
Abstract
Objective
To validate a new system for functional residual capacity (FRC) measurements using oxygen washin/washout in spontaneously breathing humans. The system (LUFU, Drägerwerk AG, Lübeck, Germany) consists of an unmodified EVITA 4 ventilator, a side-stream paramagnetic oxygen sensor and a dedicated software.
Design
Laboratory study and measurements in spontaneously breathing volunteers.
Setting
Pulmonary function laboratory of a university hospital.
Participants
20 healthy and 15 lung diseased volunteers.
Interventions
FRC was measured by LUFU (LUFU-FRC) and by helium dilution (He-FRC); intra-thoracic gas volume (ITGV) was determined by body plethysmography. Each measurement cycle consisted of four independent LUFU-FRC determinations (step change of FiO2 from 0.21 to 0.5 and back and from 0.21 to 1.0 and back), two helium-dilution runs and two body box measurements. Repeatability and agreement between methods were determined by comparing different measurements of one technique and by comparing different techniques among each other.
Measurements and results
Repeatability of LUFU-FRC was estimated by comparing washin to washout and the different FiO2steps. The difference of the means was 3.7% at the most. Agreement between methods resulted in the following differences (mean ± standard deviation of differences) for healthy and lung-diseased volunteers, respectively: LUFU-FRC vs. He-FRC –0.40 ± 0.50 L (0.02 ± 0.95 L), LUFU-FRC vs. ITGV –0.43 ± 0.54 L (–0.18 ± 0.61 L) and He-FRC vs. ITGV –0.03 ± 0.43 L (–0.20 ± 0.98 L).
Conclusions
LUFU is a non-invasive method for the determination of FRC that requires only minor additional equipment and no modification to the ventilator. It can be used in difficult conditions such as breathing patterns with variations from breath to breath. The results of this study show that LUFU is sufficiently reliable and repeatable to warrant its clinical application.
Similar content being viewed by others


Introduction
Functional residual capacity (FRC), the lung volume at the end of expiration, is the principle determinant of the area available for gas exchange; thus, knowing the FRC of a patient on mechanical ventilation could help to understand the patho-physiological mechanism behind an oxygenation problem. It could be used for trend analysis and finally support therapeutic decision making [1]. To date, measurement of FRC has not gained significance in clinical anaesthesia and intensive care medicine, probably because of the lack of equipment that could be easily applied in these high-dependency environments.
In non-ventilated patients, FRC is determined mainly by three methods: dilution or washout techniques for nitrogen or inert gases such as helium, argon or sulfurhexafluoride; body plethysmography; and finally, three-dimensional imaging technologies. All of these methods have been tested extensively for their reliability, and some of them have gained clinical acceptance or have even become the method of choice in lung function laboratories [2–5]. While body plethysmography cannot be applied in adult ventilated patients, the other methods can be used only in conjunction with dedicated equipment (special helium sensor or mass spectrometer) or with gases and valves not commonly used in the clinical setting.
The current study was designed to validate a novel method for FRC determination by oxygen washin and washout, called LUFU (acronym for LUng FUnction). It uses oxygen as tracer gas assuming a steady state for oxygen uptake during the measurement [6]. This kind of FRC measurement neither requires modifications to the ventilator nor interruption of the care process. The present study in healthy subjects and in volunteers with pulmonary disease tested LUFU-FRC against helium dilution and body plethysmography.
Materials and methods
Measurement sequence
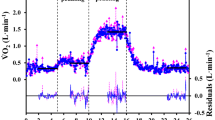
For LUFU-FRC measurements volunteers breathed spontaneously through a EVITA 4 ventilator (Drägerwerk AG, Lübeck, Germany) in CPAP mode (CPAP = 0 cmH2O) via a tightly sealing mouthpiece and with the nose clipped. FiO2 (fraction of inspired oxygen) was changed from 0.21 to 0.5 (washin with delta FiO2 of 0.29) and back (washout/0.29) and from 0.21 to 1.0 (washin/0.79) and back (washout/0.79). Time for reaching an oxygen concentration equilibrium at the new level, approximately 10 min, determined duration of one FRC determination.
Oxygen concentration was measured by a paramagnetic side-stream O2-sensor (Pm 1111E, Servomex Group Ltd, Crowborough, England). Its signal as well as pressure and flow sensed by the ventilator were processed by a PC running a custom-built software. The FRC was calculated from the difference between inspired and expired amount of oxygen, corrected for the constant oxygen uptake and the change of the end-expiratory oxygen concentration. Details about this method and the results of lab tests have been described elsewhere [6] (see also the electronic supplement).
Values of LUFU-FRC measurements were compared with those for intra-thoracic gas volume (ITGV) delivered by a body box (Jaeger-Master Lab, version 1.11, Viasys GmbH—Erich Jaeger, Hoechberg, Germany) and to those from a helium-dilution technique using the helium-rebreathing circuit of the above-mentioned Jaeger-Master Lab.
Volunteers
After approval by the local ethics committee and written informed consent of each volunteer, a total of 35 individuals were included in the study. Twenty of them (11 men and 9 women) were clinically healthy and in good physical condition (mean age 27.1 years, mean body mass index 23.2 kg m–2) without abnormalities in their lung function tests. Fifteen volunteers (12 men and 3 women, mean age 63.3 years, mean body mass index 26.2 kg m–2) had known pulmonary disease and showed pathological test results: vital capacity between 0.98 and 4.99 L, forced expiratory volume in the first second between 50 and 88% of vital capacity (for additional data see electronic supplement). Individuals were not allowed to eat or drink within 4 h prior to the study. Smokers were allowed to have their last cigarette 1 h prior. Measurements of LUFU-FRC and He-FRC were performed both in sitting and in supine positions. Due to the design of the body box ITGV could be determined only in sitting position. Each measurement was performed in duplicate, resulting in a total of 14 individual values for lung volumes (2 × ITGV, 2 × He-FRC sitting, 2 × He-FRC supine, 4 × LUFU-FRC sitting and 4 × LUFU-FRC supine). Since most volunteers with diseased lungs presented with dyspnoea even at rest, most of them could sustain the measurement procedure in the sitting position only. This resulted in a total of 8 volumes per individual (2 × ITGV, 2 × He-FRC sitting, 4 × LUFU-FRC sitting). The sequence of measurements was randomized to avoid systematic error, i. e. due to fatigue. All values obtained in the same body position were averaged.
Statistics
Statistical analysis followed the guidelines proposed by Bland and Altman for the comparison of two methods [7]. A mean difference between both methods (bias) and a standard deviation (SD) of this difference (precision) were calculated together with the upper and lower limits of agreement (mean ± 1.96 * SD) and the 95% confidence interval of bias [mean ± (SD/n1/2) * t distribution (n – 1 degrees of freedom and 5% probability)]. Repeatability within the three methods was also tested according to Bland and Altman.
Results
Repeatability
The LUFU-FRC results obtained during washin and washout did not differ significantly from each other, nor did those obtained with the two FiO2 steps. The ITGV measurements showed good repeatability both in healthy and diseased subjects, whereas He-FRC measurements were sufficiently repeatable only in healthy subjects (Table 1; see also electronic supplement).
Agreement between methods
Table 1 shows the main results as mean values and standard deviations of LUFU-FRC, He-FRC and ITGV, respectively, together with mean bias and precision between the different methods. When comparing each of the methods with the corresponding other methods in the way described by Bland and Altman, all values fell within the limits of agreement; thus, between ± 1.96 times the standard deviation. In all comparisons of the different methods used, no dependency of differences from mean values was noticed. Due to the poor repeatability of the He-FRC measurements in diseased subjects, LUFU-FRC was compared with ITGV only in this group.
Figure 1 demonstrates the level of agreement between LUFU-FRC and He-FRC of healthy subjects in the sitting and supine position and between LUFU-FRC and ITGV in healthy and diseased subjects.

a–d Differences between He-FRC and LUFU-FRC in healthy subjects in sitting position, between He-FRC and LUFU-FRC in healthy subjects in supine position, between ITGV and LUFU-FRC in healthy subjects in sitting position, and between ITGV and LUFU-FRC in diseased subjects in sitting position. Black lines indicate mean bias, whereas dashed lines mark limits of agreement
Discussion
This study demonstrated that determination of FRC by oxygen washin and washout is both feasible and comparable in quality to that by reference techniques in spontaneously breathing subjects.
Repeated LUFU measurements showed bias, precision and repeatability coefficient in the same range as those of helium dilution and body plethysmography. The exception is the poor reproducibility of the helium dilution method in diseased subjects, a previously described problem [8–11]. In this group LUFU showed better performance.
Bias, i. e. mean differences of values measured with two different methods, as well as its standard deviation, were similar when comparing LUFU to the established methods and for comparison between He-FRC and ITGV (see Table 1).
Other studies show values similar to ours both for repeatability of helium dilution and body plethysmography [11, 12] and for agreement between these methods [8, 11, 13, 14]. Studies on humans [15] or lung models [16, 17] using similar techniques for determining FRC found similar bias of repeatability and bias of agreement between methods.
The LUFU is designed for use in patients on a ventilator, be it during assisted spontaneous breathing or during controlled ventilation. Under these circumstances the knowledge of FRC may help to optimize ventilator settings. Our study was performed in spontaneously breathing volunteers for two reasons: Firstly, comparison of LUFU-FRC to ITGV and He-FRC is not possible in ventilated patients. Secondly, the spontaneous breathing design was more demanding for the method with respect to variations in breathing pattern and oxygen uptake during the measurement than other conceivable designs with more controlled ventilator settings; thus it is reasonable to assume that the LUFU method will be at least as reliable in patients on controlled ventilation.
Is the quality of LUFU measurements acceptable for clinical practice? The low bias found in the comparisons to the other methods is favourable. Repeatability is in the same range as with the other methods: variation of measured values may be ascribed to measurement noise as well as to actual fluctuation of end-expiratory lung volume over time. The LUFU offers considerable advantages in this respect: measurements are frequently repeatable with minimal effort or disturbance of the ongoing therapy.
Conclusion
It is concluded that the LUFU method for determination of FRC is non-invasive, works with currently used ventilators and requires only minor additional equipment. It gives equally reliable and clinically acceptable results as reference methods. Ongoing studies in clinical settings will give insight into the usefulness during anaesthesia and intensive care.
References
Hedenstierna G (1993) The recording of FRC: Is it of importance and can it be made simple? Intensive Care Med 19:365–366
Larsson A, Linnarsson C, Jonmarker C, Jonson B, Larsson H, Werner O (1987) Measurement of lung volume by sulfur hexafluoride washout during spontaneous and controlled ventilation: further development of a method. Anesthesiology 67:543–550
Saniie J, Saidel GM, Chester EH (1979) Realtime moment analysis of pulmonary nitrogen washout. J Appl Physiol 46:1184–1190
Suter PM, Schlobohm RM (1974) Determination of functional residual capacity during mechanical ventilation. Anesthesiology 41:605–607
Wrigge H, Sydow M, Zinserling J, Neumann P, Hinz J, Burchardi H (1998) Determination of functional residual capacity (FRC) by multibreath nitrogen washout in a lung model and in mechanically ventilated patients. Intensive Care Med 24:487–449
Weismann D, Reissmann H, Maisch S, Füllekrug B, Schulte am Esch J (2006) Determination of functional residual capacity with an oxygen washin/washout: technical description and evaluation. J Clin Mon Comp 20:251–260
Bland JM, Altman DG (1986) Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1:307–310
Hildebrand H, Islam MS, Ulmer WT (1984) Comparison between body plethysmographic measurement of the intrathoracic gas volume and oscillatory measurement of the functional residual air capacity in healthy volunteers, miners with and without obstruction of the airways and in patients not exposed to dust but with obstructive airways disease. Prax Klin Pneumol 38:217–219
Kendrick AH (1996) Comparison of methods of measuring static lung volumes. Monaldi Arch Chest Dis 51:431–439
Quanjer PH, Tammeling GJ, Cotes JE, Pedersen OF, Peslin R, Yernault JC (1993) Lung volumes and forced ventilatory flows. Report of the Working Party on Standardization of Lung Function Tests. European Community for Steel and Coal. Official statement of the European Respiratory Society. Eur Respir J 6(Suppl 16):5–40
Schaanning CG, Gulsvik A (1973) Accuracy and precision of helium dilution technique and body plethysmography in measuring lung volumes. Scand J Lab Invest 32:271–277
Hruby J, Butler J (1975) Variability of routine pulmonary function tests. Thorax 30:548–553
Germouty J, Charruyer-Latrille G, Boyer M, Charles A, Jaubert A, Chatelut J, Chantegreil D, Germouty C (1970) La mesure de la capacité résiduelle fonctionelle. Comparaison de trois méthodes: Spirographique, radiographique et plethysmographique chez 100 adultes normaux. Poumon 26:589–594
Rodenstein DO, Stanescu DC (1982) Reassessment of lung volume measurement by helium dilution and by body plethysmography in chronic airflow obstruction. Am Rev Respir Dis 126:1040–1044
Eichler W, Schumacher J, Roth-Isigkeit A, Braun J, Kuppe H, Klotz KF (2002) Automated evaluation of functional residual capacity by oxygen washout. J Clin Monit 17:195–201
Olegard C, Söndergaard S, Houltz E, Lundin S, Stenqvist O (2005) Estimation of functional residual capacity at the bedside using standard monitoring equipment: a modified nitrogen washout/washin technique requiring a small change of the inspired oxygen fraction. Anesth Analg 101:206–212
Stenqvist O, Olegard C, Sondergaard S, Odenstedt H, Karason S, Lundin S (2002) Monitoring functional residual capacity (FRC) by quantifying oxygen/carbon dioxide fluxes during a short apnea. Acta Anaesthesiol Scand 46:732–739
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Rights and permissions
About this article
Cite this article
Maisch, S., Boehm, S.H., Weismann, D. et al. Determination of functional residual capacity by oxygen washin-washout: a validation study. Intensive Care Med 33, 912–916 (2007). https://doi.org/10.1007/s00134-007-0578-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-007-0578-2