Article Text

Abstract
BACKGROUND Inhalation therapy using a pressured metered dose inhaler (pMDI) and a spacer is frequently used in the treatment of airway disease in children. Several laboratory studies found a clear negative influence of electrostatic charge (ESC) on plastic spacers on the delivery of aerosol.
AIMS To investigate whether ESC on plastic spacers could diminish bronchodilating responses to salbutamol.
METHODS Ninety asthmatic children (aged 4–8 years) were randomised into three groups: metal Nebuchamber, plastic Volumatic, and plastic Aerochamber. The bronchodilating response was measured by the change in peak expiratory flow rate (PEF) after 100 μg and 400 μg salbutamol. Within the Volumatic and Aerochamber groups, a crossover comparison was made between electrostatic and non-electrostatic spacers.
RESULTS We found no significant effect of ESC on the bronchodilating response to salbutamol with any of the doses in the Aerochamber and Volumatic groups. For the plastic spacers, the mean difference of the change in PEF after 100 μg salbutamol between non-electrostatic and electrostatic spacers was only +1.7% (95% CI −1.3% to 4.7%). After 400 μg salbutamol this was +1.9% (95% CI −1.4% to 5.1%). A comparable efficacy was found for the Nebuchamber, the Aerochamber, and Volumatic with respect to the change in PEF after 100 and 400 μg salbutamol.
CONCLUSION This study showed no negative influence of ESC on plastic spacers with regard to clinical efficacy of a β2 agonist (salbutamol) in children with asthma. The metal Nebuchamber, plastic Aerochamber, and plastic Volumatic were equally effective.
- asthma
- spacer
- electrostatic charge
- salbutamol
Statistics from Altmetric.com
Inhalation therapy using a pressured metered dose inhaler (pMDI) combined with a spacer plays a crucial role in the treatment of young asthmatic children, patients with cystic fibrosis, and infants with bronchopulmonary dysplasia (BPD).1 ,2 Moreover, this method of administering medication is becoming increasingly important when treating adults with chronic obstructive lung disease,3 and is even effective for patients with acute exacerbations who are receiving ventilatory support.4Several types of spacers are available, for instance, Aerochamber, Babyhaler, and Volumatic (all made of polycarbonate (plastic)), and the metal Nebuchamber.5-7 In the past five years, several in vitro studies reported that the effectiveness of plastic spacers may be substantially limited by electrostatic charge (ESC).5-11Because of this charge, the aerosol may precipitate more rapidly on the spacer surface, and less medication may by available for inhalation.7 ,9 It is not clear whether ESC on plastic spacers can limit clinical efficacy of inhalation therapy in vivo. In the above mentioned studies, the amount of drug delivered from the spacer was measured by means of a filter6 or an inertial impactor connected in series with the spacer.7 ,9 ,11However, a greater drug delivery at the mouth does not necessarily lead to a larger deposition in small airways, or to a greater clinical effect in vivo.5 ,6 Whether or not ESC on plastic spacers limits the clinical efficacy of drugs in vivo, is therefore uncertain. The purpose of our study was: (1) to investigate the influence of ESC on the bronchodilating response to a β2 agonist in vivo; (2) to compare the efficacy of three frequently used spacers (plastic Aerochamber, plastic Volumatic, and metal Nebuchamber).
Methods
PATIENTS
The study was approved by the Medical Ethics Committee of the Zuiderziekenhuis, Rotterdam, Netherlands. From the total patient population of the paediatric outpatients clinic of the Zuiderziekenhuis, patients were selected who fulfilled the following criteria: diagnosis of asthma; between 4 and 8 years of age; ability to inhale via a pMDI and spacer; and ability to perform technically acceptable and reproducible peak expiratory flow (PEF) manoeuvres.
Parents of children fulfilling these criteria received written information about the background, the purpose, and the practical aspects of the study. Some days later, parents were phoned and were asked for their participation. Parents who allowed their child to participate signed written informed consent.
STUDY DESIGN
All short acting bronchodilators were stopped at least eight hours before the study (long acting bronchodilators at least 72 hours before the study). Anti-inflammatory medication (corticosteroids, cromoglycate) was maintained unchanged during the study. All measurements were performed by one investigator (ED). Children were randomly allocated to one of three groups: Aerochamber, Volumatic, and Nebuchamber. Within the Aerochamber and Volumatic group, a crossover comparison was made between electrostatic and non-electrostatic spacers. Half of the children started with an electrostatic spacer and crossed over to a non-electrostatic one, and vice versa. The change in PEF after salbutamol was the primary outcome measure. Peak flow measurements were performed by means of the “Personal Best” PEF meter.12 Three technically satisfactory maximal forced expiratory manoeuvres were performed which did not differ by more than 5%.13 The highest PEF was used for analysis.13 Height and weight were measured and used for calculation of the individual predicted PEF values.14 ,15One puff of 100 μg salbutamol (Ventolin pMDI with hydrofluoroalkane propellant, Glaxo Wellcome, Zeist, Netherlands) was then inhaled via the spacer. Time between actuation of the pMDI and inhalation was kept as short as possible (less than three seconds).7 ,9 ,11Children first practised correct inhalation technique from the spacer (at least six deep slow breaths for a period of at least 45 seconds). All children could inhale without a facemask. Fifteen minutes after inhalation of salbutamol, PEF measurements were repeated in the same way. Another 300 μg of salbutamol was then given as separate puffs of 100 μg salbutamol, each followed by inhalation from the spacer. After 15 minutes, PEF measurements were performed again.
One day later, the children returned at the same time of day for a repetition of the experiment. Children who used an electrostatic spacer the first day, crossed over to a non-electrostatic spacer the second day, and vice versa. Children from the Nebuchamber group also returned for a second measurement. In these children, bronchodilating responses on the first and second day were averaged and used for calculations. The salbutamol pMDI perfectly fitted the Nebuchamber. Parents/children and investigator completed a questionnaire on the side effects of medication (tremor, flush, headache, perspiration), and experience with spacer(s) in the past.
SPACERS
Three types of spacers were used: the Aerochamber (Boehringer Ingelheim, Alkmaar, Netherlands), the Volumatic (Glaxo Wellcome, Zeist, Netherlands), and the metal Nebuchamber (Astra Zeneca, Zoetermeer, Netherlands). Plastic spacers were made non-electrostatic by cleaning with an ionic detergent (Dreft, Procter and Gamble, Rotterdam, Netherlands; concentration 1/5000; content: 15–30% anionic, 5–15% non-ionic, and <5% amphoteric material) and drip drying in the air for 24 hours.16 Plastic spacers were made electrostatic by washing with water and drip drying for 24 hours.16 ESC on the inner surface of the Aerochamber, Volumatic, and Nebuchamber was measured by a custom made electrometer (Central Instrumentation Department, Erasmus University Rotterdam, Netherlands). The electrometer consisted of a metal probe of length of 12 cm connected to a high impedance volt meter. To measure ESC, the probe was positioned exactly in the middle of one half of the spacer. Any ESC on the inner surface of the spacer induced a charge on the probe, which was shown on the display of the electrometer. The two parts of the Volumatic and Nebuchamber were measured separately. ESC of the spacer was the sum of the two parts. In a validation study, ESC on electrostatic and non-electrostatic spacers was measured in a random sample of 10 spacers of each type to evaluate the reliability of the standardised washing technique.
OUTCOME MEASURES
The change in PEF 15 and 30 minutes after administration of 100 and 400 μg salbutamol was the primary end point. We calculated absolute change in PEF as well as percentage improvement from initial (prebronchodilator) value, as the first mentioned expression method may give a better reproducibility of bronchodilating responses.17 We present only data on the percentage changes because analysis of both expression methods led to the same conclusions. The children scored their degree of satisfaction with the used spacer from 0 to 10. We noted possible side effects (palpitations, headache, hyperactive behaviour, flush, tremor).
STATISTICS
The influence of ESC within the Aerochamber or Volumatic groups was analysed within patients using Student'st test for paired data. The absence of significant period or carry over effects was first checked by procedures for crossover studies.18 Comparison of the various spacers was done using analysis of variance (ANOVA). For the comparison of categorical data, the χ2 test was used. A p value of 0.05 (two sided) was considered the limit of significance. For the parallel group comparison, 22 patients for each spacer group were necessary to detect a clinically relevant difference of 5% in PEF with 95% reliability, assuming a power (1 − beta) of 90% and a coefficient of variation in PEF of 5%. With the sizes of the studied groups, differences within, as well as between groups should become evident (power: 80%) if the differences are about 0.7 standard deviations.
Results
A total of 162 children with asthma from the outpatients clinic were asked to participate in the trial. Parents of 90 children gave written informed consent. One child was excluded from the study because he was not able to perform PEF measurements correctly. Therefore, we collected data on 89 children. Reasons for non-participation were mainly not medical (n = 68; no time, no interest, moving home, sickness in the family). Four patients refused for medical reasons (Bordetella infection in one, not able to inhale or to perform PEF manoeuvres in two, too mild asthma in one). Table 1 presents patient characteristics. No clinically and statistically significant difference existed between the groups.
Patient characteristics of the study group
VALIDATION OF ANTISTATIC TREATMENT
ESC on plastic spacers ranged from 0 to 2.5 V for both the non-electrostatic Aerochamber and Volumatic. For the electrostatic Aerochamber, charge ranged from 50 to 100 V. ESC on the electrostatic Volumatic was 12.5 to 40 V. As expected, no charge was present on the metal Nebuchamber.
EFFECT OF ELECTROSTATIC CHARGE (WITHIN PATIENT COMPARISON)
A high correlation was found between baseline PEF values at the first and second visit for both the Aerochamber group and Volumatic group (both r > 0.97, p < 0.001). Mean baseline values at both visits were not significantly different (Aerochamber group: p = 0.46, Volumatic group: p = 0.37). No effect of ESC was found on the bronchodilating response to salbutamol in the Aerochamber group. For 100 μg salbutamol, the percentage change in PEF was 13.9 (SEM 1.8)% for the non-electrostatic spacers and 14.0 (1.8)% for the electrostatic spacers (95% confidence interval (CI) −3.8% to +3.7%, p = 0.984). For 400 μg salbutamol, the change in PEF of 16.7 (2.5)% in the non-electrostatic Aerochamber was not different from the bronchodilating response of 15.7 (2.0)% in the electrostatic Aerochamber (95% CI −3.7% to +5.7%, p = 0.668). No effect of ESC was found on the bronchodilating response to salbutamol in the Volumatic group. The change in PEF after 100 μg salbutamol was 15.8 (SEM 2.9)% for the non-electrostatic group and 12.5 (2.3)% for the electrostatic Volumatic (95% CI −1.5% to +8.1%, p = 0.165). For 400 μg salbutamol, the change in PEF of 21.8 (3.2)% in the non-electrostatic Volumatic was not different from the bronchodilating response of 19.1 (2.7)% in the electrostatic Volumatic group (95% CI −2.2% to +7.5%, p = 0.266). Combining the data from the Aerochamber and Volumatic groups, the mean difference (non-electrostatic minus electrostatic) in the bronchodilating response after 100 μg salbutamol equalled +1.7% (95% CI −1.3% to +4.7%). The same figure after 400 μg salbutamol was +1.9% (95% CI −1.4% to +5.1%).
EFFICACY OF NEBUCHAMBER VERSUS AEROCHAMBER VERSUS VOLUMATIC (BETWEEN PATIENT COMPARISON)
As we found no significant effect of ESC, we calculated average values of the bronchodilating response at both visits in each group in order to make intergroup comparisons. A comparable efficacy was found for the Nebuchamber, Aerochamber, and Volumatic with respect to the change in PEF after salbutamol (fig 1). For 100 μg salbutamol, the change in PEF was 10.5 (SEM 1.7)% in the Nebuchamber group, 14.0 (SEM 1.6)% in the Aerochamber group, and 14.1 (SEM 2.4)% in the Volumatic group (p = 0.329). The mean increase in PEF after 400 μg salbutamol was 16.9 (SEM 2.0)% in the Nebuchamber group, which was not significantly different from the response of 16.2 (SEM 2.0)% in the Aerochamber group and the response of 20.5 (SEM 2.8)% in the Volumatic group (p = 0.369). The comparable efficacy of Nebuchamber, Aerochamber, and Volumatic remained when the non-electrostatic outcomes of the Aerochamber and Volumatic groups were compared with the Nebuchamber.
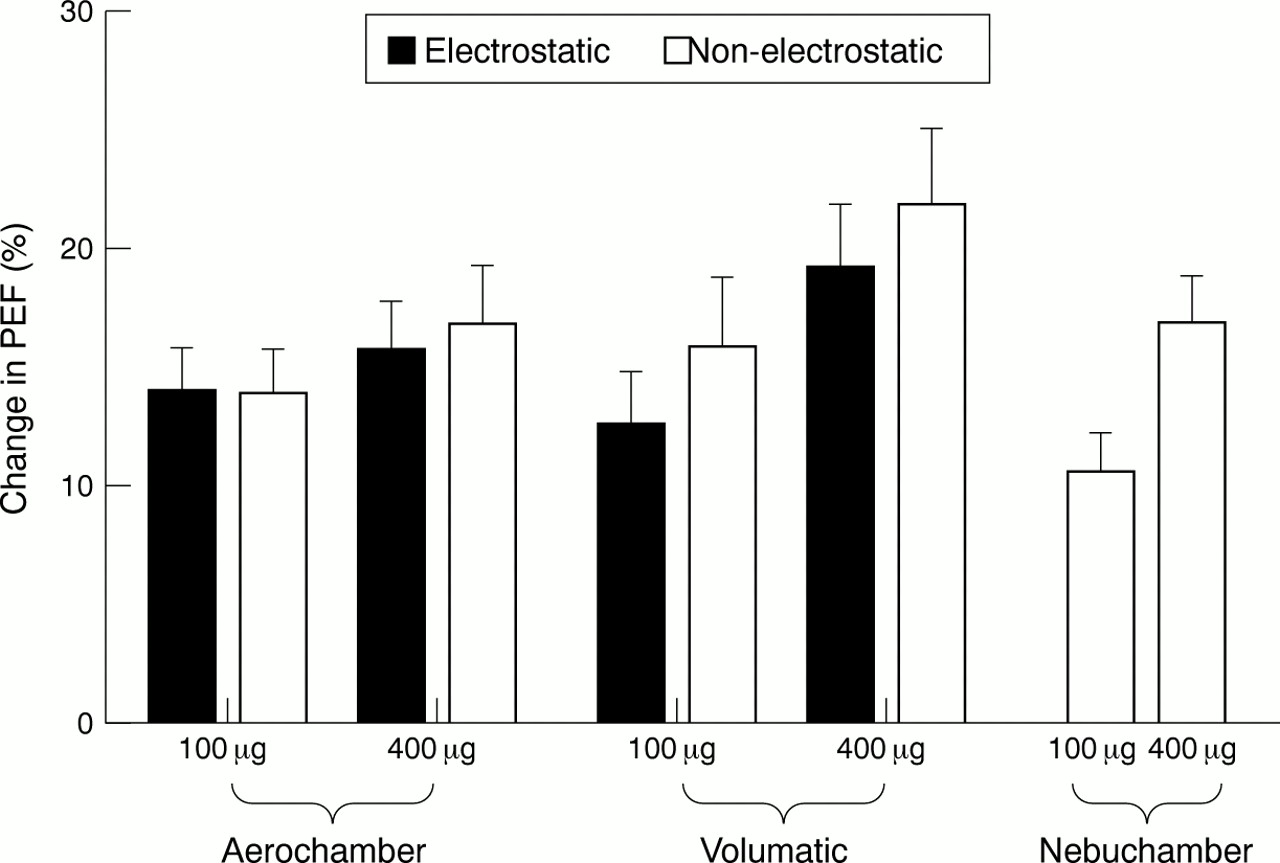
{kind=link}
Relation between spacer type and bronchodilating response to salbutamol; influence of ESC and drug dosage.
As expected, we found a clear relation between the dose of salbutamol and the bronchodilating response (fig 1). The bronchodilating response to 400 μg of salbutamol was significantly greater than the response to 100 μg in the Aerochamber group (p = 0.021), the Volumatic group (p = 0.0001), and the Nebuchamber group (p = 0.0001).
The incidence of side effects to the hydrofluoroalkane pMDI of salbutamol was low, one child with tremor and one with hyperactive behaviour.
Eighty four per cent of children were satisfied with their spacer. This percentage did not differ between the Aerochamber (89%), Volumatic (79%), and Nebuchamber (85%) (p = 0.609).
Discussion
Inhalation therapy using a pMDI with spacer plays a crucial role in the treatment of young asthmatic children and is of great use in the management of patients with cystic fibrosis and BPD.1 ,2 ,19 Several studies in the past five to ten years reported that the efficacy of plastic spacers may be reduced by ESC.5-11 It is not clear from these studies to what extent ESC is a problem for the in vivo efficacy of inhalation medication in children. To clarify this issue, we investigated ESC on plastic spacers in relation to the bronchodilating responses of a β2 agonist in vivo. In 90 asthmatic children, we did not find a negative influence of ESC on clinical efficacy of salbutamol. Bronchodilating response to this drug, inhaled via electrostatic or non-electrostatic spacers, was comparable. This result was not dependent on the dose of salbutamol.
A number of in vitro studies have investigated the relation between antistatic treatment of spacers and the aerodynamic particle size output as assessed by a multistage liquid impinger.7-9 ,11 ,20 O'Callaghan and colleagues found a 144% increase in output of cromoglycate particles <5 μm by lining the Fisonair spacer with an antistatic spray.9 In a comparable study, Wildhaber et al found that treatment with an ionic detergent increased the output of salbutamol particles <6.8 μm from the Babyhaler 1.7-fold and from the plastic Nebuhaler 2.1-fold.7 The amount of budesonide particles <5 μm from an antistatic Nebuhaler was increased 2.3-fold compared with a static Nebuhaler in the study of Barry and O'Callaghan.11 Although these studies showed a clear and reproducible effect of ESC, the results may not be generalisable as passage of an aerosol through an impinger at constant flow does not resemble physiological breathing and normal inhaling techniques. Although one might expect that a larger number of particles <5 μm from reduced static or metal spacers would result in a larger deposition in small airways, the actual deposition was not measured, so firm conclusions cannot be drawn.
In two filter studies by Bisgaard et al, the delivery of budesonide aerosol from different spacers was evaluated in 124 asthmatic children aged 6 months to 6 years6 and 164 children with asthma less than 8 years of age.5 The children breathed through the spacer for 60 seconds. The dose of aerosol released from the spacers was largest for the metal spacer (39% of nominal dose) and decreased to 28% for the Babyhaler and 19% for the Aerochamber.6 In the in vitro part of this study, the half life (t1/2) of the budesonide aerosol appeared to be best for the metal spacer (27 seconds), compared to 21 and 17 seconds for the Babyhaler and Aerochamber respectively, despite antistatic treatment of these plastic spacers by means of priming.6 However, results do not detail lung deposition or clinical response.
This drawback was partially overcome in three scintigraphic studies. Kenyon and colleagues10 investigated the influence of static charge on lung deposition of radiolabelled budesonide in 10 adult asthmatic patients by priming plastic spacers. Priming improved the peripheral lung deposition of the plastic Nebuhaler and Volumatic by 37% and 47% respectively, but had no influence on deposition in the metal Nebuchamber group (as expected). In a recent study,21 the whole lung deposition of salbutamol delivered from a detergent coated Babyhaler and Volumatic in 18 asthmatic children aged 12 to 146 months was much higher than expected. Deposition increased with age from 16.4% to 41.8% but there was no control group using non-detergent coated (or static) spacers, and ESC was not measured. On the basis of these results, our hypothesis was that ESC on plastic spacers diminished the bronchodilator response to salbutamol in asthmatic children. However, we found no such effect. How can we explain the differences between the results of our study and those of others?
It might be that an influence of ESC in our study was masked by the excellent inhaler technique of the children and the dosages of salbutamol used. Children in our study started inhalation immediately after actuation of the pMDI into the spacer and took at least six deep breaths from the spacer for at least 45 seconds. Others have shown that a negative influence of ESC was mainly prominent in combination with a long residence time of aerosol in the spacer.7 ,9 ,11Moreover, a greater number of breaths from the spacer increases the total amount of drug inhaled.22 Although there was a clear dosage effect on the PEF response in this study, it is possible that these dosages were already at the higher part of the dose–response curve. In this way, the effect of ESC might be too small to influence the bronchodilating response. On the other hand, it is difficult to compare our results with others because this is the first clinical study which has investigated the influence of ESC on the clinical efficacy of inhaled bronchodilators, assessed by changes in lung function. Although the PEF is a more variable and more effort dependent variable than, for instance, FEV1, our study had sufficient power to show a possible relevant difference between static and non-static spacers and between different dosages of salbutamol. More studies are needed to establish further the relation between ESC and the clinical response to inhaled medication. As maintenance treatment with inhaled corticosteroids is very important for the long term control of asthma, it would be interesting to investigate whether ESC does influence the efficacy of steroids.
The comparative study between Nebuchamber, Aerochamber, and Volumatic revealed equal efficacy of these devices with respect to the bronchodilating response to salbutamol in this age group. A number of studies compared the clinical efficacy of different spacer systems by investigating the change in lung function after a bronchodilator.23-25 Lee and Evans found a slightly greater bronchodilator response after albuterol for the Inspir-Ease and the Aerosol Bag than for the Aerochamber in 20 stable asthmatic children.23 Salbutamol 100 μg via the Volumatic was superior to terbutaline 250 μg via the Nebuhaler in the study of Chapman and Crompton.25
Two pharmacokinetic studies compared the efficacy of different spacer devices. In the study of Lipworth and Clark, the average plasma concentration following administration of salbutamol 1200 μg (non-CFC, Airomir) between Nebuhaler, Volumatic, and Aerochamber was compared with pMDI alone in 10 healthy adults.26 Lung delivery from the Nebuhaler was 2.1-fold, from the Volumatic 1.5-fold, and from the Aerochamber not significantly different from that of the pMDI alone. In a comparable study of Hindle and Chrystyn, the relative bioavailability to the lung was larger in the Nebuhaler and Bricanyl Spacer groups in comparison with pMDI alone. This was not found for the Volumatic group.27
In the filter study of Wildhaber et al, delivery of salbutamol particles <6.8 μm from a reduced static Aerochamber was comparable with the metal Nebuchamber.7 In 124 asthmatic children, Bisgaard et al found a greater delivery of budesonide from a metal non-electrostatic spacer (39% of the nominal dose) on a filter than from the “primed” Aerochamber.6
Two studies by Barry and O'Callaghan compared delivery of various drugs and formulations in different spacer devices by means of a glass multistage liquid impinger.11 ,20 In comparison with a pMDI alone, the large volume spacers (Volumatic, Fisonair, and plastic Nebuhaler) appeared to increase the delivery of fine particles (<5 μm), whereas the small volume spacers (Aerochamber, Dynahaler) seemed to decrease it. This result held for both salbutamol and sodium cromoglycate but was less evident for budesonide. It is clear from this study that experiments with one spacer device or drug cannot be extrapolated to others.
It is difficult to compare these studies with our investigation because of differences in outcome measures, patients, ages, types, and dosages of drugs. Some studies suggested a greater efficacy of the large volume spacer (Volumatic) than of the small volume spacer (Aerochamber).20 ,26 It is possible that the young asthmatic patients in our study benefited relatively more from a few small breaths from concentrated aerosol in a small spacer than from a large spacer.22 We could not find a difference between the Volumatic and the Aerochamber in this study.
We conclude that all three spacers worked equally well and produced good bronchodilatation in asthmatic children, even using only 100 μg of salbutamol. The clinical efficacy of the spacers was also reflected by the high percentage of our asthmatic children who were satisfied with their spacer (84%). The degree of satisfaction did not differ between the Nebuchamber, Volumatic, and Aerochamber groups. Salbutamol from a hydrofluoroalkane pMDI (Ventolin) was in general well tolerated by our asthmatic patients.
We further conclude that ESC on plastic spacers does not decrease the in vivo efficacy of bronchodilator therapy in asthmatic children. The metal Nebuchamber, plastic Volumatic, and plastic Aerochamber worked equally well.
Acknowledgments
The authors thank Astra Zeneca BV, Boehringer Ingelheim BV, and Glaxo Wellcome BV for free supply of the Nebuchamber, Aerochamber, and Volumatic respectively.