Article Text

Abstract
Introduction: Hyperoxia and variable oxygenation are associated with morbidity in preterm infants. The optimal range of oxygen tensions is not known. This study aimed to determine whether care based on transcutaneous oxygen tension (TcPo2) or saturation (Spo2) monitoring is associated with less time spent with high oxygen tension and less variability of oxygenation.
Methods: Spo2 and TcPo2 were measured simultaneously during two 3-h study periods allocated in random order. During one period supplemental oxygen was adjusted according to TcPo2 (target range 6.0–9.0 kPa) and during the other according to Spo2 (target range 86–94%). During each period, readings from the second monitor were not displayed. Both TcPo2 and Spo2 were downloaded every second. For each period the mean level and the variability (standard deviation) of Spo2 and TcPo2 and the percentage of time spent above and below target range were calculated and compared.
Results: 19 infants, 13 ventilated and 6 on continuous positive airway pressure, were studied at mean corrected gestational age of 27.2 weeks and mean postnatal age of 6.8 days. Their mean fraction of inspired oxygen at the start of the study was 0.34. Care based on Spo2 monitoring was associated with more time spent with high oxygen tension (median increase 2.62%, p = 0.01), more time with low oxygen tension (median increase 17.41%, p = 0.01), more variability in oxygen tension (median increase 0.28 kPa, p = 0.02) and more variability in oxygen saturation (median increase 0.82%, p = 0.01) than care based on TcPo2 monitoring.
Conclusion: Within the target ranges studied Spo2 monitoring was associated with significantly more variable oxygenation than TcPo2 monitoring.
Statistics from Altmetric.com
Hyperoxia and variability of oxygenation have been linked with increased risk of morbidity in preterm infants.1–5 Oxygen saturation (Spo2) and transcutaneous oxygen tension (TcPo2) monitors are used to monitor oxygen levels in preterm infants. Oxygen therapy is usually adjusted with the aim of keeping the infant’s oxygenation within a target range. Specific target ranges vary from unit to unit because there remains uncertainty over the optimal levels.6 7 Randomised trials are in progress, examining different target ranges. Although both types of monitoring device are used, oxygen saturation and oxygen tension are not linearly related to one another. Neither monitoring method is clearly superior in terms of minimising adverse outcome but comparative studies have not been done.
Saturation monitors are non-invasive, easy to use and do not require calibration or cause heating of the skin. They have a relatively high rate of false alarms,8–10 often caused by poor signal resulting from motion. Because of the shape of the haemoglobin-oxygen dissociation curve small changes in oxygen saturation above 95% can mask large increases in oxygen tension so that saturation monitoring may not be reliable in preventing hyperoxia.8 9 11–13 Transcutaneous monitors require calibration and this can lead to periods of time when no oxygen level is being measured. They are sometimes inaccurate.8 14–16 They need to be re-sited regularly to avoid skin damage from heating and can cause skin burns if left on too long. These issues make them more cumbersome and deter some from using them, particularly in more immature infants. The relative convenience of using saturation monitors may be one reason why saturation monitoring has become the predominant method of monitoring oxygenation in the USA and in the UK, and why more recent studies have focused on saturation monitoring.17 18
We aimed to determine whether infants are exposed to more cumulative hyperoxia or hypoxia or to more variable oxygen tension when oxygen therapy is controlled on the basis of transcutaneous Po2 monitoring or oxygen saturation monitoring.
METHODS
We conducted the study at the neonatal unit of the Simpson Centre for Reproductive Health, Edinburgh, between February 2004 and January 2005. Preterm infants who were more than 24 h old, had an arterial line in situ and were receiving supplemental oxygen, were eligible for inclusion in the study if they were considered unlikely to require a major handling procedure such as intubation during the next 6 h. Infants with known duct-dependent congenital heart disease were excluded. Written informed parental consent was obtained in all cases and the study was approved by an ethics advisory committee.
Each infant was monitored simultaneously with an Spo2 monitor and a TcPo2 monitor. Data from both monitors were downloaded continuously in real time to a cot-side PC for later analysis. The sites of attachment of these monitors were left up to the nursing staff and not standardised among infants as we wished to study the real-life implementation of these technologies and this is often limited by the presence of lines and dressings. Functional oxygen saturation was measured using a Siemens Infinity SC 7000 multiparameter patient monitor (Siemens Medical Systems, Inc, Danvers MA). This monitor uses Siemens’ Oxisure pulse oximetry technology and Nellcor Oximax (Nellcor Puritan Bennett, CA, USA) saturation probes and incorporates ECG to reduce motion artefact. The normal averaging mode for this monitor was used in all cases. This reflects 90% of a Spo2 change within 30 s. The same multiparameter monitor measured transcutaneous Po2 using a Radiometer sensor (Radiometer, Copenhagen, Denmark). Although both methods of monitoring were attached to the patient throughout, at any given time information was only displayed from one monitor. During two consecutive 3-h periods allocated in random order by the opening of a sealed opaque envelope, nursing staff adjusted the oxygen therapy for the first 3 h on the basis of one of the monitors and for the subsequent 3 h on the basis of the other. The transcutaneous oxygen sensor was maintained at a temperature of 43.5°C. The sensor was sited shortly before the start of the first monitoring period and monitoring commenced once the transcutaneous Po2 reading had stabilised. The sensor was re-sited for the second monitoring period. During the TcPo2 monitoring period the nursing staff adjusted the fraction of inspired oxygen (Fio2) to maintain the infant’s TcPo2 within the range 6.0–9.0 kPa. At the start of the study a blood gas sample was obtained from the arterial line of each infant to ensure that there was close agreement between TcPo2 and the arterial oxygen tension (Pao2). Where there was a difference of 1 kPa or more between the two values the TcPo2 alarm limits that were set by the nurse were adjusted by the difference between Pao2 and TcPo2 to the nearest kPa. The downloaded TcPo2 data in these infants were adjusted by the same amount prior to data analysis so that the final data reflected as closely as possible the likely Pao2 of the infants. During the Spo2 monitoring period the nursing staff adjusted the Fio2 to maintain the infant’s Spo2within the range 86–94%. For each of the two periods alarms were only enabled for the monitor under investigation. The infants were cared for by the nursing staff throughout as normal, with no intervention from study personnel.
Downloaded data for TcPo2, Spo2, saturation derived heart rate and ECG derived heart rate were analysed using SPSS version 12.0. Saturation readings where the heart rate measured by the saturation monitor differed from the simultaneous ECG heart rate by more than 10 beats per minute were excluded as artefact from both monitoring periods in order to minimise any motion artefact. For each infant and for each period of monitoring we calculated: the mean TcPo2; percentage of time spent with TcPo2 >9.0 kPa; percentage of time with TcPo2 <6.0 kPa; variability (standard deviation) of TcPo2; mean Spo2; percentage of time with Spo2 >94%; percentage of time with Spo2 <86%; and variability (standard deviation) of Spo2. Transcutaneous Po2 probes required re-siting during two studies, which led to a period where saturation readings were unblinded until transcutaneous Po2 readings were available again. These periods were included in the analysis on an intention-to-treat basis. Because the variables showed non-normally distributed data the two methods of monitoring were compared using non-parametric two related samples test (Wilcoxon test).
RESULTS
A total of 19 infants were enrolled in the study; 11 were conventionally ventilated, 2 received high-frequency oscillatory ventilation and 6 were on nasal continuous positive airway pressure (CPAP). Table 1 gives the characteristics of the infants. None of the infants was paralysed at time of study.
The Spo2 probe site was postductal in 15 infants and preductal in 4 infants. The TcPo2 probe site was postductal in 15 infants and preductal in 4 infants. In 9 infants the first monitoring period was Spo2 and in 10 infants the first period was TcPo2. Saturation data were excluded as artefact for a total of 695 s (0.3%) and 608 s (0.3%) from the TcPo2 and Spo2 monitoring periods, respectively. TcPo2 data were not available from one 3-h monitoring period in an infant during the time when the clinical care was based on Spo2 readings because the TcPo2 monitor was not attached. TcPo2 data were available for a total of 94% of the time when TcPo2 was the monitor displayed to the clinical staff. The transcutaneous Po2 data of four infants was adjusted by the difference between TcPo2 and Pao2 obtained on the arterial blood gas taken at the start of the study. In one case the adjustment was 1 kPa and in three cases the adjustment was 2 kPa.
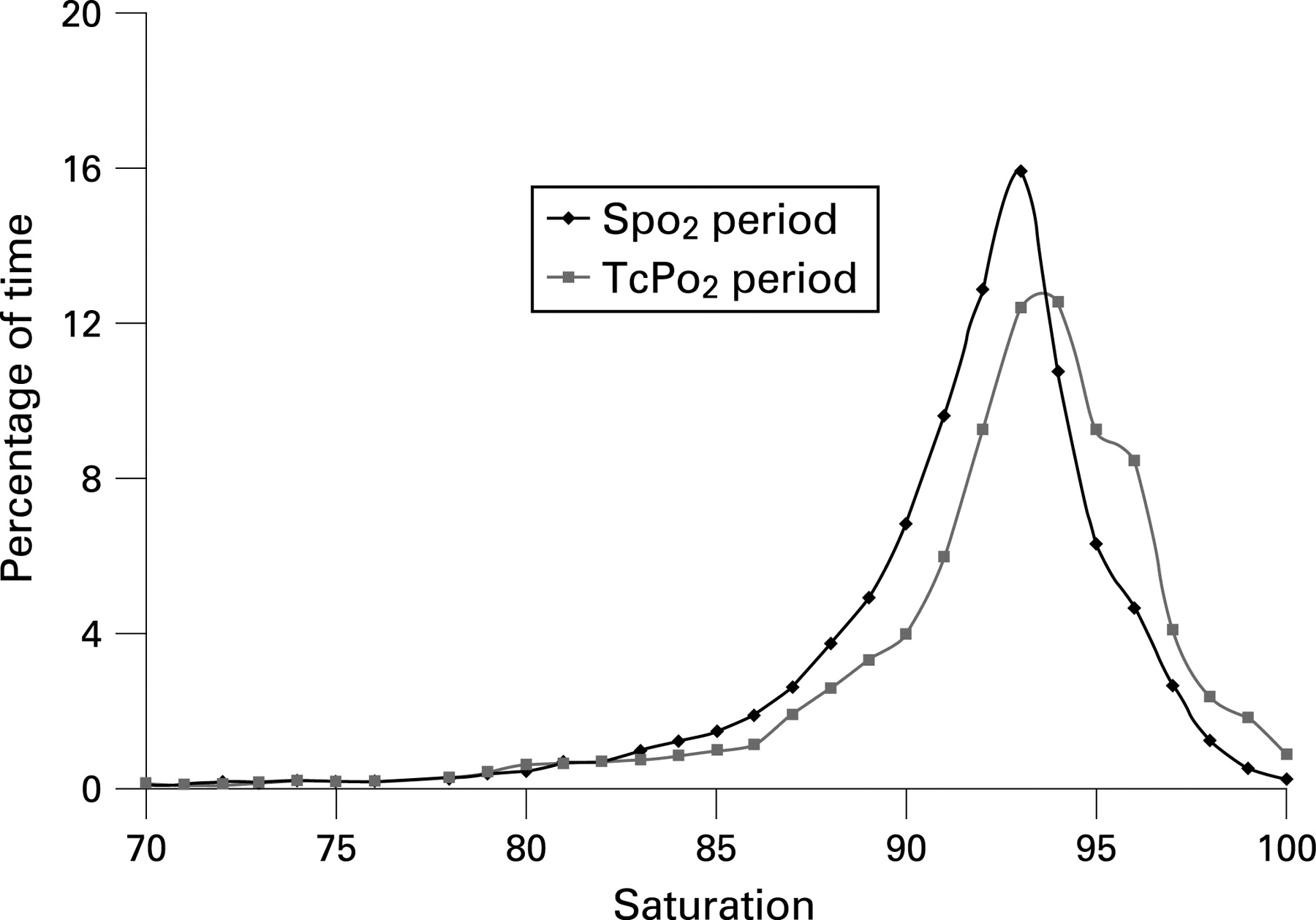
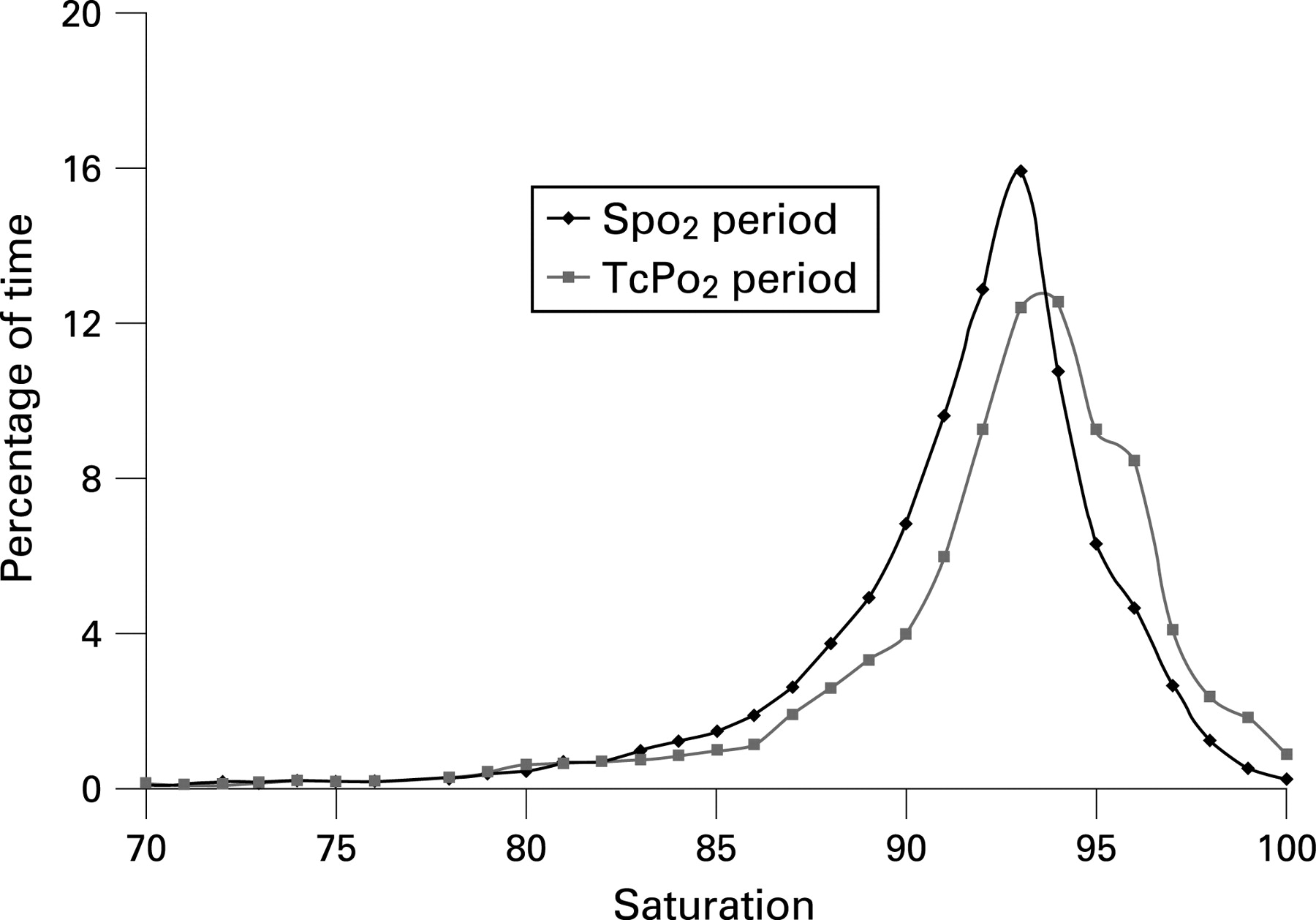
Table 2 summarises the outcome data. Figures 1 and 2 show the cumulative data from all of the infants for the percentage of time spent at different Spo2 and TcPo2, according to the method of monitoring being displayed to the clinical staff.

{kind=link}
{kind=link}
What is already known on this topic
Oxygen saturation (Spo2) monitoring is now used more frequently than transcutaneous oxygen tension (TcPo2) monitoring to guide oxygen therapy in preterm infants in neonatal units.
Neither monitoring method is clearly superior in reducing morbidity and the optimal target ranges are unknown.
What this study adds
Within the target ranges studied, the use of TcPo2 monitoring was associated with less variability in oxygen tension and saturation and less time spent with low and high oxygen tension than the use of Spo2 monitoring.
DISCUSSION
We have shown in a randomised study that within the target ranges specified, controlling oxygen therapy on the basis of transcutaneous Po2 is more effective in limiting high and low transcutaneous oxygen tensions and variability in transcutaneous oxygen tension or saturation than controlling oxygen therapy on the basis of saturation. There was no significant difference in the amount of time spent with low oxygen saturations between the two monitoring methods. When the oxygen treatment was adjusted on the basis of TcPo2 the infants spent more time with high Spo2 than when control was based on Spo2, but this was not statistically significant. Also, a high Spo2 is unlikely to be harmful if it is not associated with increased oxygen tension. Healthy infants can have saturations of 97% or more breathing air.
These results have important implications for practice. There has been a trend recently to reject transcutaneous monitoring in favour of saturation monitoring. Survival of preterm infants has increased but similar improvements in morbidity have not been observed.19–21 No randomised trials have compared the two methods of monitoring. Epidemiological studies and case series suggest that high oxygen tensions or saturations and increased variability of oxygenation may be harmful2 22 and that limiting these exposures may be associated with improved outcomes.4 5 The differences in oxygen tension variability observed in this study were large enough to be relevant to the risk of developing retinopathy of prematurity.2 5 Using only saturation monitoring as the basis for administering oxygen might not be the most effective clinical strategy. There are practical difficulties associated with using transcutaneous monitoring that make saturation monitoring more straightforward but these can generally be overcome in all but the most fragile infants. However, it cannot be assumed that these results, obtained in a research setting, would be replicated fully in everyday use. Randomised trials of different saturation target ranges are under way. It will be important for the interpretation of these trials to gather detailed information about the oxygenation patterns that are achieved.
There are several reasons that the oxygenation of infants may be more stable when they are nursed on the basis of TcPo2 rather than Spo2. Depending on the set averaging time, saturation monitors respond to change more rapidly than transcutaneous monitors. Brief desaturations that trigger the saturation alarms could prompt caregivers to adjust the inspired oxygen, whereas the relatively damped signal obtained with TcPo2 might not show such fluctuation or bring about these adjustments. This may be the main explanation of the differences in stability shown. Movement artefact can lead to loss of signal from saturation monitors, trigger low saturation alarms and cause inappropriate adjustment of the oxygen, with consequent hyperoxia. These issues may be reduced by intensive staff education.4 Saturation monitors incorporating technology that reduces motion artefact, such as Masimo SET may also reduce this problem.23 To minimise bias attributable to motion artefact we excluded saturation data from both monitoring periods where there was a difference in heart rate of more than 10 beats per minute between the ECG and oximeter derived heart rates.
The Spo2 probe and the transcutaneous probe were postductal in 15 of 19 infants. As this was a clinical study, the site of the monitors was left up to the clinical staff. Because few babies have remarkable right-to-left shunts beyond the first few hours after birth, we suspect that most units do not vary their target ranges according to whether their monitors and lines are preductal or postductal. This is unlikely to have had an important effect on the results.
With the limits that we specified, infants spent substantially more time with TcPo2 <6 kPa when oxygen was controlled on the basis of Spo2 than when it was controlled on the basis of TcPo2. The mean TcPo2 and saturation of the infants were also slightly lower, although these differences were not statistically significant. Other studies have shown that episodes of apnoea occur less frequently in infants with higher mean Po2 and sleep architecture and pulmonary hypertension may also be affected.24–31
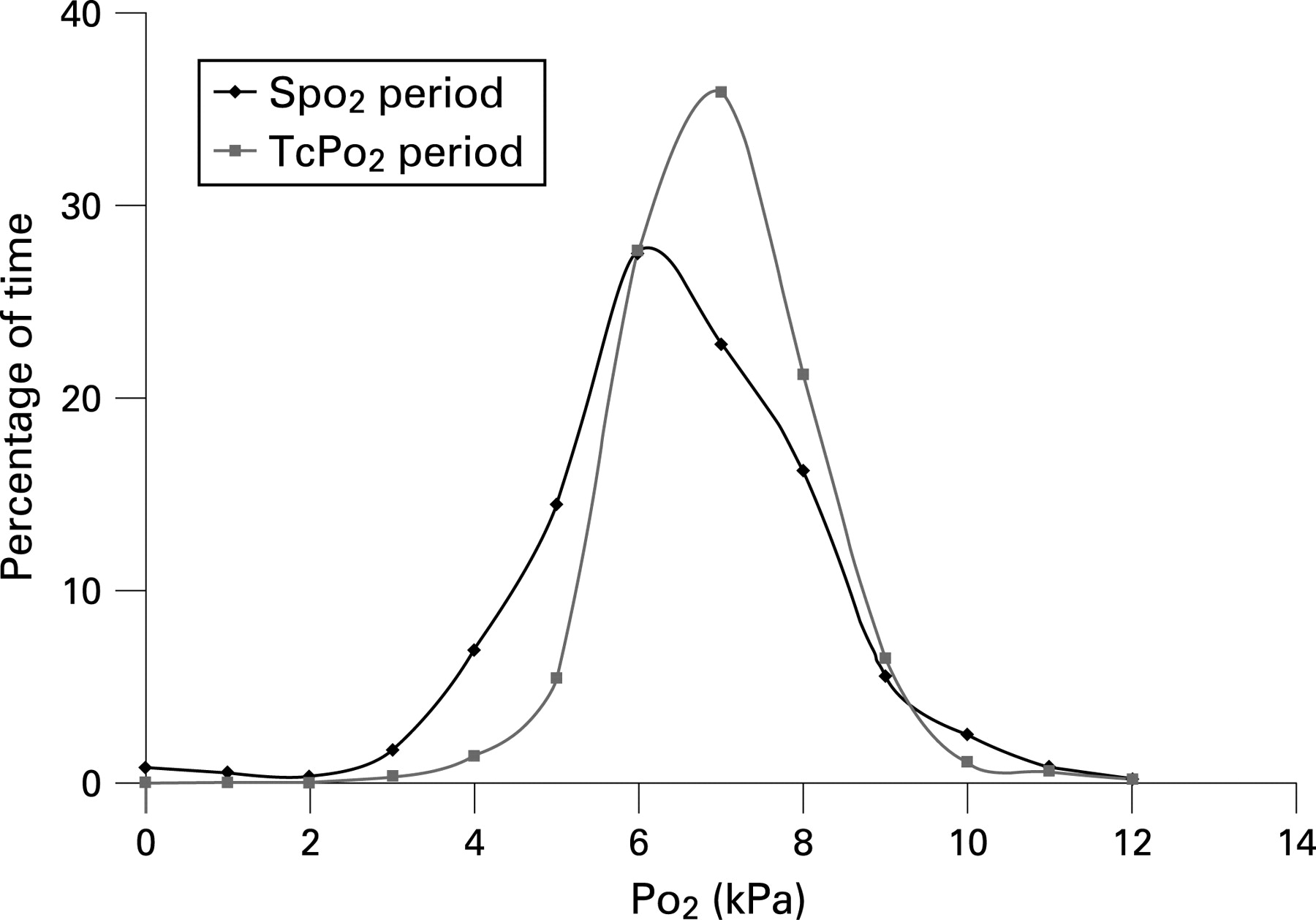
Because saturation and Po2 are not linearly related it would be expected that the two measures would result in different care being delivered. Even though the target ranges overlap, some infants with TcPo2 approaching 9.0 kPa will have saturation greater than 94% and some with saturation of 86% will have TcPo2 less than 6.0 kPa. There is broad consensus that high oxygen tensions should be avoided. Our data suggest that using saturation monitoring with an upper alarm limit of 94% is slightly less effective in this respect than using a TcPo2 limit of 9.0 kPa. However, oxygen tensions greater than 11.0 kPa were seldom observed in either group (fig 2). There is far less agreement over how low oxygen tension or saturation should be allowed to go. Infants in this study spent considerably more time with lower oxygen tension when controlled on the basis of Spo2, but no more time with low saturation. This may not be important, provided that haemoglobin and cardiac output are adequate. Fetal haemoglobin permits satisfactory blood oxygen content and tissue oxygen delivery at lower saturation than 86% and oxygen tensions far lower are observed in the healthy fetus. Preliminary data describing 10-year follow-up of infants cared for with lower saturations do not demonstrate increased adverse outcome.22 32 Deulofeut et al33 observed a reduction in bronchopulmonary dysplasia and retinopathy of prematurity and better mental development index scores at 18 months in infants with birth weight ⩽1250 g when they adopted lower saturation targets. Long-term outcome data from the ongoing randomised trials of different saturation ranges will be capable of showing even modest differences between groups in neurodevelopmental outcome.
We could not download information about the inspired oxygen concentration that the infants were exposed to, as some intensive care equipment do not have the necessary data ports. This should be addressed by manufacturers when developing new equipment.
The target ranges employed in this study simply reflected practice in our unit and are not necessarily the ideal. They are within the range of accepted oxygen targets that have been described. Although some may feel that a lower saturation alarm limit of 86% is quite low, other neonatal units use much lower levels.4 7 22 34 All of the infants in the study were monitored with a single type of oxygen saturation monitor. There is variation in the saturation readings obtained with monitors produced by different manufacturers.8
In conclusion, we have shown in a randomised crossover study that the method of monitoring used to control oxygen therapy in preterm newborn infants has a significant effect on the oxygenation patterns that result. This could have an important effect on the risk of adverse clinical outcome and is worthy of further study.
REFERENCES
Footnotes
Competing interests: None.
Ethics approval: The study was approved by a local ethics advisory committee.
Patient consent: Obtained.
Linked Articles
- Fantoms