
Abstract
Background
This systematic review and meta-analysis summarizes the safety and efficacy of high flow nasal cannula (HFNC) in patients with acute hypoxemic respiratory failure.
Methods
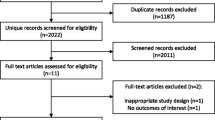
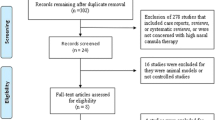
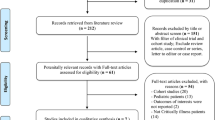
We performed a comprehensive search of MEDLINE, EMBASE, and Web of Science. We identified randomized controlled trials that compared HFNC to conventional oxygen therapy. We pooled data and report summary estimates of effect using relative risk for dichotomous outcomes and mean difference or standardized mean difference for continuous outcomes, with 95% confidence intervals. We assessed risk of bias of included studies using the Cochrane tool and certainty in pooled effect estimates using GRADE methods.
Results
We included 9 RCTs (n = 2093 patients). We found no difference in mortality in patients treated with HFNC (relative risk [RR] 0.94, 95% confidence interval [CI] 0.67–1.31, moderate certainty) compared to conventional oxygen therapy. We found a decreased risk of requiring intubation (RR 0.85, 95% CI 0.74–0.99) or escalation of oxygen therapy (defined as crossover to HFNC in the control group, or initiation of non-invasive ventilation or invasive mechanical ventilation in either group) favouring HFNC-treated patients (RR 0.71, 95% CI 0.51–0.98), although certainty in both outcomes was low due to imprecision and issues related to risk of bias. HFNC had no effect on intensive care unit length of stay (mean difference [MD] 1.38 days more, 95% CI 0.90 days fewer to 3.66 days more, low certainty), hospital length of stay (MD 0.85 days fewer, 95% CI 2.07 days fewer to 0.37 days more, moderate certainty), patient reported comfort (SMD 0.12 lower, 95% CI 0.61 lower to 0.37 higher, very low certainty) or patient reported dyspnea (standardized mean difference [SMD] 0.16 lower, 95% CI 1.10 lower to 1.42 higher, low certainty). Complications of treatment were variably reported amongst included studies, but little harm was associated with HFNC use.
Conclusion
In patients with acute hypoxemic respiratory failure, HFNC may decrease the need for tracheal intubation without impacting mortality.




Similar content being viewed by others
References
Antonelli M, Conti G, Rocco M et al (1998) A comparison of noninvasive positive-pressure ventilation and conventional mechanical ventilation in patients with acute respiratory failure. New Engl J Med 339(7):429–435
Carrillo A, Gonzalez-Diaz G, Ferrer M et al (2012) Non-invasive ventilation in community-acquired pneumonia and severe acute respiratory failure. Intensive Care Med 38(3):458–466
Delclaux C, L’Her E, Alberti C et al (2000) Treatment of acute hypoxemic nonhypercapnic respiratory insufficiency with continuous positive airway pressure delivered by a face mask: a randomized controlled trial. JAMA 284(18):2352–2360
Hilbert G, Gruson D, Vargas F et al (2000) Noninvasive continuous positive airway pressure in neutropenic patients with acute respiratory failure requiring intensive care unit admission. Crit Care Med 28(9):3185–3190
Zhang Y, Fang C, Dong BR et al (2012) Oxygen therapy for pneumonia in adults. Cochrane Database Syst Rev 3:CD006607
Xu XP, Zhang XC, Hu SL et al (2017) Noninvasive ventilation in acute hypoxemic nonhypercapnic respiratory failure: a systematic review and meta-analysis. Crit Care Med 45(7):e727–e733
Bello G, De Pascale G, Antonelli M (2016) Noninvasive ventilation. Clin Chest Med 37(4):711–721
Rochwerg B, Brochard L, Elliott MW et al (2017) Official ERS/ATS clinical practice guidelines: noninvasive ventilation for acute respiratory failure. Eur Respir J 50(2):1602426
Ni YN, Luo J, Yu H et al (2017) Can high-flow nasal cannula reduce the rate of endotracheal intubation in adult patients with acute respiratory failure compared with conventional oxygen therapy and noninvasive positive pressure ventilation? A systematic review and meta-analysis. Chest 151(4):764–775
Huang HW, Sun XM, Shi ZH et al (2018) Effect of high-flow nasal cannula oxygen therapy versus conventional oxygen therapy and noninvasive ventilation on reintubation rate in adult patients after extubation: a systematic review and meta-analysis of randomized controlled trials. J Intensive Care Med 33(11):609–623
Lee CC, Mankodi D, Shaharyar S et al (2016) High flow nasal cannula versus conventional oxygen therapy and non-invasive ventilation in adults with acute hypoxemic respiratory failure: a systematic review. Respir Med 121:100–108
Maitra S, Som A, Bhattacharjee S et al (2016) Comparison of high-flow nasal oxygen therapy with conventional oxygen therapy and noninvasive ventilation in adult patients with acute hypoxemic respiratory failure: a meta-analysis and systematic review. J Crit Care 35:138–144
Zhao H, Wang H, Sun F et al (2017) High-flow nasal cannula oxygen therapy is superior to conventional oxygen therapy but not to noninvasive mechanical ventilation on intubation rate: a systematic review and meta-analysis. Crit Care (Lond, Engl) 21(1):184
Azoulay E, Lemiale V, Mokart D et al (2018) Effect of high-flow nasal oxygen vs standard oxygen on 28-Day mortality in immunocompromised patients with acute respiratory failure: the HIGH randomized clinical trial. JAMA 320(20):2099–2107
RIsk of Bias in Systematic Reviews (2018) cited 2018 September 30, 2018. http://www.evidencepartners.com/resources/methodological-resources/risk-of-bias-commentary/
Guyatt GH, Oxman AD, Vist GE et al (2008) GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ (Clin Res ed) 336(7650):924–926
Higgins JP (2011) Cochrane handbook for systematic reviews of interventions. Version 5.1.0. The Cochrane Collaboration
Higgins JP, Thompson SG (2002) Quantifying heterogeneity in a meta-analysis. Stat Med 21(11):1539–1558
Makdee O, Monsomboon A, Surabenjawong U et al (2017) High-flow nasal cannula versus conventional oxygen therapy in emergency department patients with cardiogenic pulmonary edema: a randomized controlled trial. Ann Emerg Med 70(4):465–472
Lemiale V, Mokart D, Mayaux J et al (2015) The effects of a 2-h trial of high-flow oxygen by nasal cannula versus Venturi mask in immunocompromised patients with hypoxemic acute respiratory failure: a multicenter randomized trial. Crit Care (Lond, Engl) 19:380
Wetterslev J, Jakobsen JC, Gluud C (2017) Trial sequential analysis in systematic reviews with meta-analysis. BMC Med Res Methodol 17(1):39
Azoulay E, Lemiale V, Mokart D et al (2018) Effect of high-flow nasal oxygen vs standard oxygen on 28-Day mortality in immunocompromised patients with acute respiratory failure: the high randomized clinical trial. JAMA 320(20):2099–2107
Bell N, Hutchinson CL, Green TC et al (2015) Randomised control trial of humidified high flow nasal cannulae versus standard oxygen in the emergency department. Emerg Med Australas EMA 27(6):537–541
Frat JP, Thille AW, Mercat A et al (2015) High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. New Engl J Med 372(23):2185–2196
Jones PG, Kamona S, Doran O et al (2016) Randomized controlled trial of humidified high-flow nasal oxygen for acute respiratory distress in the emergency department: the HOT-ER study. Respir Care 61(3):291–299
Parke RL, McGuinness SP, Eccleston ML (2011) A preliminary randomized controlled trial to assess effectiveness of nasal high-flow oxygen in intensive care patients. Respir Care 56(3):265–270
Rittayamai N, Tscheikuna J, Praphruetkit N et al (2015) Use of high-flow nasal cannula for acute dyspnea and hypoxemia in the emergency department. Respir Care 60(10):1377–1382
Schwabbauer N, Berg B, Blumenstock G et al (2014) Nasal high-flow oxygen therapy in patients with hypoxic respiratory failure: effect on functional and subjective respiratory parameters compared to conventional oxygen therapy and non-invasive ventilation (NIV). BMC Anesthesiol 14:66
Doshi P, Whittle JS, Bublewicz M, Kearney J, Ashe T, Graham R, Salazar S, Ellis TW, Jr., Maynard D, Dennis R, Tillotson A, Hill M, Granado M, Gordon N, Dunlap C, Spivey S, Miller TL (2018) High-velocity nasal insufflation in the treatment of respiratory failure: a randomized clinical trial. Ann Emerg Med 72:73–83.e75
Brochard L, Slutsky A, Pesenti A (2017) Mechanical ventilation to minimize progression of lung injury in acute respiratory failure. Am J Respir Crit Care Med 195(4):438–442
Mauri T, Alban L, Turrini C et al (2017) Optimum support by high-flow nasal cannula in acute hypoxemic respiratory failure: effects of increasing flow rates. Intensive Care Med 43(10):1453–1463
Acknowledgements
The authors would like to thank Dr. Iris Arad for her help with the search strategy and running the search.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Dr. Einav has received funding for travel, given lectures, owns patents with and/or performed consultancy work for Zoll, Medtronic and Diasorin, has participated in multicentre trials run by Artisanpharma, Eisai and Astra Zeneca. Dr. Frat reports grants from the French Ministry of Health; grants, personal fees and non- financial support from Fisher & Paykel HeathCare; personal fees and non-financial support from SOS oxygene, outside the submitted work. Dr. Azoulay reports that Fisher & Payckle provided the optiflow device for the HIGH trial (to all the centers). They also provided support to my research group to organize research meetings. He also provides lectures for Alexion Baxter MSD Pfizer and Ablynx. Dr. Mercat receives fees for serving on a steering committee from Faron Pharmaceuticals, consulting fees from Air Liquide Medical Systems, grant support and lecture fees from Fisher and Paykel and Covidien, and lecture fees from Pfizer, ResMed, and Drager. Dr. Demoule reports personal fees from Medtronic, grants, personal fees and non-financial support from Philips, personal fees from Baxter, personal fees from Hamilton, grants and personal fees from Fisher & Paykel, grants from French Ministry of Health, personal fees from Getinge, personal fees from Respinor, outside the submitted work. Dr. Lemiale reports grants from the French Ministry of Health. The research group (GRRR-OH) she belongs to received financial support from Fisher & Paykel HeathCare; Pfizer, Gilead, Astellas And Alexion, outside this submitted work. Prof. Antonio Pesenti received consulting honorarium from Xenion, Maquet and Baxter outside the present work. He is also an inventor of patented devices for respiratory support and extracorporeal carbon dioxide removal. Dr. Mauri received speaking fees from Fisher and Paykel unrelated to the present work. Dr. Mancebo reports receiving personal fees from Faron and Medtronic. Fisher Paykel and A-Lung provided medical equipment for multicenter trials (high flow nasal oxygen therapy and extracorporeal CO2 removal respectively). IMT Medical provided travel and hotel expenses to attend a meeting. Dr. Brochard’s laboratory has received equipment and/or research grants from Fisher Paykel (high-flow), Medtronic Covidien (PAV+), Air Liquide (Helium, CPR), Philips (sleep), Sentec (tcPCO2), General Electric (ultrasound) and consulting from Baxter. Dr. Burns received a grant from Fisher & Paykel to conduct an observational study.
Ethical approval
An approval by an ethics committee was not applicable
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Rochwerg, B., Granton, D., Wang, D.X. et al. High flow nasal cannula compared with conventional oxygen therapy for acute hypoxemic respiratory failure: a systematic review and meta-analysis. Intensive Care Med 45, 563–572 (2019). https://doi.org/10.1007/s00134-019-05590-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-019-05590-5