
Abstract
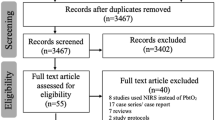
Observational clinical studies demonstrate that brain hypoxia is associated with poor outcome after severe traumatic brain injury (TBI). In this study, available medical literature was reviewed to examine whether brain tissue oxygen (PbtO2)-based therapy is associated with improved patient outcome after severe TBI. Clinical studies published between 1993 and 2010 that compared PbtO2-based therapy combined with intracranial and cerebral perfusion pressure (ICP/CPP)-based therapy to ICP/CPP-based therapy alone were identified from electronic databases, Index Medicus, bibliographies of pertinent articles, and expert consultation. For analysis, each selected paper had to have adequate data to determine odds ratios (ORs) and confidence intervals (CIs) of outcome described by the Glasgow outcome score (GOS). Seven studies that compared ICP/CPP and PbtO2- to ICP/CPP-based therapy were identified. There were no randomized studies and no comparison studies in children. Four studies, published in 2003, 2009, and 2010 that included 491 evaluable patients were used in the final analysis. Among patients who received PbtO2-based therapy, 121(38.8%) had unfavorable and 191 (61.2%) had a favorable outcome. Among the patients who received ICP/CPP-based therapy 104 (58.1%) had unfavorable and 75 (41.9%) had a favorable outcome. Overall PbtO2-based therapy was associated with favorable outcome (OR 2.1; 95% CI 1.4–3.1). Summary results suggest that combined ICP/CPP- and PbtO2-based therapy is associated with better outcome after severe TBI than ICP/CPP-based therapy alone. Cross-organizational practice variances cannot be controlled for in this type of review and so we cannot answer whether PbtO2-based therapy improves outcome. However, the potentially large incremental value of PbtO2-based therapy provides justification for a randomized clinical trial.
Similar content being viewed by others

References
Thurman DJ, Alverson C, Dunn KA, Guerrero J, Sniezek JE. Traumatic brain injury in the United States: a public health perspective. J Head Trauma Rehab. 1999;14(6):602–15.
Chesnut RM, Marshall LF, Klauber MR, et al. The role of secondary brain injury in determining outcome from severe head injury. J Trauma. 1993;34(2):216–22.
Robertson CS, Valadka AB, Hannay HJ, et al. Prevention of secondary ischemic insults after severe head injury. Crit Care Med. 1999;27(10):2086–95.
Stein SC, Georgoff P, Meghan S, Mirza KL, El Falaky OM. Relationship of aggressive monitoring, treatment to improved outcomes in severe traumatic brain injury. J Neurosurg. 2010;112(5):1105–12.
Stein SC, Georgoff P, Meghan S, Mizra K, Sonnad SS. 150 years of treating severe traumatic brain injury: a systematic review of progress in mortality. J Neurotrauma. 2010;27(7):1343–53.
Cremer OL, van Dijk GW, van Wensen E, et al. Effect of intracranial pressure monitoring and targeted intensive care on functional outcome after severe head injury. Crit Care Med. 2005;33(10):2207–13.
Shafi S, Diaz-Arrastia R, Madden C, Gentilello L. Intracranial pressure monitoring in brain-injured patients is associated with worsening of survival. J Trauma. 2008;64(2):335–40.
Le Roux PD, Newell DW, Lam AM, et al. Cerebral arteriovenous oxygen difference: a predictor of cerebral infarction, outcome in patients with severe head injury. J Neurosurg. 1997;87(1):1–8.
Menon DK, Coles JP, Gupta AK, et al. Diffusion limited oxygen delivery following head injury. Crit Care Med. 2004;32(6):1384–90.
Stiefel MF, Udoetuk JD, Spiotta AM, et al. Conventional neurocritical care, cerebral oxygenation after traumatic brain injury. J Neurosurg. 2006;105(4):568–75.
Vespa P, Bergsneider M, Hattori N, Wu HM, Huang SC, Martin NA, Glenn TC, McArthur DL, Hovda DA. Metabolic crisis without brain ischemia is common after traumatic brain injury: a combined microdialysis, positron emission tomography study. J Cereb Blood Flow Metab. 2005;25(6):763–74.
Bratton SL, Chestnut RM, Ghajar J, et al. Guidelines for the management of severe traumatic brain injury. X. Brain oxygen monitoring and thresholds. J Neurotrauma. 2007;24(Suppl 1):S65–70.
Bardt TF, Unterberg AW, Hartl R, Kiening KL, Schneider GH, Lanksch WR. Monitoring of brain tissue PO2 in traumatic brain injury: effect of cerebral hypoxia on outcome. Acta Neurochir Suppl. 1998;71:153–6.
Chang JJ, Youn TS, Benson D, et al. Physiologic, functional outcome correlates of brain tissue hypoxia in traumatic brain injury. Crit Care Med. 2009;37(1):283–90.
Valadka AB, Gopinath SP, Contant CF, Uzura M, Robertson CS. Relationship of brain tissue PO2 to outcome after severe head injury. Crit Care Med. 1998;26(9):1576–81.
van den Brink WA, van Santbrink H, Steyerberg EW, et al. Brain oxygen tension in severe head injury. Neurosurgery. 2000;46(4):868–76. discussion 876–868.
van Santbrink H, Maas AI, Avezaat CJ. Continuous monitoring of partial pressure of brain tissue oxygen in patients with severe head injury. Neurosurgery. 1996;38(1):21–31.
Maloney-Wilensky E, Gracias V, Itkin A, et al. Brain tissue oxygen, outcome after severe traumatic brain injury: a systematic review. Crit Care Med. 2009;37(6):2057–63.
Adamides AA, Cooper DJ, Rosenfeldt FL, et al. Focal cerebral oxygenation and neurological outcome with or without brain tissue oxygen-guided therapy in patients with traumatic brain injury. Acta Neurochir (Wien). 2009;151(11):1399–409.
Martini RP, Deem S, Yanez ND, et al. Management guided by brain tissue oxygen monitoring, outcome following severe traumatic brain injury. J Neurosurg. 2009;111(4):644–9.
McCarthy MC, Moncrief H, Sands JM, et al. Neurologic outcomes with cerebral monitoring in traumatic brain injury. Surgery. 2009;146(4):585–90. discussion 590–91.
Meixensberger J, Jaeger M, Väth A, Dings J, Kunze E, Roosen K. Brain tissue oxygen guided treatment supplementing ICP/CPP therapy after traumatic brain injury. J Neurol Neurosurg Psychiatr. 2003;74(6):760–4.
Narotam PK, Morrison JF, Nathoo N. Brain tissue oxygen monitoring in traumatic brain injury, major trauma: outcome analysis of a brain tissue oxygen-directed therapy. J Neurosurg. 2009;111(4):672–82.
Spiotta AM, Stiefel MF, Gracias VH, et al. Brain tissue oxygen-directed management, outcome in patients with severe traumatic brain injury. J Neurosurg. 2010;113(3):571–80.
Stiefel MF, Spiotta A, Gracias VH, et al. Reduced mortality rate in patients with severe traumatic brain injury treated with brain tissue oxygen monitoring. J Neurosurg. 2005;103(5):805–11.
Rosenthal G, Hemphill JC III, Sorani M, et al. Brain tissue oxygen tension is more indicative of oxygen diffusion than oxygen delivery and metabolism in patients with traumatic brain injury. Crit Care Med. 2008;36:1917–24.
Harris RP, Helfand M, Woolf SH, et al. Current methods of the third US preventive services task force. Am J Prev Med. 2001;20(3 Suppl):21–35.
Contant CF, Valadka AB, Gopinath SP, Hannay HJ, Robertson CS. Adult respiratory distress syndrome: a complication of induced hypertension after severe head injury. J Neurosurg. 2001;95(4):560–8.
Rothwell PM. Can overall results of clinical trials be applied to all patients? Lancet. 1995;345(8965):1616–9.
Thompson SG, Pocock SJ. Can meta-analyses be trusted? Lancet. 1991;338(8775):1127–30.
Villar J, Carroll G, Belizan M. Predictive ability of meta-analyses of randomised controlled trials. Lancet. 1995;345(8952):772–6.
Hedges LV, Olkin I. Statistical methods for meta-analysis. New York: Academia Press; 2002.
Petitti DB. Meta-analysis, decision-analysis and cost-effectiveness analysis. New York: Oxford University Press; 1994.
Bhatia A, Gupta AK. Neuromonitoring in the intensive care unit. II. Cerebral oxygenation monitoring, microdialysis. Intensive Care Med. 2007;33(8):1322–8.
Oddo M, Levine JM, Mackenzie L, Frangos S, Feihl F, Kasner SE, et al. Brain hypoxia is associated with short-term outcome after severe traumatic brain injury independent of intracranial hypertension and low cerebral perfusion pressure. Neurosurgery. 2011 [Epub ahead of print].
Adamides AA, Rosenfeldt FL, Winter CD, et al. Brain tissue lactate elevations predict episodes of intracranial hypertension in patients with traumatic brain injury. J Am Coll Surg. 2009;209(4):531–9.
Belli A, Sen J, Petzold A, Russo S, Kitchen N, Smith M. Metabolic failure precedes intracranial pressure rises in traumatic brain injury: a microdialysis study. Acta Neurochir (Wien). 2008;150(5):461–70.
Pascual JL, Georgoff P, Maloney-Wilensky E, Sims C, Sarani B, Stiefel MF, et al. Reduced brain tissue oxygen in traumatic brain injury: are most commonly used interventions successful? J Trauma. 2011;70(3):535–46.
Harvey S, Harrison DA, Singer M, et al. Assessment of the clinical effectiveness of pulmonary artery catheters in management of patients in intensive care (PAC-Man): a randomised controlled trial. Lancet. 2005;366(9484):472–7.
Richard C, Warszawski J, Anguel N, et al. Early use of the pulmonary artery catheter and outcomes in patients with shock and acute respiratory distress syndrome: a randomized controlled trial. JAMA. 2003;290(20):2713–20.
Sandham JD, Hull RD, Brant RF, et al. A randomized, controlled trial of the use of pulmonary-artery catheters in high-risk surgical patients. N Engl J Med. 2003;348(1):5–14.
Fletcher JJ, Bergman K, Blostein PA, Kramer AH. Fluid balance, complications, brain tissue oxygen tension monitoring following severe traumatic brain injury. Neurocrit Care. 2010;13(1):47–56.
Diringer MN. Hyperoxia: good or bad for the injured brain? Curr Opin Crit Care. 2008;14(2):167–71.
Johnston AJ, Steiner LA, Coles JP, et al. Effect of cerebral perfusion pressure augmentation on regional oxygenation, metabolism after head injury. Crit Care Med. 2005;33(1):189–95.
Tolias CM, Reinert M, Seiler R, Gilman C, Scharf A, Bullock MR. Normobaric hyperoxia–induced improvement in cerebral metabolism, reduction in intracranial pressure in patients with severe head injury: a prospective historical cohort-matched study. J Neurosurg. 2004;101(3):435–44.
Zygun DA, Nortje J, Hutchinson PJ, Timofeev I, Menon DK, Gupta AK. The effect of red blood cell transfusion on cerebral oxygenation, metabolism after severe traumatic brain injury. Crit Care Med. 2009;37(3):1074–8.
Acknowledgments
EM-W and PDL are members of Integra Lifesciences Speaker’s Bureau. Supported in part by Research Grants from the Integra Foundation (PDL), Integra Neurosciences (PDL), and the Mary Elisabeth Groff Surgical and Medical Research Trust (PDL).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nangunoori, R., Maloney-Wilensky, E., Stiefel, M. et al. Brain Tissue Oxygen-Based Therapy and Outcome After Severe Traumatic Brain Injury: A Systematic Literature Review. Neurocrit Care 17, 131–138 (2012). https://doi.org/10.1007/s12028-011-9621-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-011-9621-9