Hookah (Shisha, Narghile) Smoking and Environmental Tobacco Smoke (ETS). A Critical Review of the Relevant Literature and the Public Health Consequences

Abstract
:1. Introduction
Hookah Smoking as a New Public Health and Environmental Research Field
Overview of Landmark Studies on Cigarette ETS
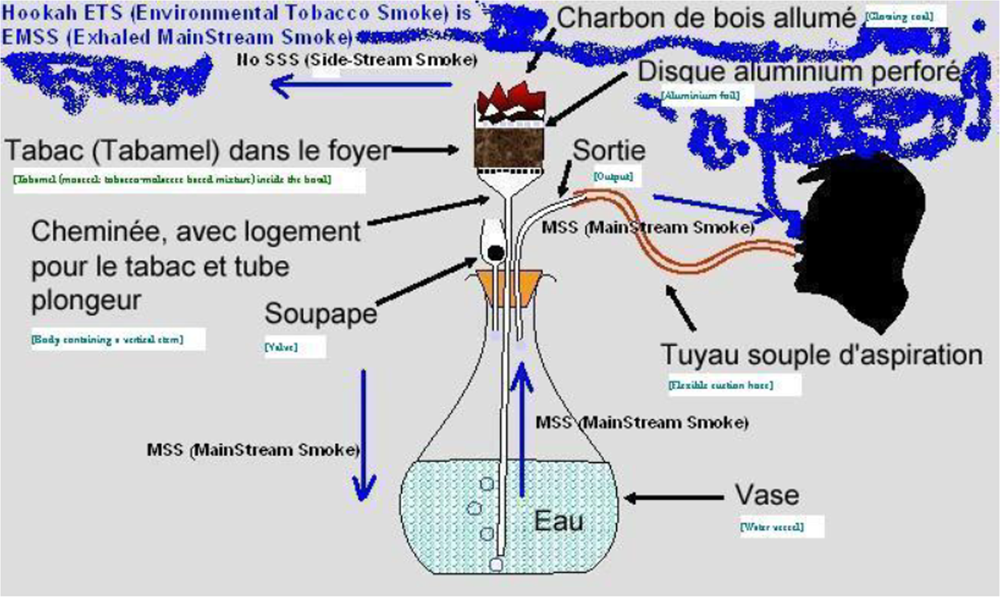
Recent Concern about Hookah ETS and Differences with Cigarette ETS
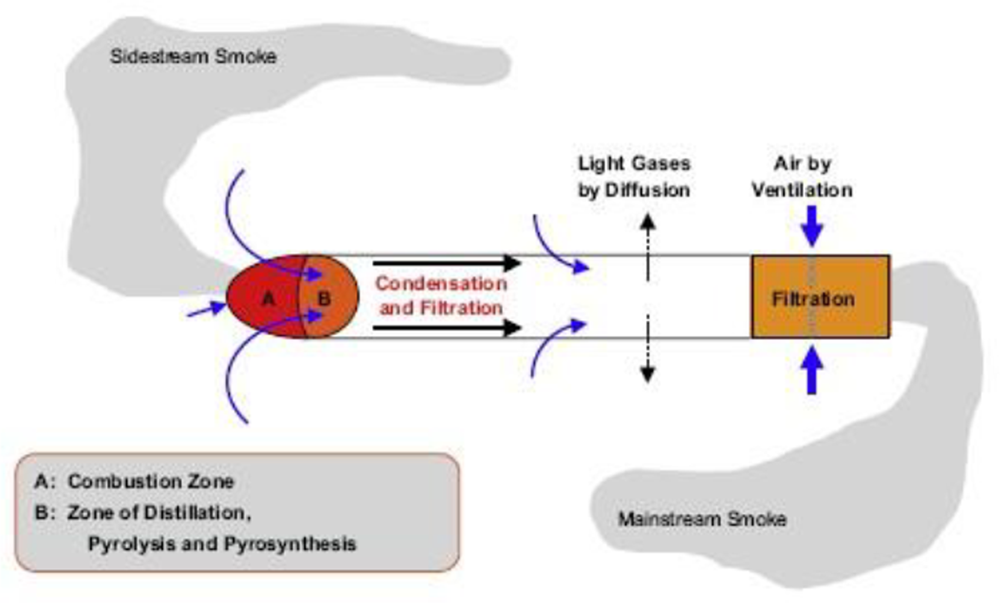
Difference between ETS and MSS
Ageing
2. Results and Discussion
Overview of ETS Markers
2.1. Exhaled MainStream Smoke (EMSS) Oriented Studies (Cigarette and Hookah)
2.2. Epidemiological Studies Approaching Hookah ETS
Middle East Studies
Indian Studies
2.3. Studies on Particles
Overview
“1) Direct gas deposition (DGD) of the portion of the compound that is initially in the gas phase of the inhaled smoke; 2) evaporative gas deposition (EGD) of PM-phase compound by evaporation to the gas phase, then deposition; (3) particle deposition, evaporation from the deposited particle, then deposition from the gas phase (PDE); and (4) particle deposition with diffusion (PDD) into RT tissue. He adds that “Three of the mechanisms (DGD, EGD, and PDE) involve volatilisation from the PM phase. The relative importance of all the mechanisms is therefore greatly affected by the volatility of the compound from the PM phase as it is set by the compound’s gas/particle partitioning constant K(p) through the compound’s vapour pressure. For a largely non-volatile compound such as benzo[a]pyrene, only PDD will likely be important. For a semi-volatile compound such as nicotine, all four mechanisms can be important” [83].
In Situ Measurements
Comparison with Cigarettes
UFP (Ultra-Fine Particles)
Swiss Experiment
French Experiment
US Experiment
Particle Growth
2.4. Studies on Specific Chemicals
Nicotine
Carbon Monoxide
CO Intoxication (Cigarette and Hookah)
Carbonyls (Aldehydes)
Recent and Older Studies on Aldehydes in Hookah MSS
2.5. Other Substances (PAHs, Phenols, Benzene, Toluene, NOx, Heavy Metals, etc.)
PAHs (Polycyclic Aromatic Hydrocarbons)
Phenols
Benzene and Toluene
Nitric Oxides
Heavy Metals
Nitrosamines
Acetone and 2-butanone
Radiotoxic Elements
Miscellanea
2.6. Further Discussion
Effect of Water Solubility of Smoke Constituents
Glycerol
Ventilation
Ageing of Smoke
Dilution
The Case of the Hookah Lounges
Pregnant Women and Children
3. Methods
Eligibility Criteria
Search Strategy
Study Selection, Data Collection and Analysis
Limits Set on this Review
4. Conclusions
- hookah smoke is made up of a large amount of glycerol and water (probably around 80% or more) and that these two substances are harmless;
- exposed non-smokers to hookah smoke would retain in their respiratory tract 11–59% of the remaining (EMSS) particulate matter and 71–81% of nicotine;
- exhaled CO measured in non-smokers exposed to hookah ETS in different settings (cafes, hookah lounges) and countries does not vary;
- the respiratory tract of active hookah smokers would retain up to 95% of the main aldehydes which are known to be water soluble and, consequently, also stopped to an unknown proportion in the water vessel of the hookah.
Glossary
Competing interests
References
- Chaouachi, K. The medical consequences of narghile (hookah, shisha) use in the world. Rev. Epidemiol. Sante Publique 2007, 55, 165–170. [Google Scholar]
- Chaouachi, K. Tout savoir sur le narguilé. Société, culture, histoire et santé; [Eng.: Everything about Hookahs. Society, Culture, Origins and Health Aspects]Maisonneuve et Larose: Paris, France, 2007. [Google Scholar]
- Salameh, P; Waked, M; Aoun, Z. Water pipe smoking: Construction and validation of the Lebanon Waterpipe Dependence Scale (LWDS-11). Nicotine Tob. Res 2008, 10, 149–158. [Google Scholar]
- Chaouachi, K. A Critique of the WHO’s TobReg “Advisory Note” entitled: “Waterpipe Tobacco Smoking: Health Effects, Research Needs and Recommended Actions by Regulators. J. Negat. Result. Biomed 2006, 5, 17. [Google Scholar]
- Chaouachi, K. Le narguilé: analyse socio-anthropologique. Culture, convivialité, histoire et tabacologie d’un mode d’usage populaire du tabac; [Narghile (hookah): a Socio-Anthropological Analysis. Culture, Conviviality, History and Tobaccology of a Popular Tobacco Use Mode]. Transdisciplinary doctoral thesis, UniversitéParis X: Paris, France, 2000. [Google Scholar]
- Chaouachi, K. Tetralogy on Narghile (Hookah, Shisha) and Health. Part 1: Presentation (Tabaccologia 2005; 1, 39–47); Part 2: Chemistry (Tabaccologia 2005; 3, 27–33); Part 3: Diseases (Tabaccologia 2006; 1, 27–34); Part 4: Public Health and Prevention (Tabaccologia 2006; 4, 29–38. In Tabaccologia; SITAB (the official Journal of the Italian Society of Tobaccology): Bologna, Italy, 2005–2006. [Google Scholar]
- Khater, AE; Abd El-Aziz, NS; Al-Sewaidan, HA; Chaouachi, K. Radiological hazards of Narghile (hookah, shisha, goza) smoking: activity concentrations and dose assessment. J. Environ. Radioact 2008, 99, 1808–1814. [Google Scholar]
- Sajid, KM; Chaouachi, K; Mahmood, R. Hookah smoking and cancer. Carcinoembryonic Antigen (CEA) levels in exclusive/ever hookah smokers. Harm Reduct. J 2008, 24, 19. [Google Scholar]
- Prignot, JJ; Sasco, AJ; Poulet, E; Gupta, PC; Aditama, TY. Alternative forms of tobacco use. Int. J. Tuberc. Lung Dis 2008, 12, 718–727. [Google Scholar]
- Pande, BR. Hubble-bubble Smoking. Brit. Med. J 1962, 1, 1556. [Google Scholar]
- Stolerman, IP; Stenius, K. The language barrier and institutional provincialism in science. Drug Alcohol Dependence 2008, 92, 1–2. [Google Scholar]
- Horton, R. Medical journals: evidence of bias against the diseases of poverty. Lancet 2003, 361, 712–713. [Google Scholar]
- Molimard, R. Le rapport Européen Lifting the SmokeScreen: Etude épidémiologique ou manipulation? [The European Report “Lifting the SmokeScreen”: Epidemiological study or manipulation?]. Rev. Epidemiol. Sante Publique 2008, 56, 286–290. [Google Scholar]
- Bacha, ZA; Salameh, P; Waked, M. Saliva Cotinine and Exhaled Carbon Monoxide Levels in Natural Environment Waterpipe Smokers. Inhal. Toxicol 2007, 19, 771–777. [Google Scholar]
- Al Mutairi, SS; Mojiminiyi, OA; Shihab-Eldeen, AA; Al Sharafi, A; Abdella, N. Effect of smoking habit on circulating adipokines in diabetic and non-diabetic subjects. Ann. Nutr. Metab 2008, 52, 329–334. [Google Scholar]
- Al-Numair, K; Barber-Heidal, K; Al-Assaf, A; El-Desoky, G. Water-pipe (shisha) smoking influences total antioxidant capacity and oxidative stress of healthy Saudi males. J. Food Agricul. Environ 2007, 5, 17–22. [Google Scholar]
- Ourari, B; Zouaoui, A; Mehiri, N; Cherif, J; Khalsi, S; Enaifer, E; Daghfous, J; Louzir, B; Boubaker, S; Beji, M. Cytologie alvéolaire et fonction respiratoire chez le consommateur de narguilé [Lung Cell profile and lung function in narghile smokers]. Rev. Mal. Respir 2006, 23, 86. [Google Scholar]
- Mohammad, Y; Kakah, M; Mohammad, Y. Chronic respiratory effect of narguileh smoking compared with cigarette smoking in women from the East Mediterranean region. Int. J. Chron. Obstruct. Pulmon Dis 2008, 3, 405–414. [Google Scholar]
- Mohammad, Y. Les dangers du narguilé [Narghile Hazards]. Info Resp 2000, 36, 24. [Google Scholar]
- Chaouachi, K. Hookah (Narghile, Shisha) Smoking and Communicable Diseases. Tabaccologia 2008, 1, 47. [Google Scholar]
- Chaouachi, K. The narghile (hookah, shisha, goza) epidemic and the need for clearing up confusion and solving problems related with model building of social situations. TheScientificWorldJOURNAL 2007, 7, 1691–1696. [Google Scholar]
- El-Roueiheb, Z; Tamim, H; Kanj, M; Jabbour, S; Alayan, I; Musharrafieh, U. Cigarette and waterpipe smoking among Lebanese adolescents, a cross-sectional study, 2003–2004. Nicotine Tob. Res 2008, 10, 309–314. [Google Scholar]
- Tamim, H; Al-Sahab, B; Akkary, G; Ghanem, M; Tamim, N; Roueiheb, ZE; Kanj, M; Afifi, R. Cigarette and Nargileh Smoking Practices Among School Students in Beirut, Lebanon. Am. J. Health Behav 2007, 31, 56–63. [Google Scholar]
- Schumacher, JN; Green, CR; Best, FW; Newell, MP. Smoke composition. An extensive investigation of the water-soluble portion of cigarette smoke. J. Agric. Food Chem 1977, 25, 310–320. [Google Scholar]
- El-Aasar, AM; El-Merzabani, MM. Studies on Jurak Smoke. I. The Organic Constitutents of Jurak Smoke. J. King Abdulaziz University (Science) 1991, 3, 169–181. [Google Scholar]
- Thielen, A; Klus, H; Müller, L. Tobacco smoke: unraveling a controversial subject. Exp. Toxicol. Pathol 2008, 60, 141–156. [Google Scholar]
- Deckers, SK; Farley, J; Heath, J. Tobacco and its trendy alternatives: implications for pediatric nurses. Crit. Care Nurs. Clin. North Am 2006, 18, 95–104. [Google Scholar]
- WHO-EMRO (Eastern Mediterranean Regional Office) and ESPRI (Egyptian Smoking Prevention Research Institute). Shisha Hazards Profile “Tobacco Use in Shisha - Studies on Water-pipe Smoking in Egypt”; Mohamed, MK, Loffredo, CA, Israel, E, Eds.; WHO: Geneva/Cairo, 2007; p. 84. [Google Scholar]
- Gupta, D; Aggarwal, AN; Jindal, SK. Pulmonary effects of passive smoking: the Indian experience. Tob. Induc. Dis 2002, 1, 129–136. [Google Scholar]
- Gori, GB; Mantel, N. Mainstream and environmental tobacco smoke. Regul. Toxicol. Pharmacol 1991, 14, 88–105. [Google Scholar]
- Adlkofer, F. Lung cancer due to passive smoking--a review. Int. Arch. Occup. Environ. Health 2001, 74, 231–241. [Google Scholar]
- IARC (International Agency for Research on Cancer). Monographs on the Evaluation of Carcinogenic Risks to Humans. Tobacco Smoke and Involuntary Smoking. Vol. 83; IARC Press: Lyon, France, 2004. [Google Scholar]
- California Environmental Protection Agency. Air Resources Board “Proposed Identification of Environmental Tobacco Smoke as a Toxic Air Contaminant”. Tob Control. 2005.
- US Surgeon General. The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General; Department of Health: Washington, D.C., USA, 2006. [Google Scholar]
- WHO (World Health Organization). TFI (Tobacco Free Initiative). “Rigorous Research Leaves No Doubt...”; WHO: Geneva, Switzerland, 2008.
- Scherer, G. Biomonitoring of inhaled complex mixtures--ambient air, diesel exhaust and cigarette smoke. Exp. Toxicol. Pathol 2005, 57, 75–110. [Google Scholar]
- ENSP (European Network For Smoking Prevention). Second-Hand Smoke (SHS) Markers. Review of methods for monitoring exposure levels; ENSP: Brussels, Belgium, 2005. [Google Scholar]
- Huber, GL; Brockie, RE; Mahajan, VK. Smoke and Mirrors: The EPA ’s Flawed Study of Environmental Tobacco Smoke and Lung Cancer. Regulation. The Cato Review of Business & Government. 1993, p. 3.
- US EPA (Environmental Protection Agency). Respiratory health effects of passive smoking: lung cancer and other disorders: the report of the U.S. Environmental Protection Agency; Smoking and Tobacco Control Monograph 4National Cancer Institute: Bethesda, MD, US, 1993. [Google Scholar]
- Boffetta, P; Agudo, A; Ahrens, W; Benhamou, E; Benhamou, S; Darby, SC; Ferro, G; Fortes, C; Gonzalez, CA; Jöckel, KH; Krauss, M; Kreienbrock, L; Kreuzer, M; Mendes, A; Merletti, F; Nyberg, F; Pershagen, G; Pohlabeln, H; Riboli, E; Schmid, G; Simonato, L; Trédaniel, J; Whitley, E; Wichmann, HE; Winck, C; Zambon, P; Saracci, R. Multicenter case-control study of exposure to environmental tobacco smoke and lung cancer in Europe. J. Natl. Cancer Inst 1998, 90, 1440–1150. [Google Scholar]
- Vineis, P; Airoldi, L; Veglia, F; Olgiati, L; Pastorelli, R; Autrup, H; Dunning, A; Garte, S; Gormally, E; Hainaut, P; Malaveille, C; Matullo, G; Peluso, M; Overvad, K; Tjonneland, A; Clavel-Chapelon, F; Boeing, H; Krogh, V; Palli, D; Panico, S; Tumino, R; Bueno-De-Mesquita, B; Peeters, P; Berglund, G; Hallmans, G; Saracci, R; Riboli, E. Environmental tobacco smoke and risk of respiratory cancer and chronic obstructive pulmonary disease in former smokers and never smokers in the EPIC prospective study. BMJ 2005, 330, 277. [Google Scholar]
- Klepeis, NE; Ott, WR; Switzer, P. Real-time measurement of outdoor tobacco smoke particles. J. Air Waste Manag. Assoc 2007, 57, 522–534. [Google Scholar]
- Brewis, J; Grey, C. The regulation of smoking at work. Hum. Relat 2008, 67, 965–987. [Google Scholar]
- Sargent, RP; Shepard, RM; Glantz, SA. Reduced incidence of admissions for myocardial infarction associated with public smoking ban: before and after study. BMJ 2004, 328, 977–980. [Google Scholar]
- Kabat, G. Effect of public smoking ban in Helena, Montana: When results look too good to be true, they probably are. BMJ 2004, 328, 1379. [Google Scholar]
- Snowdon, C. Health fears go up in smoke; Spiked online: London, UK, December 2 2008; Available at http://www.spiked-online.com/index.php?/site/article/5988/(accessed December 12, 2008). [Google Scholar]
- Gori, GB. Environmental tobacco smoke and coronary heart syndromes: absence of an association. Regul. Toxicol. Pharmacol 1995, 21, 281–295. [Google Scholar]
- Siegel, M. Is the tobacco control movement misrepresenting the acute cardiovascular health effects of secondhand smoke exposure? An analysis of the scientific evidence and commentary on the implications for tobacco control and public health practice. Epidemiologic Perspective. Innov 2007, 4, 12. [Google Scholar]
- Lee, PN; Forey, BA. Environmental tobacco smoke exposure and risk of stroke in nonsmokers: a review with meta-analysis. J. Stroke Cerebrovasc. Dis 2006, 15, 190–201. [Google Scholar]
- Enstrom, JE; Kabat, GC. Environmental tobacco smoke and tobacco related mortality in a prospective study of Californians, 1960–98. BMJ 2003, 326, 1057. [Google Scholar]
- Enstrom, JE. Defending legitimate epidemiologic research: combating Lysenko pseudoscience. Epidemiologic Perspective. Innov 2007, 4, 11. [Google Scholar]
- Ungar, S; Bray, D. Silencing science: partisanship and the career of a publication disputing the dangers of secondhand smoke. Publ. Underst. Sci 2005, 14, 5–23. [Google Scholar]
- The Smoke Free Partnership [for the European Respiratory Society, INCa (Institut National du Cancer), Cancer Research UK, European Heart Network].
- WHO (World Health Organization). Report: Smoke-Free Inside. World No-Tobacco Day 2007; WHO: Geneva, Switzerland, 2007; p. 3.
- WHO TobReg World Health Organization. Study Group on Tobacco Product Regulation (TobReg). Waterpipe Tobacco Smoking: Health Effects, Research Needs and Recommended Action by Regulators; WHO TobReg: Geneva, Switzerland, 2005.
- Maziak, W; Ward, KD; Afifi Soweid, RA; Eissenberg, T. Tobacco smoking using a waterpipe: a re-emerging strain in a global epidemic. Tob. Control 2004, 13, 327–333. [Google Scholar]
- Scherer, G; Conze, C; Tricker, AR; Adlkofer, F. Uptake of tobacco smoke constituents on exposure to environmental tobacco smoke (ETS). Clin. Invest 1992, 70, 352–367. [Google Scholar]
- Moldoveanu, SC; Coleman, W; Wilkins, J. Determination of Carbonyl Compounds in Exhaled Cigarette Smoke. Beitr. Tabakforsch. Int 2007, 22, 346–357. [Google Scholar]
- Borgerding, M; Klus, H. Analysis of complex mixtures--cigarette smoke. Exp. Toxicol. Pathol 2005, 57, 43–73. [Google Scholar]
- Schick, S; Glantz, S. Philip Morris toxicological experiments with fresh sidestream smoke: more toxic than mainstream smoke. Tob. Control 2005, 14, 396–404. [Google Scholar]
- Bernstein, DM. A review of the influence of particle size, puff volume, and inhalation pattern on the deposition of cigarette smoke particles in the respiratory tract. Inhal. Toxicol 2004, 16, 675–689. [Google Scholar]
- Ingebrethsen, B. Evolution of the particle size distribution of mainstream cigarette smoke during a puff. Aerosol. Sci. Technol 1986, 5, 423–433. [Google Scholar]
- Tamim, H; Akkary, G; El-Zein, A; El-Roueiheb, Z; El-Chemaly, S. Exposure of pre-school children to passive cigarette and narghile smoke in Beirut. Eur. J. Public Health 2006, 16, 509–512. [Google Scholar]
- Tamim, H; Musharrafieh, U; El-Roueiheb, Z; Yunis, K; Almawi, WY. Exposure of children to environmental tobacco smoke (ETS) and its association with respiratory ailments. J. Asthma 2003, 40, 571–576. [Google Scholar]
- Moldoveanu, SC. Determination of Polycyclic Aromatic Hydrocarbons in Exhaled Cigarette Smoke. Beitr. Tabakforsch. Int 2008, 23, 85–97. [Google Scholar]
- Moldoveanu, SC; Coleman, W; Wilkins, J. Determination of Benzene and Toluene in Exhaled Cigarette Smoke. Beitr. Tabakforsch. Int 2008, 23, 107–114. [Google Scholar]
- Moldoveanu, SC; Coleman, W; Wilkins, J. Determination of Hydroxybenzenes in Exhaled Cigarette Smoke. Beitr. Tabakforsch. Int 2008, 23, 98–106. [Google Scholar]
- Moldoveanu, SC; St. Charles, FK. Differences in the Chemical Composition of the Particulate Phase of Inhaled and Exhaled Cigarette Mainstream Smoke. Beitr. Tabakforsch. Int 2006, 22, 290–302. [Google Scholar]
- Morawska, L; Zhang, JJ. Combustion sources of particles. 1. Health relevance and source signatures. Chemosphere 2002, 49, 1045–1058. [Google Scholar]
- Jarvis, MJ. Uptake of environmental tobacco smoke. IARC Sci. Publ 1987, 81, 43–58. [Google Scholar]
- Benowitz, NL. Biomarkers of environmental tobacco smoke exposure. Environ. Health Perspect 1999, 107, 349–355. [Google Scholar]
- Hinds, W; First, MW; Huber, GL; Shean, JW. A method for measuring respiratory deposition of cigarette smoke during smoking. Am. Ind. Hyg. Assoc. J 1983, 44, 113–118. [Google Scholar]
- Baker, RR; Dixon, M. The retention of tobacco smoke constituents in the human respiratory tract. Inhal. Toxicol 2006, 17, 255–294. [Google Scholar]
- Rylander, R. Environmental Tobacco Smoke Effects on the Non-Smoker. Workshop (Bermuda, March 27–29, 1974)University of Geneva: Geneva, Switzerland, 1974. [Google Scholar]
- Al-Haddad, NM; Hamadeh, RR; Bahram, SA. Public knowledge and attitudes towards passive smoking. Saudi Med. J 2005, 26, 2004–2006. [Google Scholar]
- Maziak, W; Ward, KD; Rastam, S; Mzayek, F; Eissenberg, T. Extent of exposure to environmental tobacco smoke (ETS) and its dose-response relation to respiratory health among adults. Respir. Res 2005, 6, 13. [Google Scholar]
- Maziak, W; Ward, KD; Eissenberg, T. Measuring exposure to environmental tobacco smoke (ETS): a developing country’s perspective. Prev. Med 2006, 42, 409–414. [Google Scholar]
- Gupta, D; Aggarwal, AN; Chaudhry, K; Chhabra, SK; D’Souza, GA; Jindal, SK; Katiyar, SK; Kumar, R; Shah, B; Vijayan, VK. Household environmental tobacco smoke exposure, respiratory symptoms and asthma in non-smoker adults: a multicentric population study from India. Indian J. Chest Dis. Allied Sci 2006, 48, 31–36. [Google Scholar]
- Dhar, GM; Shah, GN; Naheed, B; Hafiza. Epidemiological trend in the distribution of cancer in Kashmir Valley. J Epidemiol. Community Health 1993, 47, 290–292. [Google Scholar]
- Rapiti, E; Jindal, SK; Gupta, D; Boffetta, P. Passive smoking and lung cancer in Chandigarh, India. Lung Cancer 1999, 23, 183–189. [Google Scholar]
- Goel, P; Radotra, A; Singh, I; Aggarwal, A; Dua, D. Effects of passive smoking on outcome in pregnancy. J. Postgrad. Med 2004, 50, 12–16. [Google Scholar]
- Jindal, SK; Aggarwal, AN; Chaudhry, K; Chhabra, SK; Souza, GA; Gupta, D; Katiyar, SK; Kumar, R; Shah, B; Vijayan, VK; Asthma Epidemiology Study Group. A multicentric study on epidemiology of chronic obstructive pulmonary disease and its relationship with tobacco smoking and environmental tobacco smoke exposure. Indian J. Chest Dis. Allied Sci 2006, 48, 23–29. [Google Scholar]
- Pankow, JF. A consideration of the role of gas/particle partitioning in the deposition of nicotine and other tobacco smoke compounds in the respiratory tract. Chem. Res. Toxicol 2001, 14, 1465–1481. [Google Scholar]
- Gardner, DE. A Review of “Particle Toxicology”. Inhal. Toxicol 2007, 19, 787–788. [Google Scholar]
- Maziak, W; Ali, RA; Fouad, MF; Rastam, S; Wipflin, H; Travers, MJ; Ward, KD; Eissenberg, T. Exposure to secondhand smoke at home and in public places in Syria: a developing country’s perspective. Inhal. Toxicol 2008, 20, 17–24. [Google Scholar]
- Mohamed, MK; Momen, M; Hyland, A; El Setouhy, M; Travers, MJ; Loffredo, CA. Measurement of PM2.5 as a marker for passive exposure to water pipe in cafes in Egypt.
- Buchholtz, C. Indoor air pollution due to hookah smoking: particulate concentrations in a lexington, kentucky hookah lounge Public Health without Borders. APHA 136th Annual Meeting and Expo, San Diego, California, USA, October 25–29, 2008.
- Maziak, W; Rastam, S; Ibrahim, I; Ward, KD; Eissenberg, T. Waterpipe associated particulate matter emissions. Nicotine Tob. Res 2008, 10, 519–523. [Google Scholar]
- McCusker, K; Hiller, FC; Wilson, JD; Mazumder, MK; Bone, R. Aerodynamic sizing of tobacco smoke particulate from commercial cigarettes. Arch. Environ. Health 1983, 38, 215–218. [Google Scholar]
- Jaques, PA; Kim, CS. Measurement of total lung deposition of inhaled ultrafine particles in healthy men and women. Inhal. Toxicol 2000, 12, 715–731. [Google Scholar]
- Anderson, PJ; Wilson, JD; Hiller, FC. Particle size distribution of mainstream tobacco and marijuana smoke. Analysis using the electrical aerosol analyzer. Am. Rev. Respir. Dis 1989, 140, 202–205. [Google Scholar]
- Monn, C; Kindler, P; Meile, A; Brändli, O. Ultrafine particle emissions from waterpipes. Tob. Control 2007, 16, 390–393. [Google Scholar]
- Becquemin, MH; Bertholon, JF; Attoui, M; Roy, F; Roy, M; Dautzenberg, B. [Particle size in water pipe smoke]. Rev. Mal. Respir 2008, 25, 839–846. [Google Scholar]
- Brinkman, M; Gordon, S; Chuang, J; Kroeger, R. Distribution, deposition, and chemical speciation of mainstream smoke particles in respiratory tract of smokers [ISEE/ISEA 2006 Conference Abstracts Supplement]. Poster/Abstract. Epidemiology 2006, 17, S294. [Google Scholar]
- McCusker, K; Hiller, C; Mazumder, M; Bone, R. Dynamic growth of cigarette smoke particles. Chest 1981, 80, 3. [Google Scholar]
- Richardson, RB. The growth in a humid environment of smoke particles produced by various cigarettes; British American Tobacco: London, UK, 1976; (cited by Baker & Dixon). [Google Scholar]
- Jones, RT. Measurements of exhaled smoke particles; British American Tobacco: London, UK, 1976; (cited by Baker & Dixon). [Google Scholar]
- Iwase, A; Aiba, M; Kira, S. Respiratory nicotine absorption in non-smoking females during passive smoking. Int. Arch. Occup. Environ. Health 1991, 63, 139–143. [Google Scholar]
- Feng, S; Plunkett, SE; Lam, K; Kapur, S; Muhammad, R; Jin, Y; Zimmermann, M; Mendes, P; Kinser, R; Roethig, HJ. A new method for estimating the retention of selected smoke constituents in the respiratory tract of smokers during cigarette smoking. Inhal. Toxicol 2007, 19, 169–179. [Google Scholar]
- Scherer, G; Conze, C; von Meyerinck, L; Sorsa, M; Adlkofer, F. Importance of exposure to gaseous and particulate phase components of tobacco smoke in active and passive smokers. Int. Arch. Occup. Environ. Health 1990, 62, 459–466. [Google Scholar]
- Jarvis, MJ; Russell, MA; Feyerabend, C. Absorption of nicotine and carbon monoxide from passive smoking under natural conditions of exposure. Thorax 1983, 38, 829–833. [Google Scholar]
- Sajid, KM; Akther, M; Malik, GQ. Carbon monoxide fractions in cigarette and hookah. J. Pak. Med. Assoc 1993, 43, 179–182. [Google Scholar]
- Molimard, R. Le tabac sans fumée ou snus, une réduction des risques liés au tabagisme [Smokeless tobacco or snus, a tobacco harm reduction]. Le Courrier des Addictions 2005, 7, 52–55. [Google Scholar]
- El-Nachef, WN; Hammond, SK. Exhaled carbon monoxide with water pipe use in US students. JAMA 2008, 299, 36–38. [Google Scholar]
- Russell, MA; Cole, PV; Brown, E. Absorption by non-smokers of carbon monoxide from room air polluted by tobacco smoke. Lancet 1973, 1, 576–579. [Google Scholar]
- Guillerm, R. Les Cahiers Sandoz 1969, 15, 33–34.
- Al-Moamary, MS; Al-Shammary, AS; Al-Shimemeri, AA; Ali, MM; Al-Jahdali, HH; Awada, AA. Complications of carbon monoxide poisoning. Saudi Med. J 2000, 21, 361. [Google Scholar]
- Levant, A; Cabot, C; Genestal, M; Georges, M; Letourmy, F. Intoxication aiguë au CO par narguilé. Poster, 22e Journee de Tabacologie, Paris, France, October 7, 2006.
- Al-Safi, SA; Ayoub, NM; Albalas, MA; Al-Doghim, I; Aboul-Enein, FH. Does shisha smoking affect blood pressure and heart rate? J. Public Health 2008. [Google Scholar]
- Shafagoj, YA; Mohammed, FI. Levels of Maximum End-Expiratory Carbon Monoxide and Certain Cardiovascular Parameters Following Hubble-Bubble Smoking. Saudi Med. J 2002, 23, 953–958. [Google Scholar]
- Higenbottam, T; Siddons, T; Demoncheaux, E. The direct and indirect action of inhaled agents on the lung and its circulation: lessons for clinical science. Environ. Health Perspect 2001, 109, 559–562. [Google Scholar]
- Al Rashidi, M; Shihadeh, A; Saliba, NA. Volatile aldehydes in the mainstream smoke of the narghile waterpipe. Food Chem. Toxicol 2008, 46, 3546–3549. [Google Scholar]
- Guillerm, R; Badré, R; Vignon, B. Effet inhibiteurs de la fumée de tabac sur l’activité ciliaire de l’épithélium respiratoire et nature des composants responsables [Inhibitory effects of tobacco smoke on the respiratory epithelium ciliary activity]. Académie Nationale de Médecine 1961, 13, 416–423. [Google Scholar]
- Huber, GL; First, MW; Grubner, O. Marijuana and tobacco smoke gas-phase cytotoxins. Pharmacol. Biochem. Behav 1991, 40, 629–636. [Google Scholar]
- Lee, PN. Smoking “attributable” mortality in India. Some relevant considerations.
- El-Aasar, AM; El-Merzabani, MM; Ba-Akel, H. Studies on Jurak Smoke: II. The Metallic Constituents of Jurak Paste and Jurak Smoke. J. King Abdulaziz University (Science) 1991, 3, 183–188. [Google Scholar]
- Hoffmann, D; Rathkamp, G; Wynder, EL. Comparison of the Yields of Several Selected Components in the Smoke from Different Tobacco Products. J. Natl. Cancer Inst 1963, 31, 627–637. [Google Scholar]
- Sukumar, A; Subramanian, R. Elements in hair and nails collected from residents from a village adjacent to New Delhi. Influence of place of occupation and smoking habits. Biol. Trace Elem. Res 1992, 34, 99–105. [Google Scholar]
- Richter, E. NNK is not insoluble in water. Inhal. Toxicol 2007, 19, 591. [Google Scholar]
- Zaga, V; Gatta-vecchia, E. Radicali liberi e fumo di sigaretta [Free radicals and cigarette smoke]. Giorn. It. Mal. Tor 2002, 56, 375–391. [Google Scholar]
- Sutherland, G; Russell, MA; Stapleton, JA; Feyerabend, C. Glycerol particle cigarettes: a less harmful option for chronic smokers. Thorax 1993, 48, 385–387. [Google Scholar]
- Repace, JL; Hyde, JN; Brugge, D. Air pollution in Boston bars before and after a smoking ban. BMC Public Health 2006, 6, 266. [Google Scholar]
- Higenbottam, T; Shipley, MJ; Rose, G. Cigarettes, lung cancer, and coronary heart disease: the effects of inhalation and tar yield. J. Epidemiol. Community Health 1982, 36, 113–117. [Google Scholar]
- Huber, GL. Physical, chemical, and biologic properties of tobacco, cigarette smoke, and other tobacco products. Semin. Respir. Med 1989, 10, 297–332. [Google Scholar]
- Mirahmadizadeh, A; Nakhaee, N. Prevalence of waterpipe smoking among rural pregnant women in Southern Iran. Med. Princ. Pract 2008, 17, 435–439. [Google Scholar]
- Nuwayhid, IA; Yamout, B; Azar, G; Kambris, M. Narghile (Hubble-Bubble) Smoking, Low Birth Weight, and other Pregnancy Outcomes. Am. J. Epidemiol 1998, 148, 375–383. [Google Scholar]
- Sulaiman, MI. Effects of prenatal exposure to sheesha smoke - response to juvenile rats to novel environment. Inhal. Toxicol 1993, 5, 313–322. [Google Scholar]
- Smith, R. Comment from the editor. BMJ 2003, 327, 505. [Google Scholar]
- Pechacek, TF; Babb, S. How acute and reversible are the cardiovascular risks of secondhand smoke? BMJ 2004, 328, 980–983. [Google Scholar]
- Winickoff, JP; Friebely, J; Tanski, SE; Sherrod, C; Matt, GE; Hovell, MF; McMillen, RC. Beliefs About the Health Effects of “Thirdhand” Smoke and Home Smoking bans. Pediatrics 2009, 123, e74–e79. [Google Scholar]
- Eclipse Expert Panel. A safer cigarette? A comparative study. A consensus report. Inhal. Toxicol 2000, 12, 1–58. [Google Scholar]
- Tricker, AR; Schorp, MK; Urban, HJ; Leyden, D; Hagedorn, HW; Engl, J; Urban, M; Riedel, K; Gilch, G; Janket, D; Scherer, G. Comparison of Environmental Tobacco Smoke (ETS) Concentrations Generated by an Electrically Heated Cigarette Smoking System and a Conventional Cigarette. Inhal. Toxicol 2009, 21, 62–77. [Google Scholar]
- Frost-Pineda, K; Zedler, BK; Liang, Q; Roethig, HJ. Environmental tobacco smoke (ETS) evaluation of a third-generation electrically heated cigarette smoking system (EHCSS). Regul. Toxicol. Pharmacol 2008, 52, 118–121. [Google Scholar]
- Kabat, GC. Hyping health risks: environmental hazards in daily life and the science of epidemiology; Columbia University Press: New York, USA, 2008. [Google Scholar]
Abbreviations
| CI: | Confidence Interval; |
| EMSS: | Exhaled Main-Stream Smoke; |
| ETS: | Environmental Tobacco Smoke (taken as synonym of SHS); |
| MSS: | Main-Stream Smoke; |
| OTS | (Outdoors Tobacco Smoke); |
| OR: | Odds Ratio; |
| PM2.5: | Particle Matter whose size is below 2.5 μm); |
| PM10: | Particle Matter whose size is below 10 μm): |
| PAH: | Polycyclic Aromatic Hydrocarbons; |
| RSP: | Respirable Suspended Particles; |
| SHS: | Second Hand Smoke (syn. ETS); |
| SSS: | Side-Stream Smoke; |
| UFP: | Ultra Fine Particles; |
| WHO | (World Health Organisation). |





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Concentration of particles
(millions per mL [median Ø]) | Cigarette | Narghile |
|---|---|---|
| MSS | 3.14 [0.27 μm] | 3.55 [0.34 μm]
(before water bubbling) 1.20 [0.27 μm] (after water bubbling) |
| SSS | 19 [0.09 μm] | 2.91 [0.11 μm] |
| EMSS (machine) | 2.26[0.30 μm] | 6.22 [0.25 μm] |
| Aerodynamic size and filter efficiency of smoke from commercial cigarettes | |||||||
|---|---|---|---|---|---|---|---|
| Cigarette | Filter type | FTC tar ratinga(mg/cig) | MMAD (μm) with filter | MMAD (μm) without filter | Number/cm3 with filter (103) | Number/cm3 without filter (103) | Filter efficiency (%) |
| IR2F | Cell. acetate | 26 | 0.44 | 0.43 | 3.3 | 4.2 | 22 |
| Marlboro | Cell. acetate | 17 | 0.43 | 0.48 | 3.1 | 4.5 | 32 |
| Tareyton | Cell. acetate + charcoal particles | 14 | 0.50 | 0.47 | 1.6 | 4.0 | 60 |
| Doral II | Cell. acetate + plastic baffles | 5 | 0.50 | 0.48 | 1.9 | 4.4 | 57 |
| Koolite | Cell. acetate | 5 | 0.43 | 0.38 | 1.6 | 3.9 | 60 |
| Merit | Cell. acetate | 8 | 0.36 | 0.38 | 2.1 | 3.9 | 46 |
| Vantage | Cell. acetate | 11 | 0.47 | 0.48 | 2.7 | 5.0 | 46 |
| Cambridge | Cell. acetate | <1 | 0.53 | 0.51 | 0.25 | 4.67 | 96 |
| Barclay | Cell. acetate + vent.holes | <1 | 0.56 | 0.36 | 0.57 | 5.9 | 91 |
| Carlton | Cell. acetate + vent.holes | <1 | 0.43 | 0.36 | 0.33 | 5.3 | 94 |
| Barclay | Vent.holes taped | – | 4.90 | ||||
| Carlton | Vent.holes taped | – | 2.37 | ||||
| Tobacco smoke constituents | Smoking (S)(20cig/day)b | Passive smoking (PS)(8h/day)c | Dose ratio S/PS |
|---|---|---|---|
| GASEOUS PHASE | |||
| CO (mg) | 40–400 | 14.4–96 | 2.7–4.2 |
| Formaldehyde (mg) | 0.4–1.8 | 0.08–0.4 | 4–5 |
| Volatile nitrosamines (μg) | 0.05–1.0 | 0.03–0.4 | 1.5–2.5 |
| Benzene (μg) | 200–1200 | 40–400 | 3–5 |
| PARTICULATE MATTER | |||
| Particles (mg) | 75–300 | 0.024–0.24 | 1250–3000 |
| Nicotine (mg) d | 7.5–30 | 0.08–0.4 | 75–90 |
| Benzo[a]pyrene (μg) | 0.15–0.75 | 0.001–0.011 | 70–150 |
| Cadmium (μg) | 1.5 | 0.001–0.014 | 110–1500 |
| Tobacco specific nitrosamines (μg) | 4.5–45 | 0.002–0.010 | 2300–4500 |
| The 15 Reasons behind the World Upsurge in Hookah (Narghile, Shisha) Smoking |
|---|
| OBECTIVE REASONS |
| 1-Global Tourism and Migration Flows (back from Egypt, Tunisia, etc. with a hookah in the suitcase; hookah lounges in the West) |
| 2- A New Hassle-Free Lighting System (new easy to light charcoal) |
| 3-Relative Acceptance by Non-Smokers (notable smoke irritants filtered out) |
| 4-Unexepected Backlash Effect of Anti-Tobacco Campaigns (viewed as safer than cigarette smoking) |
| 5-Filtration of Some Noxious Substances (some carcinogens, among others, may be filtered out) |
| 6-A “Light” Dependence (seen as easy to quit) |
| 7-The Influence of Television (case of the Arab World) (Egyptian movies have featured hookah smokers for decades) |
| 8-The Rise of Individualism in Modern Societies (socialising needs and the search for new forms of sociability) |
| SUBJECTIVE REASONS |
| 9-Conviviality (“social” smoking, sharing the hose (ludens), talking, long time passing) |
| 10-A Powerful Symbolism (dream, art, “mysticism”, “peace pipe”) |
| 11-A Transverse Social, Sexual, Religious and Inter-Generational Practice (social and cultural melting pot) |
| 12-Flavours (“tobamel” (mu’assel), a flavoured tobacco (or no-tobacco)-honey/molasses based mixture) |
| 13-The Cultural Status of Honey (Koran, The Bees) |
| 14-A Highly Sensory Experience (Five senses permanently stimulated) |
| 15-“Rebellion” Values (an “anti-modern” concept of time passing in a global world. A social and cultural counter-product of the globalisation process of the Nineties) |
Share and Cite
Chaouachi, K. Hookah (Shisha, Narghile) Smoking and Environmental Tobacco Smoke (ETS). A Critical Review of the Relevant Literature and the Public Health Consequences. Int. J. Environ. Res. Public Health 2009, 6, 798-843. https://doi.org/10.3390/ijerph6020798
Chaouachi K. Hookah (Shisha, Narghile) Smoking and Environmental Tobacco Smoke (ETS). A Critical Review of the Relevant Literature and the Public Health Consequences. International Journal of Environmental Research and Public Health. 2009; 6(2):798-843. https://doi.org/10.3390/ijerph6020798
Chicago/Turabian StyleChaouachi, Kamal. 2009. "Hookah (Shisha, Narghile) Smoking and Environmental Tobacco Smoke (ETS). A Critical Review of the Relevant Literature and the Public Health Consequences" International Journal of Environmental Research and Public Health 6, no. 2: 798-843. https://doi.org/10.3390/ijerph6020798