

Abstract
BACKGROUND: Mechanical insufflation-exsufflation (MI-E) is a noninvasive technique performed to simulate cough and remove sputum from proximal airways. To date, the effects of MI-E on critically ill patients on invasive mechanical ventilation are not fully elucidated. In this randomized crossover trial, we evaluated the efficacy and safety of MI-E combined to expiratory rib cage compressions (ERCC).
METHODS: Twenty-six consecutive subjects who were sedated, intubated, and on mechanical ventilation > 48 h were randomized to perform 2 sessions of ERCC with or without additional MI-E before tracheal suctioning in a 24-h period. The primary outcome was sputum volume following each procedure. Secondary end points included effects on respiratory mechanics, hemodynamics, and safety.
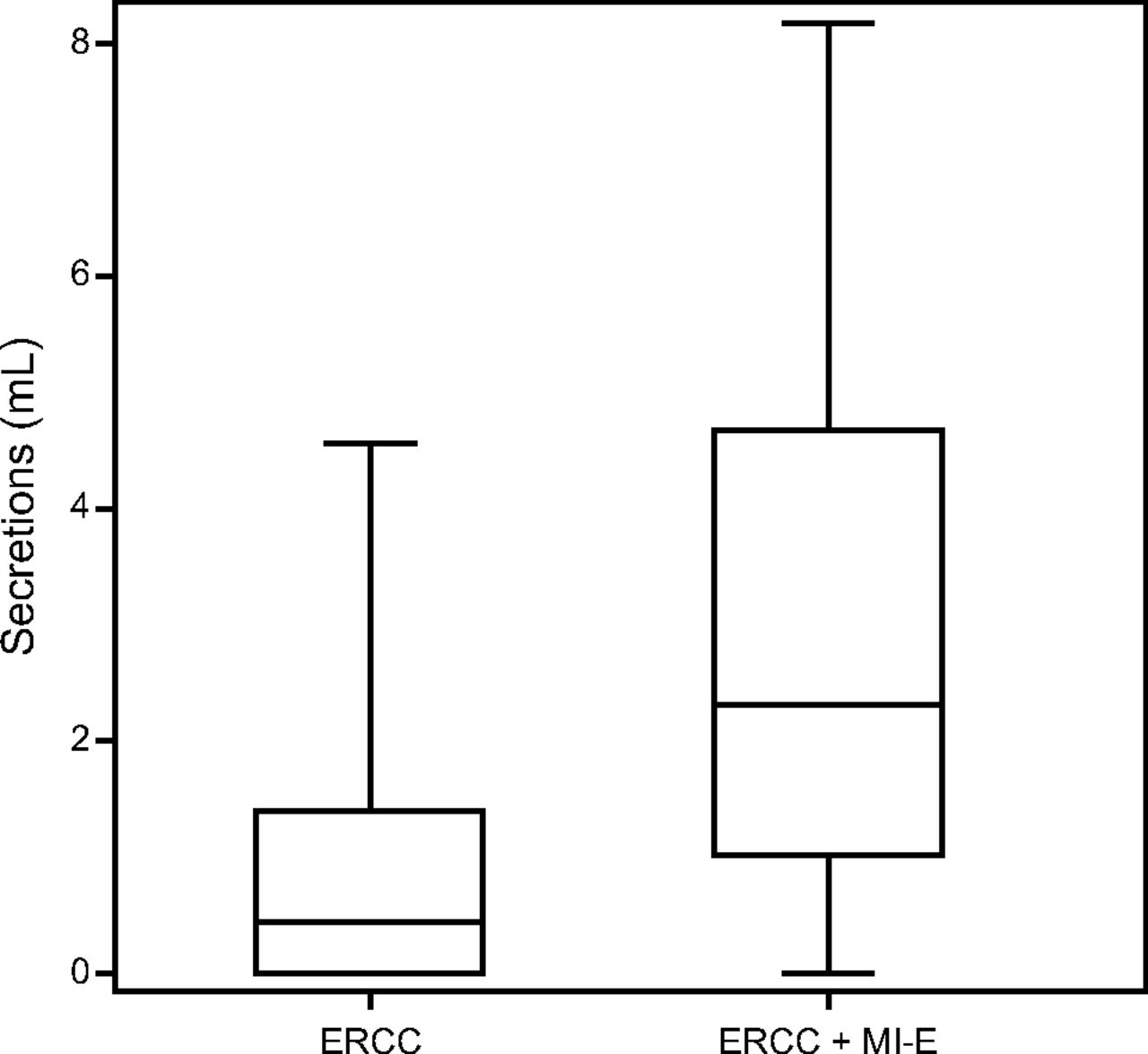
RESULTS: In comparison to ERCC alone, median (interquartile range) sputum volume cleared was significantly higher during ERCC+MI-E (0.42 [0–1.39] mL vs 2.29 [1–4.67] mL, P < .001). The mean ± SD respiratory compliance improved in both groups immediately after the treatment, with the greater improvement in the ERCC+MI-E group (54.7 ± 24.1 mL/cm H2O vs 73.7 ± 35.8 mL/cm H2O, P < .001). Differences between the groups were not significant (P = .057). Heart rate increased significantly in both groups immediately after each intervention (P < .05). Additionally, a significant increase in oxygenation was observed from baseline to 1 h post-intervention in the ERCC+MI-E group (P < .05). Finally, several transitory hemodynamic variations occurred during both interventions, but these were nonsignificant and were considered clinically irrelevant.
CONCLUSIONS: In mechanically ventilated subjects, MI-E combined with ERCC increased the sputum volume cleared without causing clinically important hemodynamic changes or adverse events. (ClinicalTrials.gov registration: NCT03316079.)
- mechanical ventilation
- sputum clearance
- physiotherapy
- mechanical insufflation-exsufflation
- pulmonary mechanics
Introduction
Retention of airway secretions is a frequent complication in critically ill patients on invasive mechanical ventilation.1 One of the main causes is the presence of an endotracheal tube (ETT), which has been demonstrated to decrease mucociliary clearance2 and hinder the ability to generate adequate peak expiratory flows (PEF) when coughing.3 Inspiratory flow bias during mechanical ventilation,4 semi-Fowlers patient positioning,5 or suboptimal humidification of respiratory gases6 further impair sputum clearance. Retention of airway secretions is a risk factor for respiratory infections and lobar collapse1 and may prolong mechanical ventilation and ICU length of stay.7,8 Therefore, interventions aimed to improve secretion clearance are pivotal in decreasing morbidity of patients requiring mechanical ventilation.
During mechanical ventilation, endotracheal suctioning is recommended only when clinically indicated to remove retained secretions.9 However, only marginal removal of peripheral secretions is achieved during the procedure.10 Consequently, clinicians may increase suctioning frequency, leading to an increased risk of associated complications, including alveolar collapse, tracheal mucosa injury, and respiratory or hemodynamic impairment.11,12
Expiratory rib cage compressions (ERCC) is a common physiotherapy technique performed before endotracheal suctioning to enhance expiratory air flows and cephalad movement of secretions.13,14 However, although ERCC are frequently used in the ICU, only a small body of evidence exists to support its use in this setting, specifically during invasive mechanical ventilation. Moreover, the methods applied to implement ERCC are highly inconsistent across studies, and extrapolation of the results is complex.15-17
Mechanical insufflation-exsufflation (MI-E) is a noninvasive technique performed to mimic the act of coughing and clear secretions from the proximal airways.18 Theoretically, the negative expiratory pressure applied promotes high PEF that moves airway secretions cranially. To date, only a few studies have evaluated the efficacy and safety of MI-E in ventilated critically ill subjects, with data commonly indicating an increased removal of airway secretions19-22 without any deleterious effects.20-22 MI-E has been more widely investigated in spontaneously breathing patients with neuromuscular diseases unable to produce an effective cough.23 However, translation of the aforementioned results to the ICU setting is challenging because most studies have been undertaken in non-intubated patients.
To address these limitations, we performed a study in critically ill patients who were sedated and receiving mechanical ventilation > 48 h via an ETT to evaluate potential adjuvant effects of MI-E in clearing airway secretions after routine application of ERCC. In addition, we comprehensively evaluated resulting air flows, hemodynamic changes, and potential adverse events.
QUICK LOOK
Current Knowledge
Mechanically ventilated patients often present with airway secretion retention and ineffective cough. In this context, expiratory rib cage compressions may be carried out to help clear secretions. Mechanical insufflation-exsufflation (MI-E) is a technique that propels retained airway secretions toward the larger airways, similar to a simulated cough, and has been suggested as a potential strategy to clear airway secretions.
What This Paper Contributes to Our Knowledge
In this crossover randomized clinical trial in mechanically ventilated subjects, MI-E combined with expiratory rib cage compressions led to a greater volume of cleared secretions compared to expiratory rib cage compressions alone, with clinically insignificant hemodynamic changes.
Methods
Study Design
We conducted a prospective, crossover, randomized, single-blind study in a medical and a surgical ICU at Bordeaux University Hospital (France). The study was approved by the institution’s ethics committee (DC2015/02).
Population
Adult patients (> 18 y) on mechanical ventilation for > 48 h, with Richmond Agitation and Sedation Scores ranging from –3 to –5 and tracheally intubated (ETT internal diameter 7.0–8.0 mm), were evaluated daily for inclusion. Patients with lung trauma or with emphysema, pneumothorax, mechanical ventilation-associated barotrauma, pulmonary instability (PEEP > 10 cm H2O or  < 90%) or mean arterial pressure < 65 mm Hg (irrespective of vasoactive support) were excluded. Patients who met aforementioned criteria were included after the next of kin provided consent. All subjects received the 2 interventions, with a 4-h washout period to avoid carryover effects. We used a web-based, computer-generated, single-block randomization system to randomly decide which intervention they received first (ERCC or ERCC+MI-E), with each intervention followed by endotracheal suctioning. Additionally, we ensured that no suctioning was performed 4 h prior to the first intervention and between interventions (Fig. 1).
< 90%) or mean arterial pressure < 65 mm Hg (irrespective of vasoactive support) were excluded. Patients who met aforementioned criteria were included after the next of kin provided consent. All subjects received the 2 interventions, with a 4-h washout period to avoid carryover effects. We used a web-based, computer-generated, single-block randomization system to randomly decide which intervention they received first (ERCC or ERCC+MI-E), with each intervention followed by endotracheal suctioning. Additionally, we ensured that no suctioning was performed 4 h prior to the first intervention and between interventions (Fig. 1).

Study protocol.
Interventions
Five experienced respiratory physiotherapists performed the ERCC as routinely applied in participating units. Prior to the intervention, the internal ETT cuff pressure was adjusted to 30 cm H2O and subjects were positioned in the semi-recumbent position with the head of the bed ≥ 30° above horizontal. Either soft/prolonged or hard/prompt manual rib cage compressions were applied to dislodge airway secretions from the distal or proximal airways, respectively, as indicated by chest auscultation.24-26 After ERCC, MI-E was delivered with a Cough Assist E-70 (Philips North America, Andover, Massachusetts). The MI-E was set to automatic mode with ± 40 cm H2O insufflation-exsufflation pressure, medium inspiratory flow, and an inspiratory-expiratory time of 3 s and 2 s, respectively, with a 1-s pause.27 We performed 4 series of 5 insufflation-exsufflation cycles, with a 1-min pause between series to allow reconnection to mechanical ventilation and avoid potential oxygen desaturation and de-recruitment.
Measurements
The primary outcome was quantification of wet volume of sputum. Once each intervention was completed (ie, after implementation of ERRC in the ERRC group or after completion of the 4 series of insufflation-exsufflation cycles in EERC+MI-E group), the secretions were immediately suctioned using an open suction procedure and collected through a 12-Fr catheter (Biçakcilar, Istanbul, Turkey) connected to a sterile collector container (Vygon, Ecouen, France). The suction procedure was performed as recommended by international guidelines.9 At the end of the suction procedure, if needed, 5 mL saline solution were instilled and aspirated through the suction catheter to clear secretions adherent to the internal lumen of the suction catheter. This instilled saline volume was ultimately subtracted from the overall volume of secretions.
Mechanical ventilator tidal volumes, peak inspiratory flow (PIF), PEF, and airway pressures were measured before interventions, after endotracheal suctioning, and 1 h thereafter with the Fluxmed GrH monitor (MBMED, Buenos Aires, Argentina).28 All data were recorded and analyzed with the dedicated FluxReview software (MBMED). The aforementioned parameters were also continuously recorded during the MI-E procedure. Prior to the MI-E intervention, a flow-pressure transducer was connected between the Y-piece of the ventilatory circuit and the ETT, while during MI-E it was moved between the ETT and MI-E circuit. Air flow and pressure rates of 5 respiratory cycles were averaged and compared. Respiratory system compliance, airway resistance, and lung tissue resistance were calculated using standard formulas.4 During MI-E operation, PIF and PEF were recorded and averaged for each insufflation-exsufflation cycle; we also calculated the PEF-PIF difference and the PEF:PIF ratio. Heart rate, systolic and diastolic blood pressure, arterial gas exchange (ie,  and
and  ) and
) and  were obtained before, during and after the intervention. MI-E was stopped if evidence of pneumothorax appeared. Similarly, MI-E was ceased
were obtained before, during and after the intervention. MI-E was stopped if evidence of pneumothorax appeared. Similarly, MI-E was ceased  consistently decreased to < 85% or > 10% from baseline, heart rate increased/decreased > 20% from baseline, and systolic blood pressure or diastolic blood pressure increased/decreased > 20% from baseline.
consistently decreased to < 85% or > 10% from baseline, heart rate increased/decreased > 20% from baseline, and systolic blood pressure or diastolic blood pressure increased/decreased > 20% from baseline.
Statistical Analysis
We hypothesized that the difference in secretion volume obtained with endotracheal suctioning between the 2 interventions would be 1.5 mL. Thus, for an assumed effect size of 1.33 of the paired t test, a desired statistical power of 90%, and type 1 bias of 5%, we calculated that a total sample size of 26 subjects was needed, of whom 6 subjects would potentially be lost during enrollment. We report the mean ± SD or the median (interquartile range [IQR]) for continuous variables, while categorical variables are presented as the number and percentage of patients. The Wilcoxon test was used to compare 2 paired groups. The Friedman test was used to compare > 2 paired groups. Linear regression analysis was performed to examine the correlation between continuous variables. As sensitivity analyses, we performed an analysis of variance model for crossover designs29,30 to examine differences in the primary outcome between the 2 groups, and analysis of covariance (ANCOVA) models for crossover designs in the rest of the outcomes to provide supportive information (see the supplementary materials at http://www.rcjournal.com). All statistical comparisons were 2-sided hypothesis tests, and the significance level was set at .05. All confidence intervals (CIs) were 2-sided at 95% confidence level. SPSS 25.0 (IBM, Armonk, New York) was the statistical software used to analyze the data sets.
Results
A total of 100 consecutive subjects were screened from March 2015 to June 2017, and 26 subjects met the inclusion criteria (Fig. 2). Baseline characteristics of the study population are presented in Table 1. Three subjects did not complete the study because they awakened before completion of the protocol. In 2 subjects (1 control and 1 intervention), respiratory mechanics and gas exchange were not measured following the intervention and 1-h post-treatment for technical reasons (Fig. 2). Sputum volume was not obtained for 1 subject in the intervention group due to a malfunction of the vacuum system.

Flow chart. MI-E = mechanical insufflation-exsufflation; RASS = Richmond agitation and sedation scale.
Anthropometric Values of Subjects
We recorded a total of 430 MI-E cycles, with an average of 16.5 ± 3.7 administered cycles per subject. During MI-E, all volumes, pressures, and flows were consistent within the series (see the supplementary materials at http://www.rcjournal.com). Irrespective of the pre-set insufflation-exsufflation pressure (± 40 cm H2O), the device was able to generate an adequate peak inspiratory pressure of 41.3 ± 2.3 cm H2O, but only 65.8% of the preset negative expiratory pressure (–26.3 ± 9.9 cm H2O, P = .02). MI-E produced PEF and PIF rates of 96.9 ± 20.6 L/min and 66.7 ± 11.7 L/min, respectively, resulting in a PEF-PIF difference of 30.6 ± 12.6 L/min and a PEF:PIF ratio of 1.47 ± 0.20.
Efficacy of MI-E
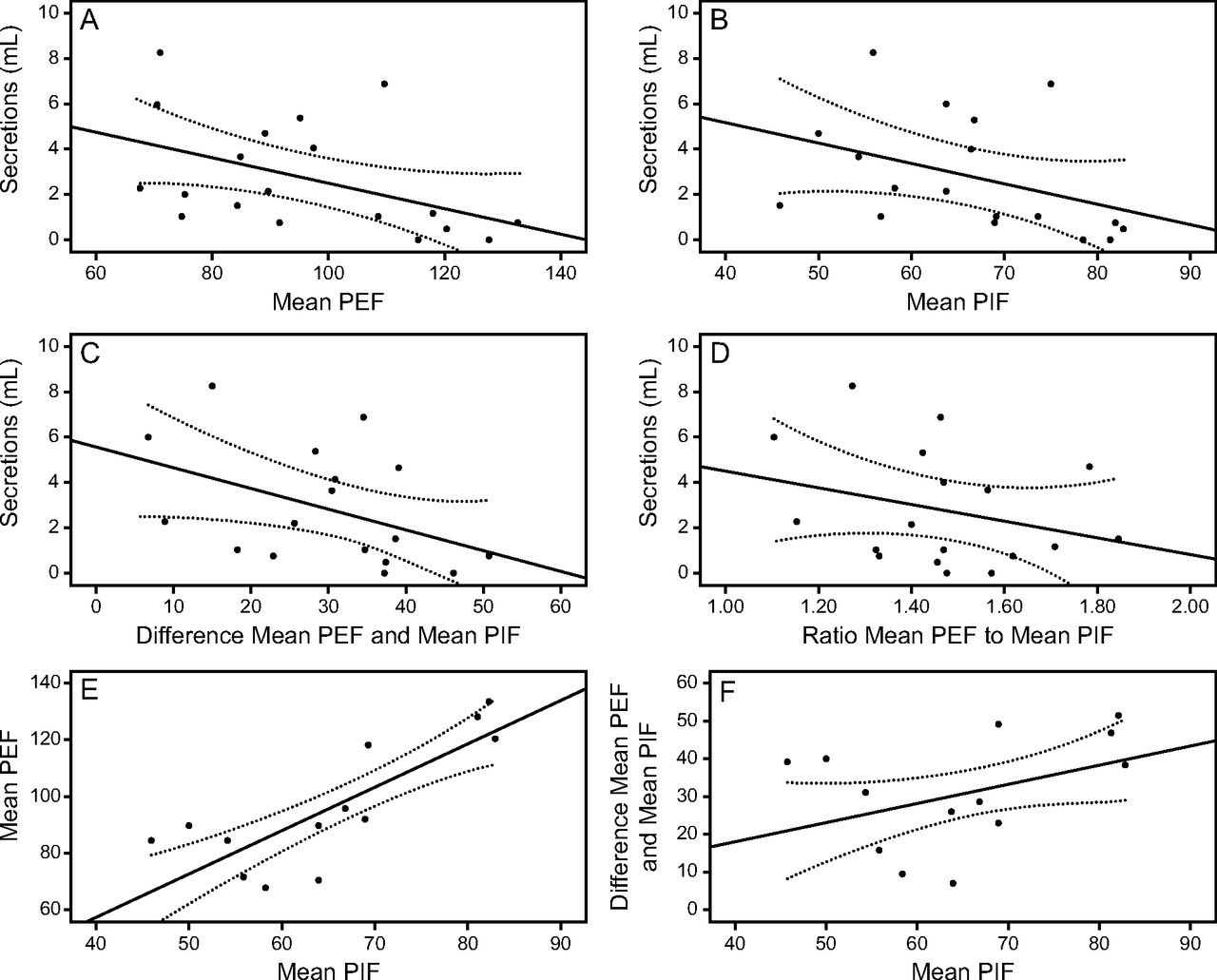
The median (IQR) secretion volume retrieved during ERCC and MI-E was significantly higher in comparison to ERCC alone (2.29 [IQR 1–4.67] mL vs 0.42 [IQR 0–1.39] mL, P < .001) (Fig. 3). The adjusted mean secretion volume was greater for the ERCC+MI-E group compared to ERCC alone (3.02 mL for ERCC+MI-E and 0.84 mL for ERCC, P < .001; difference between groups, 2.18 mL [95% CI 1.24–3.12]) (see the supplementary materials at http://www.rcjournal.com). An inverse correlation was found between the volume of retrieved secretions and PEF generated during MI-E but with weak goodness-of-fit (adjusted r2 = 0.17, P = .038) (Fig. 4). The PIF (adjusted r2 = 0.10, P = .11), the PEF-PIF difference (adjusted r2 = 0.16, P = .059), and the PEF:PIF ratio (adjusted r2 = 0.03, P = .25) did not correlate with volume of secretions retrieved. Interestingly, we observed a significant correlation of PIF with PEF and flow bias (adjusted r2 = 0.66, P < .001; adjusted r2 = 0.14, P = .07, respectively) (Fig. 4).

Sputum retrieved during expiratory rib cage compressions (ERCC) compared to ERCC with mechanical insufflation-exsufflation (ERCC+MI-E). Median (interquartile range) of secretions: ERCC+MI-E 2.29 (1–4.67) mL vs ERCC 0.42 (0–1.39) mL (P < .001).

Linear regressions between sputum and flows generated during MI-E. Relationship between volume of sputum retrieved during expiratory rib cage compressions with MI-E (ERCC+MI-E) and flows generated during MI-E. A: Association between mean peak expiratory flow (PEF) and volume of secretions retrieved: n = 20, r2 = 0.17 (P = .04). B: Association between mean peak inspiratory flow (PIF) and volume of secretions retrieved: n = 18, r2 = 0.1 (P = .11). C: Association between PEF-PIF difference and volume of secretions retrieved: n = 18, r2 = 0.16 (P = .06). D: Association between mean PEF:PIF ratio and volume of secretions retrieved: n = 18, r2 = 0.03 (P = .25). E: Association between mean PIF and mean PEF: n = 18, r2 = 0.66 (P < .001). F: Association between PEF-PIF difference and PIF: n = 18, r2 = 0.14 (P = .07). MI-E = mechanical insufflation-exsufflation.
Overall, no significant differences in respiratory system compliance, airway resistance, and lung tissue resistance were observed when comparing the interventions or evaluation periods (Table 2). In the ERCC+MI-E group, mean ± SD respiratory system compliance significantly improved (54.7 ± 24.1 mL/cm H2O vs 73.7 ± 35.8 mL/cm H2O, P < .001), but the beneficial effect tapered off 1 h after the intervention. ANCOVA analyses revealed similar results (see the supplementary materials at http://www.rcjournal.com).
Pulmonary Mechanics, Hemodynamics, and Gas Exchange
Safety of MI-E
As shown in Table 2, heart rate increased following both ERCC and ERCC+ MI-E (P < .05), but the increase was greater after the ERCC intervention and persisted even 1 h after the intervention in comparison with ERCC+MI-E (P < .05). These differences were not corroborated in ANCOVA analyses (see the supplementary materials at http://www.rcjournal.com). All remaining hemodynamic parameters varied marginally throughout the interventions. A significant increase in  was found 1 h after the intervention in the ERCC+MI-E group compared to the ERCC group (P < .03) and compared to
was found 1 h after the intervention in the ERCC+MI-E group compared to the ERCC group (P < .03) and compared to  in the ERCC+MI-E group after intervention (P < .003) (Table 2). Similarly, ANCOVA analysis showed a statistical improvement in
in the ERCC+MI-E group after intervention (P < .003) (Table 2). Similarly, ANCOVA analysis showed a statistical improvement in  1 h after the ERCC+MI-E intervention in comparison to the ERCC group (P = .008; see the supplementary materials at http://www.rcjournal.com). Despite these positive results following ERCC+MI-E, they did not correlate with the volume of secretions cleared (adjusted r2 = 0.004, P = .76). A total of 21 episodes of brief desaturations or hemodynamic variations were documented, 10 during ERCC+MI-E and 11 during single ERCC treatments, with no significant difference between interventions (see the supplementary materials at http://www.rcjournal.com). Importantly, due to marginal clinical severity and brief duration of aforementioned adverse events, protocolized interventions were never ceased.
1 h after the ERCC+MI-E intervention in comparison to the ERCC group (P = .008; see the supplementary materials at http://www.rcjournal.com). Despite these positive results following ERCC+MI-E, they did not correlate with the volume of secretions cleared (adjusted r2 = 0.004, P = .76). A total of 21 episodes of brief desaturations or hemodynamic variations were documented, 10 during ERCC+MI-E and 11 during single ERCC treatments, with no significant difference between interventions (see the supplementary materials at http://www.rcjournal.com). Importantly, due to marginal clinical severity and brief duration of aforementioned adverse events, protocolized interventions were never ceased.
Discussion
This is the first clinical trial evaluating the efficacy and safety of ERCC+MI-E and endotracheal suctioning in a cohort of sedated critically ill adult subjects on mechanical ventilation. The combination of ERCC and MI-E was associated with a significant increase in the volume of secretions compared with ERCC alone. Additionally, MI-E resulted in a short-term improvement in respiratory system compliance without any clinically relevant complications.
Previous studies have also used sputum clearance as the primary outcome to evaluate MI-E efficacy, but inconsistent results have been reported. In a previous study performed in a mixed population of 180 intubated critically ill subjects, Ferreira de Camillis et al21 reported a significant improvement in the weight of secretions obtained through MI-E in comparison with routine chest physiotherapy. In this study, routine chest physiotherapy included manual chest compressions, applied upon left and right lateral decubitus, followed by manual hyperinflation. Unfortunately, manual chest compressions were poorly described, making any extrapolation of the MI-E benefits or inefficacy of the applied ERCC techniques challenging. Conversely, in a crossover study in 43 invasively ventilated ICU subjects, Coutinho et al20 noted negligible effects of MI-E performed prior to endotracheal suctioning. The study presented some incongruencies between planned primary outcome (volume of secretions) and assessed outcome (weight of secretions), questioning whether the study was adequately powered to achieve its stated aims.
Previous studies of MI-E have commonly focused on neurologically impaired subjects with respiratory problems, and data on the efficacy and safety of MI-E in other ventilated ICU cohorts are very limited.18 To our knowledge, this is the first study to investigate the effects of MI-E and ERCC in a more diverse ICU population, with our subjects being a mix of surgical and medical patients However, although MI-E has predominantly been used in patients with neurological disorders, ICU-acquired weakness also affects the respiratory muscles, which commonly lead to limitations in cough strength in all patient cohorts requiring prolonged mechanical ventilation.31 Similarly, post-surgical incision pain commonly inhibits the production of a strong and effective cough. It is therefore important to consider MI-E as a treatment option for other patient cohorts beyond neurologically impaired patients, including post-surgical patients or patients developing expiratory muscle weakness and an ineffective cough due to a prolonged period of mechanical ventilation.
In this study, we observed that greater volumes of secretions were cleared when MI-E was used in conjunction with ERCC. A potential explanation for our positive results is the resulting PEF during MI-E (96.9 ± 20.6 L/min). Previous studies in intubated and ventilated subjects have implied that a PEF > 160 L/min is required to mobilize secretions.32 In mechanistic in vitro studies, Guérin et al33 concluded that MI-E pressures should be increased up to 50 cm H2O to achieve the aforementioned PEF values when endotracheal or tracheostomy tubes are used. A more recent review, however, concluded that a large PEF range of 64–126 L/min might be sufficient to facilitate clearance of secretions and successfully wean patients from mechanical ventilation.34 Thus, in our study, we achieved a sufficient PEF even though subjects were fully sedated, hence unable to perform expiratory efforts, and air flow resistance imposed by the ETT decreased the expiratory pressure by 34%.
In our study, the MI-E device was set at +40/–40 cm H2O pressure with medium inspiratory flow. These pressures were chosen because previous clinical studies reported that subjects tolerated the resulting insufflation and exsufflation better.18,23 However, in a recent bench study, Volpe et al35 demonstrated that expiratory flow bias and cephalad sputum displacement may be enhanced by reducing flows during the inspiratory phase of MI-E and increasing the negative expiratory pressure over inspiratory pressure (eg, +40/–60). Thus, the use of medium flow and equivalent insufflation-exsufflation pressures in our settings may explain the correlation between PIF and PEF. Therefore, cautious extrapolations on the unexpected slight inverse relationship between secretion clearance and PEF may be made due to the low flow bias generated during our protocol.
The impact of MI-E on pulmonary mechanics has been well reported, but, similar to sputum clearance, the results have been mixed. Ferreira de Camillis et al21 observed short-term improvement in lung compliance after application of MI-E in comparison with routine chest physiotherapy. Recently, Nunes et al22 investigated the effects of different MI-E pressure combinations versus standard endotracheal suctioning in 16 intubated subjects. In this randomized crossover trial, when inspiratory/expiratory pressures of 50 cm H2O were applied, lung compliance improved immediately after the intervention and 10 min thereafter. Despite these encouraging results, other publications have consistently failed to demonstrate benefits.19,20,22 Potentially, the more significant improvements in compliance are related to a higher number of performed MI-E cycles (30 and 20, respectively) in comparison with other negative studies that used lower number of MI-E cycles. In our study, respiratory system compliance increased immediately after the ERCC+MI-E intervention, but the improvement in compliance was not sustained 1 h after the intervention and was not significantly different between groups. One possible explanation for this lack of sustained effect is that MI-E may act as a lung recruitment maneuver; thus, if PEEP is not titrated and adjusted accordingly, de-recruitment can still occur in the follow-up period. In addition, our use of open suction procedures instead of closed suctioning may have contributed to further lung de-recruitment.
One effect of MI-E may be an improvement in oxygenation. Some studies have observed an increase in  after both endotracheal suctioning and MI-E22; however, other publications failed to corroborate these results.19,20 Conversely, Sánchez-García et al19 reported an improvement in
after both endotracheal suctioning and MI-E22; however, other publications failed to corroborate these results.19,20 Conversely, Sánchez-García et al19 reported an improvement in  following MI-E, although it should be emphasized that a continuous flow of oxygen at 8 L/min was administered at the filter port, adjacent to the MI-E device. Supplementary oxygen was not administered in our study, but we still observed an improvement in
following MI-E, although it should be emphasized that a continuous flow of oxygen at 8 L/min was administered at the filter port, adjacent to the MI-E device. Supplementary oxygen was not administered in our study, but we still observed an improvement in  and
and  after EERC+MI-E. This might be due to the effects of MI-E on lung aeration and perfusion as, during insufflation, MI-E creates a high transpulmonary pressure that may displace air and blood toward collapsed alveolar regions, resulting in shunt improvement and increasing saturation.36
after EERC+MI-E. This might be due to the effects of MI-E on lung aeration and perfusion as, during insufflation, MI-E creates a high transpulmonary pressure that may displace air and blood toward collapsed alveolar regions, resulting in shunt improvement and increasing saturation.36
In our study, a few episodes of minor respiratory and hemodynamic changes occurred during MI-E. However, these events were not deemed to be clinically important, did not differ significantly from the control group, lasted for a very brief period, and early protocol interruption was never necessary by the attending clinicians. Indeed, both the MI-E and control group mainly experienced a slight increase in blood pressure and heart rate during interventions. Occurrence of these events was registered at the end of each intervention. This highlights that MI-E, ERCC, and endotracheal suctioning may affect hemodynamic parameters, which should be taken into account in patients at risk of hemodynamic instability. In addition, as previously reported, MI-E has been associated with hypoxemia, de-recruitment, and pneumothorax18,37; thus, usage in patients with underlying acute or chronic pulmonary diseases should be carefully considered.
Some limitations in this study merit consideration. First, volume of secretions was applied as a surrogate end point of secretion clearance, which could ultimately decrease the accuracy of our results. However, the crossover design was chosen specifically to offset these limitations to control for patient factors. Second, respiratory physiotherapists could not be blinded to treatment allocation, and neither the number of ERCC nor the type or duration of each applied ERCC were recorded. Therefore, one type of ERCC could have been applied more frequently than the other, and this might have influenced the results. Finally, the small sample size should be acknowledged. However, we carried out a comprehensive sample-size analysis, based on a previous pilot study including 15 subjects and in line with previous studies in this field of investigation. Larger randomized studies are required to determine whether the addition of MI-E to ECRR leads to changes that are clinically important and improves patient outcomes.
Conclusions
In subjects receiving invasive mechanical ventilation, a combination of ERCC and MI-E before endotracheal suctioning improved the sputum volume cleared in comparison to ERCC alone. PEF values achieved duuring MI-E were similar to those described in the literature previous patients extubation. MI-E resulted in a short-term improvement in respiratory system compliance and induced marginal, clinically insignificant hemodynamic variations. These findings call for larger clinical trials to evaluate the impact of MI-E on major clinical outcomes and to further investigate the indications for the use of MI-E in intubated and mechanically ventilated patients.
Footnotes
- Correspondence: Antoni Torres MD PhD, Servei de Pneumologia i Al·lèrgia Respiratòria, Hospital Clínic, Calle Villarroel 170, Esc 6/8 Planta 2, 08036 Barcelona, Spain. E-mail: ATORRES{at}clinic.cat
See the Related Editorial on Page 1495
This work was partially supported by the Sociedad Española de Neumología y Cirugía Torácica (research fund 077/2016). The authors have disclosed no conflicts of interest.
- Copyright © 2021 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}
{kind=link}