughout the whole study period. dTDI evaluation, arterial blood gas analysis, assessment of dyspnea according to the visual analog scale, and sedation according to Richmond Agitation-Sedation Scale (RASS) were obtained immediately after the end of the SBT. The tidal volume and breathing frequency were acquired from the ventilator. Furthermore, conventional and diaphragmatic RSBIs were computed as previously described.24,31
, electrocardiogram, invasive arterial blood pressure, breathing frequency, and tidal volume were monitored throughout the whole study period. dTDI evaluation, arterial blood gas analysis, assessment of dyspnea according to the visual analog scale, and sedation according to Richmond Agitation-Sedation Scale (RASS) were obtained immediately after the end of the SBT. The tidal volume and breathing frequency were acquired from the ventilator. Furthermore, conventional and diaphragmatic RSBIs were computed as previously described.24,31
Intra- and Inter-Observer Reliability
dTDI intra- and inter-observer reliability of 2 operators were tested prior to subject enrollment. Each assessor carried out dTDI evaluations in 10 intubated ICU individuals. For each subject, the dTDI measurements were acquired across 4 breaths. Five minutes after the completion of the first assessment, a second dTDI assessment was performed in the same subject for another 4 breaths.
Statistical Analysis
The sample size was computed based on the difference in diaphragmatic peak relaxation velocity between successfully weaned subjects and those who experienced weaning failures, according to recent findings.22 In our setting, the subjects enrolled in the study were divided in 2 groups: extubation failures and extubation successes. Considering an expected extubation failure rate of 20%,2 a total of 89 subjects were calculated as necessary to demonstrate whether any difference in diaphragmatic peak relaxation velocity existed between extubation failure subjects and extubation success subjects (Type I error rate = 0.05; Type II error rate = 0.20, 80% power). Assuming a 10% dropout rate, we opted for a sample size of 100 subjects.
Data are summarized as medians (interquartile range) and were analyzed using the Mann-Whitney test for the comparison of continuous variables between the extubation failure group and the extubation success group. Categorical variables, whenever dichotomous or nominal, were reported as numbers and percentages and analyzed using the Fisher exact test. Receiver operating characteristic curves were also obtained for dTDI parameters, as well as for the conventional and diaphragmatic RSBIs. The area under the curve, cutoff, sensitivity, specificity, and positive and negative likelihood ratios were reported for tissue Doppler parameters and for conventional and diaphragmatic RSBIs. Area under the curve comparisons were carried out according to the DeLong method.32 Two-tailed tests were applied for hypothesis testing, and statistical significance was considered for P values < .05.
For the dTDI intra- and inter-observer reliability analysis, Pearson correlation, bias with the limits of agreement, and the intraclass correlation coefficient were computed. For computation of the intraclass correlation coefficient, 2-way mixed effects for absolute agreement between the measurements for each dTDI variable were considered.33 Statistical analyses were conducted using R 3.5.2 software (The R Foundation for Statistical Computing, Vienna, Austria).
Results
As depicted in Figure 2, from May to November 2019, 159 subjects were assessed for eligibility, of whom 100 subjects were enrolled and finally analyzed (ie, 79 extubation success subjects and 21 extubation failure subjects). The causes of postextubation respiratory failure were inspiratory stridor in 3 of 21 subjects (14.3%), respiratory failure in 10 of 21 subjects (47.6%), cardiac arrest in 1 of 21 subjects (4.8%), and neurological impairment in 7 of 21 subjects (33.3%). Prophylactic NIV was employed in 12 subjects (15.2%) and 5 subjects (23.8%) in the extubation success and failure groups, respectively. The baseline characteristics of the study population are reported in Table 1. Of the admission diagnoses, comorbidities were more frequently observed in the extubation failure group compared with individuals in the extubation success group (P = .032). In 7 subjects (33.3%) from the extubation failure group, an ineffective cough was described before re-intubation.
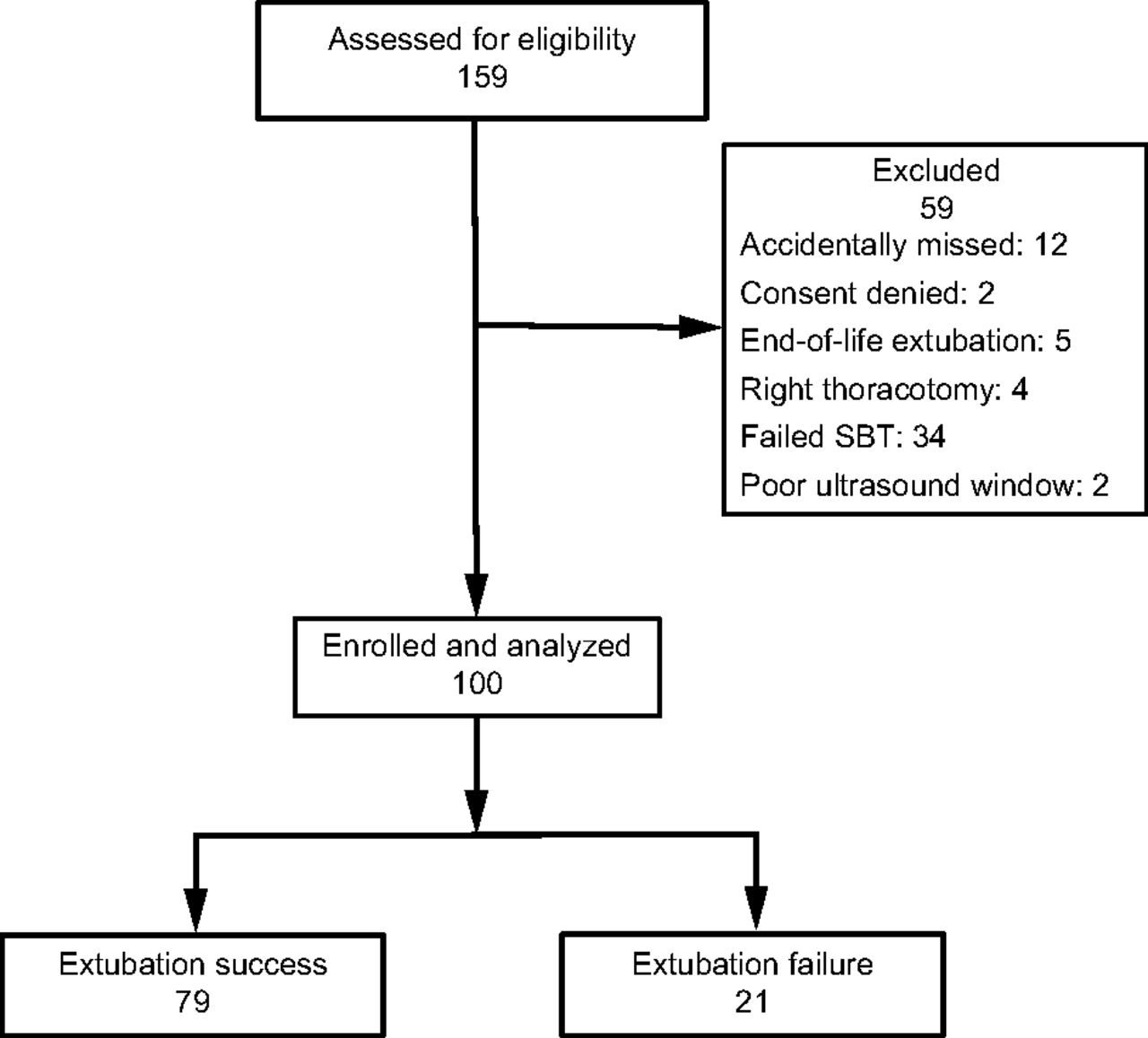
Flow chart. SBT = spontaneous breathing trial.
Baseline Characteristics of the Study Population
In our setting, diaphragmatic excursion kinetics were assessed with dTDI evaluation for a total of 300 breaths (ie, 237 breaths in the extubation success group, 63 breaths in the extubation failure group). Table 2 describes the dTDI assessments at the end of the SBT. Despite no differences in inspiratory excursion observed at the end of the SBT, the inspiratory peak excursion velocity, mean velocity, and acceleration were lower in extubation success subjects compared with those attained from extubation failure subjects. Similarly, during expiration, extubation failure subjects showed a higher peak relaxation velocity, mean velocity, and acceleration compared with those obtained from extubation successes.
Diaphragmatic Excursion Tissue Doppler at the End of the Spontaneous Breathing Trial
Table 3 reports the accuracy with which the dTDI variables and conventional and diaphragmatic RSBIs are able to predict extubation failure at the end of the SBT. The related receiver operating characteristic curves are depicted in Figure 3 for inspiratory and expiratory diaphragmatic kinetics parameters. The area under the curve values for the inspiratory peak and mean velocities were wider than those obtained for the conventional (vs inspiratory peak velocity, P = .036; vs inspiratory mean velocity, P = .042) and diaphragmatic RSBIs (vs inspiratory peak velocity, P = .01; vs inspiratory mean velocity, P = .005). The comparison of areas under the curve is presented in Table 4.
Accuracy in Predicting Extubation Failure at the End of the Spontaneous Breathing Trial

Receiver operating characteristic curves for diaphragmatic displacement tissue Doppler parameters, conventional and diaphragmatic RSBIs. A: Inspiratory values. B: Expiratory values. RSBI = rapid shallow breathing index; AUC, area under the curve.
Difference in Area Under the Curve Analysis
Table 5 reports subjects’ breathing patterns, hemodynamics, visual analog scale dyspnea, and sedation level, as well as the conventional and diaphragmatic RSBI values at the end of the SBT. With the exception of the breathing frequency and visual analog scale dyspnea, which were lower in extubation successes than in extubation failures, no differences in the remaining parameters were observed.
Parameters at the End of the Spontaneous Breathing Trial
The arterial blood gas data for the study population are presented in Table 6. At the end of the SBT,  was higher in extubation success subjects than in extubation failure subjects. pH,
was higher in extubation success subjects than in extubation failure subjects. pH,  , lactate, and bicarbonate serum levels were not different between groups.
, lactate, and bicarbonate serum levels were not different between groups.
Arterial Blood Gases
Clinical outcomes are reported in Table 7. As expected, ICU length of stay, re-intubation rate, and tracheostomy rate were higher in the extubation failure group than in the extubation success group.
Clinical Outcomes
For dTDI intra- and inter-observer variability, a total of 160 breaths were analyzed (ie, 80 for each assessor). The Pearson correlation coefficient, the bias with limits of agreement, and the intra-class correlation coefficient for each dTDI variable are presented in the supplementary materials (available at http://www.rcjournal.com). The intra-class correlation coefficient was ≥ 0.85 for all dTDI variables.
Discussion
The main findings of this study can be summarized as follows: (1) at the end of the SBT, with the exception of inspiratory excursion, which was similar among groups, all the other dTDI variables were significantly higher in the subjects who went on to exhibit extubation failure within 48 h after invasive mechanical ventilation interruption compared with those who were successfully extubated; (2) in our mixed ICU population, values of diaphragmatic inspiratory peak and mean velocity were good predictors of subsequent extubation failure following a successful SBT; and (3) in this study, dTDI assessment was characterized by good intra- and inter-observer reliability.
Diaphragm ultrasound is an easy-to-learn technique,34 widely used to monitor mechanical ventilation both in the ICU20,35 and in the emergency department.36 However, the role of diaphragm ultrasound in predicting extubation failure is still under debate.16-18 In a recent study, dTDI was employed at the end of the SBT to evaluate diaphragmatic kinetics during weaning from invasive mechanical ventilation.22 According to this previous investigation,22 inspiratory peak velocity, expiratory relaxation velocity, and expiratory maximum relaxation rate (ie, acceleration) were higher in subjects who failed the SBT with respect to subjects who passed the weaning trial. In good agreement with that study,22 in our setting, the abovementioned dTDI variables were higher in subjects in the extubation failure group compared with subjects in the extubation success group, with the exception of the inspiratory velocity-time integral (ie, inspiratory excursion). In addition, we observed higher values of mean velocity during both inspiration and expiration as well as inspiratory acceleration in the extubation failure subjects than in extubation success subjects. However, although the values of inspiratory peak velocity and expiratory relaxation velocity in our extubation failure subjects were quite similar to those of the weaning failure group in the study by Soilemezi et al (3.29 vs 2.66 cm/s and 3.26 vs 3.36 cm/s, respectively),22 the expiratory relaxation rate was substantially lower in our extubation failure subjects compared with the weaning failures from Soilemezi et al (17.59 vs 29.47 cm/s2, respectively).22 This probably depended on the different SBT modes adopted in the 2 studies (ie, CPAP 5 cm H2O in our study vs T-tube in the cited study22) and the fact that, contrary to our subjects who all passed the weaning trial and were extubated, the weaning failure group in the cited study22 constituted those who did not pass the SBT and continued invasive mechanical ventilation.
Inspiratory diaphragmatic excursion during an assisted breath is the sum of machine ventilatory assistance and diaphragmatic contraction.35,37 In light of previous findings,38 we can hypothesize that the extent of inspiratory diaphragmatic activity increased in our subjects when ventilatory support was removed during the SBT. Although the SBT was conducted in CPAP 5 cm H2O mode in our setting, the higher dTDI parameters at the end of the SBT suggested a greater diaphragmatic activation in extubation failures with respect to extubation successes. The greater diaphragmatic activation observed in extubation failure subjects could be explained by a lower level of oxygenation in these subjects compared with the extubation success group, which may have acted as a continuous trigger for increased respiratory demand.39,40 The hypothesis that diaphragmatic effort was greater in the extubation failure group to ensure adequate alveolar ventilation and gas exchange is congruent with previous findings obtained in intubated ICU subjects undergoing mechanical ventilation.41 According to these results,41 extubation failure subjects experienced poorer outcomes, not only in the presence of diaphragmatic atrophy/failure, but also when the respiratory muscles were not sufficiently unloaded during mechanical ventilation. To note, diaphragmatic dysfunction has been described in approximatively 40% of patients within the first 3 d of invasive mechanical ventilation.25,41 This dysfunction is sustained by a reduction in the strength and cross-sectional area of the myofibers as a result of excessive ventilatory assistance, deep sedation, and myo-relaxant administration.42,43 The extent of diaphragmatic inactivity is correlated to diaphragmatic thickness and is associated with adverse outcome in intubated patients.44
In our investigation, dTDI parameters were more accurate predictors of extubation failure than both the conventional15 and diaphragmatic24 RSBIs. The conventional RSBI is one of the most-used clinical predictors of weaning and extubation outcome because it provides a good indication of the balance between the mechanical load placed on the respiratory muscles and their ability to handle this load during an SBT performed in T-tube mode.15,31 However, when an SBT is conducted in modes other than the T-tube mode, the variability in the sensitivity and specificity of this index in predicting weaning outcome is greater.45 Recently, the diaphragmatic RSBI, which assesses the ratio of diaphragmatic excursion to breathing frequency, has been proposed.24 Despite being a good predictor of weaning outcome when SBT is conducted using a T-piece, this index might be affected by the same limitations associated with the conventional RSBI during an SBT conducted in pressure support ventilation or CPAP mode. Thus, in our setting, neither the conventional nor the diaphragmatic RSBI provided a satisfactory predictive value with respect to extubation outcome, as expected.
Regarding clinical implications, once a patient has successfully passed an SBT with an increased diaphragmatic activation as revealed by dTDI assessment, close clinical monitoring should be ensured in the 48 h after extubation to enable the prompt identification of the onset of extubation failure and a timely intervention. Alternatively, under these conditions, the application of prophylactic NIV soon after extubation might be justified to reduce the mismatch between the load imposed on the diaphragm and its neuromuscular capacity during spontaneous breathing.
Limitations
Our study has several limitations. First, this was a single-center observational study conducted on a mixed ICU population, including mainly neurocritical care subjects. Despite the number of subjects involved, our findings should be confirmed in further investigations specifically addressing the different subsets of subjects and focused on the validation of the dTDI technique. Second, we employed dTDI at the end of the SBT conducted in CPAP 5 cm H2O mode. Thus, our conclusions cannot be extended to SBTs carried out in other modalities. Third, we decided a priori not to assess the diaphragmatic thickness and thickening fraction. Indeed, diaphragmatic thickness and thickening fraction assessment are more prone to intra- and inter-individual errors (ie, parallax error and the capacity to acquire the thickening fraction on the same portion of the diaphragm over time) compared with excursion analysis.20,46 Moreover, the validity of the diaphragmatic thickening fraction to ascertain diaphragmatic effort is limited because it is only moderately correlated with the pressure-generating capacity of the diaphragm.19,20 Fourth, we only investigated and reported dTDI evaluations in subjects who passed the SBT because our aim was only to assess the existence of a relationship between postextubation respiratory failure and dTDI variables acquired at the end of an SBT. Last, we defined extubation failure as the need for re-intubation or NIV within 48 h after extubation.29,30,47 However, our results might be different if the definition were extended to 7 d after extubation, as recently described.48
Conclusions
In our mixed ICU population, when dTDI was performed at the end of an SBT, a greater diaphragmatic activation was observed in subjects who experienced extubation failure within 48 h after extubation compared with those who were successfully extubated, with no difference in inspiratory diaphragmatic displacement. Diaphragmatic inspiratory peak and mean velocity performed well as predictors of extubation failure occurring within 48 h of a successful SBT. Our results must be confirmed in future multicenter clinical trials addressing the role of dTDI in the prediction of extubation failure.
Acknowledgments
We thank all of the ICU clinical staff for the support provided during the study.
Footnotes
- Correspondence: Gianmaria Cammarota MD PhD, Department of Medicine and Surgery, Università degli Studi di Perugia, Perugia, Italy. E-mail: gmcamma{at}gmail.com
Supplementary material related to this paper is available at http://www.rcjournal.com
Drs De Robertis and Vaschetto are co-first authors.
Dr Boniolo presented a version of this paper at the SIAARTI Congress, held October 16–18, 2019, in Rome, Italy.
Dr Messina has disclosed a relationship with Vygon. Dr Navalesi has disclosed relationships with Maquet Critical Care, Draeger, Intersurgical, Oriopharma, Philips, Resmed, MSD, and Novartis. Dr Navalesi also contributed to the development of the patented ‘helmet Next’, the royalties for which are paid to Intersurgical. Drs Navalesi and Longhini both contributed to the development of a device not discussed in the present study with patent application number: EP20170199831. The other authors have disclosed no conflicts of interest.
- Copyright © 2021 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}