
To the Editor:
We read with great interest the article by Vargas et al1 on their in vitro study of the flow resistance of a double lumen endotracheal tube (DLET) suggested as an alternative to a standard orotracheal tube for ventilation during percutaneous tracheostomy. However, we feel some aspects deserve further comments. They made a comparison of flow resistance among the different standard-size endotracheal tubes and the DLET during fiberoptic bronchoscope insertion, remarking upon the presence of a well known increased flow resistance when the fiberoptic bronchoscope is inserted in standard devices. Although the authors carried out extensive work on the physical properties of the DLET in vitro, as we can clearly read in the abstract and text, the title refers to an in vivo clinical procedure. Moreover, even if they show relevant data, they extend their conclusions to clinical practice. The final judgment on the use of the device in vivo, based only on the in vitro experimental study, does not reflect the study's data.
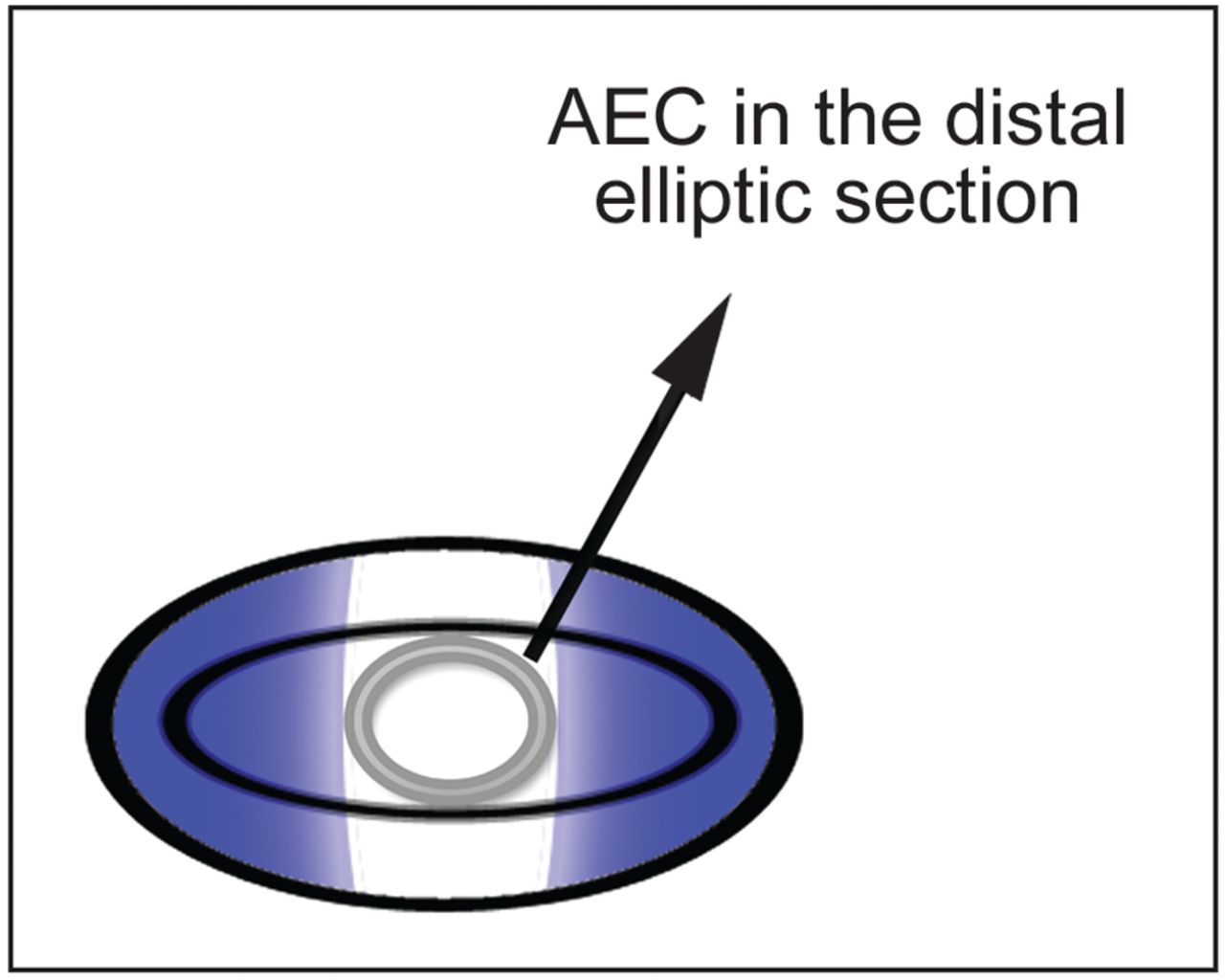
Other comments based on our clinical experience are then necessary. The first, which concerns in vivo experimentation, is about tube positioning. We agree that the tube can be safely positioned with a tube exchanger (airway exchange catheter [AEC]), but a small one (outer diameter) is needed due to the distal DLET's elliptic shape (Fig. 1). For the same reason, DLET slippage on the AEC can result in further difficulties: when the DLET is inserted with the AEC, the elliptic shape defines 2 semilunar lateral areas exceeding the AEC profile (Fig. 1, blue areas). These areas could impact anatomical structures with glottic damage and bleeding if the DLET is positioned with only the AEC.

{kind=link}
Airway exchange catheter (AEC) in the distal elliptic section of a double lumen endotracheal tube.
In our clinical practice, we use a small diameter tube (5-mm inner diameter) that can be safely positioned with the AEC without laryngoscopy, as we have described previously.2,3 We know that the resistances in the smaller diameter tube are increased, but they affect only the mechanical ventilator in the inspiratory phase. In the expiratory phase, the flow follows the physiological path because the tube is uncuffed. This system offers the greatest vision of the operatory field without any interference with ventilation or surgery during the entire procedure.
Footnotes
The authors have disclosed no conflicts of interest.
- Copyright © 2015 by Daedalus Enterprises
References
- 1.
- 2.
- 3.