Article Text

Abstract
Background: Children with special needs present a challenge to those involved in their care.
Aims: To determine the role of the acute assessment unit for these children.
Methods: Case notes and other records were reviewed for information on referrals, admissions, readmission within 7 and 28 days, length of stay, and management of 86 children registered for special needs. The study covered five years between January 1997 and December 2001.
Results: Of the 86 children, 48 (58%) were boys; 62 children had cerebral palsy and 52 learning disability. There were 914 episodes, with 44% of these being self referrals and 35% from general practitioners; 35.5% of the episodes were managed in the assessment unit. The average length of stay in hospital was 5 days, ranging from <24 hours to 63 days; 37.5% of those admitted to the ward stayed for less than 24 hours. Respiratory tract infections and seizures were the main reasons for referral and admission.
Conclusion: Children with special needs tend to have a predictable pattern of conditions requiring inpatient care. One third of the inpatients episodes did not need a prolonged stay in hospital. This latter group of children could be managed at home with support of community nurses. Integrated care pathways need to be developed to minimise disruption to their lives. Appropriate resources should be made available to achieve these goals.
- special needs
- referrals
- admission
- length of stay
- care pathways
- A&E, accident and emergency
- LOS, length of stay
- LRTI, lower respiratory tract infection
- URTI, upper respiratory tract infection
- VP, ventricular-peritoneal
Statistics from Altmetric.com
- A&E, accident and emergency
- LOS, length of stay
- LRTI, lower respiratory tract infection
- URTI, upper respiratory tract infection
- VP, ventricular-peritoneal
The term “special needs children” is a classification for describing young people (children and adolescents) who are experiencing serious and persistent physical, psychological, and/or social problems.1 It has been shown that the majority of those with cerebral palsy attain adulthood, but this is influenced by many factors.2–5
Children with special needs present a unique challenge to those involved in their care. As survival rate in these children increases there is a corresponding increase in the morbidity rate. This fact coupled with the increasing demands being made on all inpatient paediatric services makes the provision of acute health care for these children an increasingly relevant area of research.6,7 The reconfiguration of services and the need for integrated care pathways needs to address the various clinical scenarios for different individuals to ensure that their needs are met.5 Previous work has shown that these children are staying in hospital longer than children without special needs. There is also evidence that this group of children constitutes an increasing percentage of hospital admissions.3,8
Integrated care pathways will enable managed networks to deliver a service for them, if problems and their needs are clearly identified. Further evidence is therefore required to design practical guidance for carers and parents as well as professionals.
The aims of this study were to determine the frequency and reasons for referrals of these children. We also wanted to determine the role of the acute assessment unit in the management of a group of children with special needs over a five year period.
Acute assessment unit
The unit was set up in 1994 and is situated adjacent to the inpatient wards. It has its own resuscitation room and a microscope used for urine analysis. There are seven whole time equivalent nurses with no other inpatient duties. They are supported by specialist nurses in epilepsy, life threatening illnesses, diabetes, cystic fibrosis, and asthma. There are another two community nurse posts, but one was vacant for the last year of the study. There are two administrative clerks. The medical staff includes a consultant of the week, a specialist registrar, and a senior house officer. The unit opens between 8 am and 8 30 pm on weekdays and 9 am and 5 pm at weekends. The Child Development Centre (CDC) and the Accident and Emergency (A&E) Departments are based at a different site two miles away. All medical referrals as well as A&E non-trauma patients needing inpatient care are sent to the assessment unit.
All children referred during the opening hours are assessed in the unit. After the assessment, a decision is made whether to send the child home, observe in the unit, investigate, and/or admit to the ward. For children being sent home the decision is based on the medical condition, social circumstances, and the parents’ ability to cope with home management. Support is offered by the epilepsy nurse, community nurse, or the life threatening illness nurse as required.
The unit also has a list of children who are allowed open access. This usually means that the parents can contact the unit directly if there is a delay in accessing the family doctor.
Special needs register
This register was set up for those children who needed an education statement. However, children with significant neurodisability can be registered as soon as the problem is identified. At the time of the study there were 701 children on the register, in a district which has a child population of 75 000. A community paediatrician maintains it. Table 1 shows the various conditions that have lead to their inclusion on the register.
Special needs register list
Carers
In addition to parents, the district provides care for children with severe learning disability at the CDC where many attend several times a week on a regular basis. There are five nurses who help supervise during the day. Two families whose children have tracheostomy have a 24 hour home care service. All children with epilepsy have access to epilepsy specialist nurse service.
PATIENTS AND METHODS
The information was collected retrospectively from the case notes of 86 patients who attended the paediatric acute assessment unit between January 1997 and December 2001. A special needs register, an assessment unit admission register, and patient administration system were used to identify patients with relevant background problems who had attended the assessment unit over the five year period. A CHKS database program was used to review the re-referrals and re-admissions. This program is used for evaluation of clinical indicators.
Inclusion criteria were cerebral palsy, moderate to severe learning needs (mental retardation), severe physical disability, ambulatory disability, and a statement of educational needs.
Ninety children had attended the assessment unit during that period. Four children were excluded from the study because two died early in 1997 and two had moved out of the area. Eighty six children represented 12.3% of all the children on the register, but only 3.06% of all acute episodes. We do not have information on the rest of the 615 children on the register who were not seen in the assessment unit for acute illnesses. They would presumably have seen their GPs as necessary.
Eighty six case notes were reviewed for the following information: source and type of referral, age, admissions, presenting complaint, discharge diagnosis, and length of stay.
The data are presented as episodes per patient, referral, length of stay, and simple percentage calculation. Comparative data on 29 873 emergency referrals during the same period are also shown.
RESULTS
A total of 722 (79%) of the 914 episodes were emergencies; 48 (58%) of the 86 cases reviewed were boys. Table 2 shows the list of the underlying diagnoses; 72.1% of children had a background diagnosis of cerebral palsy, five (5.6%) children had muscular dystrophy, 13 of the 86 children had a gastrostomy, 11 had a ventricular peritoneal (VP) shunt, three had both a gastrostomy and a VP shunt, two had a tracheostomy, and two had a portage.
Underlying diagnosis
Age profile
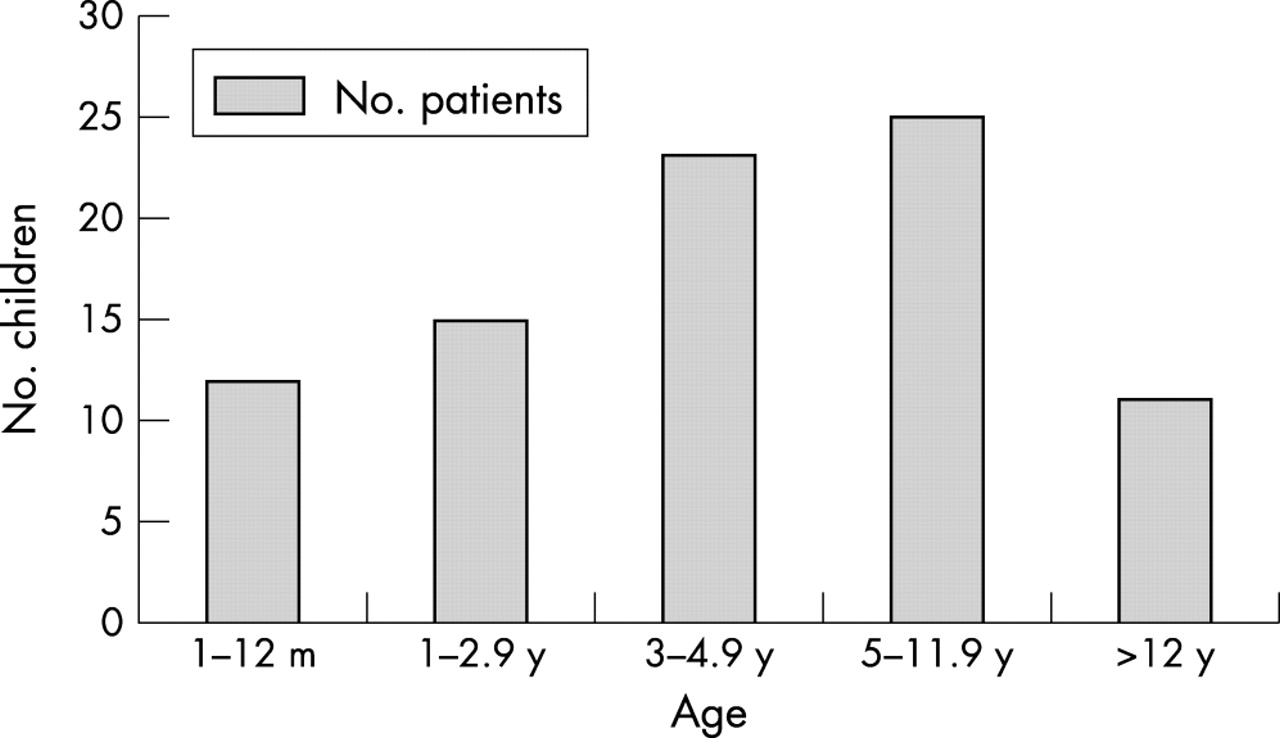
Figure 1 shows the age profile; there were no patients aged less than 1 month. The median age was 4.2 years and the mean age was 5.5 years of age. The oldest patient was 20 years old.
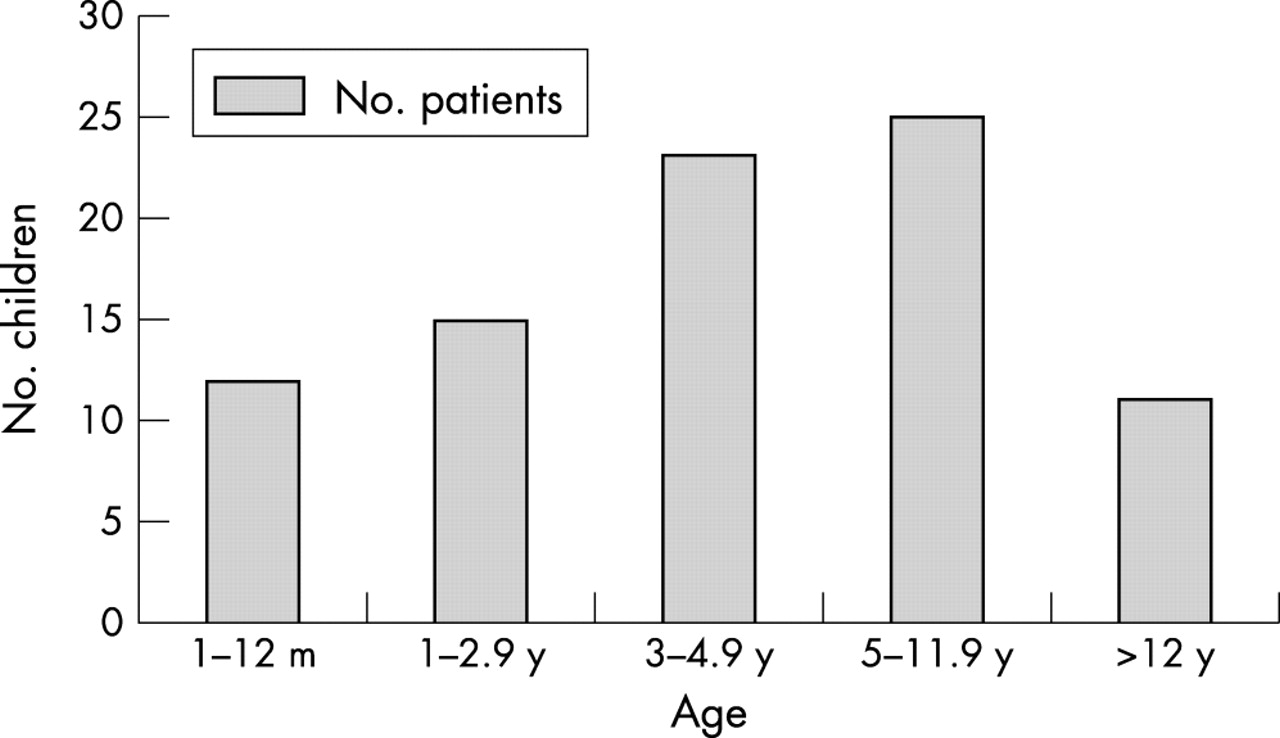
Age distribution of patients.
Referral patterns
A total of 164 (21%) of the episodes were elective in consultation between a paediatrician specialising in neurodisability, and either an orthopaedic surgeon, a neurosurgeon, or an ENT surgeon. These referrals were subsequently admitted to the inpatient facility but are not included in the calculation for length of stay for emergency referrals. The majority of the acute episodes were either general practitioner or self referrals (table 3). A small number of the emergency referrals were admitted via the accident and emergency department. Four patients who came by emergency ambulance were referred with a diagnosis of status epilepticus.
A comparison of referral sources
The number of episodes per child to the assessment unit for emergency consultation was 1–57 per child with a median and mean of 4.5 and 10.2 episodes respectively. There were individual variations, with more frequent referrals in those children with very severe neurological disability. This group of 86 children generated 914 episodes over five years compared with 28 959 episodes from the remaining 74 914 children. The episode rate over the five year period was 10 627 per 1000 versus 368 per 1000 for special needs and the remaining population respectively.
Presenting problems
Of the emergency referrals and admissions (see table 4) respiratory tract infections and seizures were the most common presenting symptom. Upper respiratory tract infection (URTI) and gastro-oesophageal reflux were the major contributing factors to lower respiratory tract infections (LRTI). The children with seizures were known to have seizures and either had status epilepticus or an increase in seizure frequency. However, there were those who were experiencing fits for the first time.
Reasons for referrals to the assessment unit and admission
Admission and length of stay (LOS)
A total of 256 (35.5%) of the 914 episodes were dealt with in the assessment unit (fig 2). The mean period of observation in the assessment unit was 2 hours with a range of 45 minutes to 4 hours.
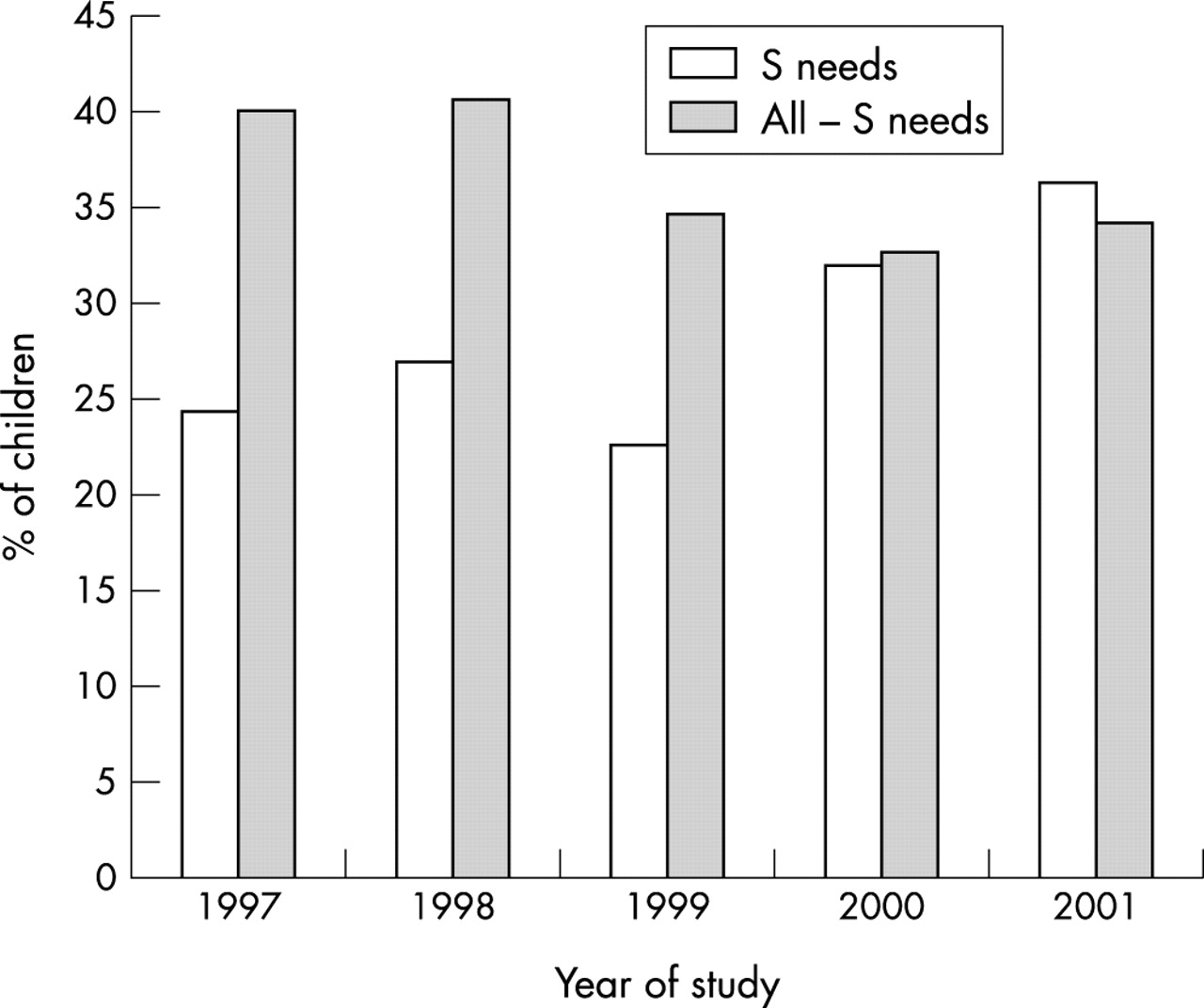
Percentage discharges per year from the assessment unit.
In comparison we have discharged between 32.8% and 40.7% of children without special needs over the same period. The mean and median number of episodes handled in the assessment unit and child going home were 4.5 and 3 respectively. The clinical problems are shown in table 4. Of those children who were admitted for inpatient care, the LOS was variable with 37.5% having “short admissions” (less than 24 hours) and a significant proportion staying in hospital for more than 24 hours (fig 3). The longest admission was for 63 days in a child with LRTI and a background diagnosis of spastic cerebral palsy. The average length of stay was 5.4 days compared to 0.9 days for other children admitted to our unit. There was a very high readmission rate, 17.6% and 26.7% being re-referred within 7 and 28 days respectively. The corresponding values are 3% and 6% for children without special needs aged 12 months and above.

{kind=link}
{kind=link}
{kind=link}
Percentage of children staying in hospital over 24 hours.
DISCUSSION
This study provides information about the referral patterns, presenting problems, length of stay, and admission rates of children with special needs via the paediatric assessment unit.
A small group of children with severe neurological disability and learning difficulties use the emergency services very frequently. Although the cases considered (3.06%) represent only a tiny proportion of referrals to the assessment unit over the same period, the data provide important background information about the utilisation of the unit by this group of patients. Many referrals were for acute illnesses, but other episodes were as a result of complications to procedures performed on these children.
Feeding was another problem, and gastro-oesophageal reflux complicated much of the children’s care, leading to recurrent LRTI. It is accepted that readmission to hospital is more common in children with special needs,7–9 but further work is required either to reduce the readmission or to provide alternative care that is convenient and safe.
Our findings also show that many parents seek advice appropriately, either through the GP or directly to the acute assessment unit. Parents are managing to look after their children at home, but there is continued disruption to their lives due to acute illness. Some of the illnesses do not require inpatient care. It is important to recognise that when parents seek help, that is not necessarily an admission request. It is a request to evaluate the problem and reassure them regarding issues such as temperature control, the fear of death while a child has a seizure episode, fluid replacement, and whether the child needs an antibiotic.
In some of these situations there is a need for observations before parents can be reassured. Alternatives have been suggested but should not be considered a cheap option.10 Hospital at home care can be achievable with appropriate resources.
There is a paucity of information on use of the acute services by children with special needs. However, comparison with recent data on paediatric admissions as a whole reveals interesting differences.11,12
These studies have looked at the age profiles and appropriateness for admission which show a pattern of emergency admission similar to that in our hospital. The age profile for children with special needs is slightly different in this study. Some of the differences may be explained by the service provided by the neonatal community nurse team that continues to supervise the care of some of these children up to 1 year of age. Children with special needs are also more dependent on their parents and it sometimes takes weeks and months to establish the underlying diagnosis.
The number of children referred by A&E is low in this study. This can be explained by the open access facility provided to the parents as all medical referrals go through the assessment unit.
Thirty five per cent of the acute admissions in this study were referred to the acute assessment unit by general practitioners. There are no figures available on those patients seen by the GP, who are not referred to hospital. The high referral rate may reflect an increasing demand from GPs for admission, which provides an acceptable and welcome solution to acute illness in children.5 Armon and colleagues13 have also reported a high referral rate and a high admission rate following referral from GPs. These findings suggest appropriateness of use of services, but in this cohort there is also a degree of clinical selection due to the nature and degree of disability. Perhaps more relevant in this cohort is the fact that a number of factors influence admission to hospital, and the GP may have insight into these factors and the decision to refer may be influenced. These factors include cerebral palsy, especially spastic quadriplegia associated with mental retardation, epilepsy, ambulatory disability, and social circumstances.
Respiratory problems were the commonest presenting complaints. The finding that “breathing difficulties” is one of the most common presenting complaints is in line with recent literature.2,5,6 In contrast however, is the large proportion of children presenting with seizure related problems. This is not surprising given the high prevalence of epilepsy in the children with cerebral palsy. The time of admission may also have affected the results since all patients here were admitted through the assessment unit (8 am–8 30 pm), but other studies have shown an increase in rate of admission with respiratory disease overnight.5,7,9,13
Sixty per cent of the patients referred to the assessment unit as an emergency were admitted to hospital. It may be argued that those children who had a “short admission” may be better cared for in the community if appropriate resources were available. Children with severe neurodisability, learning difficulties, and dependent technology are more likely to be referred. The social circumstances and parents’ perception are important when considering children with special needs and the impact this may have on admission should not be underestimated.14 This was clearly illustrated by parents whose children were referred because of seizures.
Parents whose children had presented with seizures belonged to one of the following categories. There were those parents whose children had seizures before and were already on treatment: parents wished to know whether this was another new problem or meningitis; they also wished to know whether the seizure was going to make the child’s condition worse. In other children the seizure was associated with a raised temperature, most commonly due to an upper respiratory tract infection. In others, it was the first seizure and therefore parents were duly concerned. The needs of the three groups of parents were different but also predictable. Guidelines for seizure management (either febrile or non-febrile) can be very helpful for parents and staff.15 The findings of this study are similar those of Scribano and colleagues,16 who found that observation in an assessment unit can be helpful in management of these children. A total of 18.8% of those who presented with seizures in the emergency room were admitted. The period of observation however, was longer (15 hours) than what is normally recommended in our department.
Most of the observations were done over four hours in the assessment unit; they were reassured and discharged. Thirty seven per cent of the inpatient episodes were discharged within 24 hours. In view of the fact that no other treatment was given apart from managing the fever, it is speculated that this care can be provided at home using either the epilepsy nurse or a general community nurse.10 Perhaps a more prolonged period of observation may decrease the number of children admitted.
“Open access” is a principle normally offered to parents of children with special needs. It has the advantage that those children can be seen when parents feel they need to see the child’s paediatrician. The disadvantage is that the general practitioner may be bypassed as happened in 44% of the episodes. The GP therefore will not have enough information on the individual child; this in turn reduces the experience of the GP in managing this special group of children. As a consequence many children end up in the assessment unit.
We believe that the primary care teams have a considerable role to play, but do require support as do the parents. Some parents need respite care to give them a break, but the acute ward is not the best place for special needs children. The social services department working with the GP can be assisted by the special needs team.6,17
We are currently investigating the care pathways involving a paediatrician, physiotherapy, occupational therapy, learning disability, critical care, pharmacy, child development centre, dietician, education, social services, community nurses, GPs, and the assessment unit in the management of special needs children.
The ideal would be a parent contacting a member of the team or NHS Direct and deciding who would be the best person to see the child depending on the nature of the problem. This also requires guidelines for management of seizures, fever, and the other common problems these children face.
The community nurse and dietician can provide education on management of gastrostomy in the home. Evaluation of these needs has to be continuous. Prolonged stay in hospital is not just inconvenient for all; it is also very expensive.
A disadvantage of the study is that it only involved a small number of children and no specific guidelines were followed for this group of patients. It is also a retrospective study. Perhaps future studies should be prospective with planned care pathways.
We believe that the resources required should include a dedicated team of outreach nurses. These should have training in recognition of seriously ill children. They should be able to manage gastrostomy, management of seizures, respiratory disease, intravenous access including portage, in addition to basic nursing skills. Transport for the outreach teams and parents is vital for many to be able to access medical services. Many parents cannot get their children to hospital due to lack of appropriate vehicles. Oxygen supplies are required for some but not all children, and in a two of our cases, tracheostomy care is required. Open access should be available, especially out of normal working hours, as should respite care through social services.
Summary
The acute assessment unit provides an alternative environment for children with special needs to be assessed, have preliminary investigations performed, and observation before discharge. One third of the children can be sent home directly from the unit. Respiratory tract illness and seizures were the commonest problems seen.
The numbers considered here are small and readmission of children with special needs is an area where further work would be worthwhile.
With regard to admission of children with special needs, the importance of factors other than the presenting complaint is important; perhaps it would be useful to have some form of data accessible to the assessment unit with information about these patients. Parent held records or electronic records are very relevant to this population. This would ensure a more informed decision to be made regarding their admission.
REFERENCES
Linked Articles
- Atoms