Article Text

Abstract
Objective To compare the effect of heated, humidified, high-flow nasal cannula (HHHFNC) and nasal continuous positive airways pressure (NCPAP) on lung function and mechanics in preterm infants with respiratory distress syndrome (RDS) at the same level of retropharyngeal pressure (Prp).
Design Randomised crossover trial.
Setting Neonatal intensive care unit, Ospedale Maggiore Policlinico, Milan, Italy.
Patients 20 preterm infants (gestational age: 31±1 wks) with mild-moderate RDS requiring non-invasive respiratory support within 96 h after birth.
Interventions Infants were exposed to a randomised sequence of NCPAP and HHHFNC at different settings (2, 4 and 6 cmH2O for NCPAP and 2, 4, 6 L/min for HHHFNC) to enable comparison at the same level of Prp.
Main outcome measures Tidal volume by respiratory inductance plethysmography, pleural pressure estimated by oesophageal pressure, and gas exchange were evaluated at each setting and used to compute breathing pattern parameters, lung mechanics and work of breathing (WOB).
Results A poor linear regression between flow and Prp was found during HHHFNC (Prp=0.3+0.7*flow; r2=0.37). Only in 15 out of 20 infants it was possible to compare HHHFNC and NCPAP at a Prp of 2 and 4 cmH2O. No statistically significant differences were found in breathing pattern, gas exchange, lung mechanics and total WOB. Resistive WOB in the upper airways was slightly but significantly higher during HHHFNC (0.65 (0.49;1.09) vs 1.57 (0.85;2.09) cmH2O median (IQR)).
Conclusions Despite differing mechanisms for generating positive airway pressure, when compared at the same Prp, NCPAP and HHHFNC provide similar effects on all the outcomes explored.
- Neonatology
- Respiratory
Statistics from Altmetric.com
What is already known on this topic
-
Heated, humidified, high-flow nasal cannula (HHHFNC) provides effective non-invasive respiratory support to preterm infants in a variety of clinical conditions.
-
Despite differing working mechanisms, both nasal continuous positive airway pressure (NCPAP) and HHHFNC provide a continuous positive airway pressure.
-
Compared to NCPAP, during HHHFNC, the distending pressure for a certain flow rate is not known, highly variable and unpredictable.
What this study adds
-
In infants with respiratory distress syndrome (RDS), the application of either NCPAP or HHHFNC resulted in equivalent lung function and work of breathing when they applied similar distending pressures.
-
The distending pressure developed in HHHFNC fluctuates within the breathing cycle, providing an increased load to the patient, however, this does not appear of a clinically relevant magnitude.
Introduction
Compared to nasal continuous positive airway pressure (NCPAP), heated humidified high flow nasal cannula (HHHFNC) offers ease of use, better tolerance and improved feeding and bonding in preterm newborns requiring non-invasive respiratory support.1–6 As a consequence, it is being increasingly used in neonatal intensive care units in a variety of clinical situations,7–12 most recently postextubation or as initial approach to neonatal respiratory distress syndrome (RDS).13
Even though the working mechanisms of HHHFNC are not yet fully understood, the washout of the upper airways (leading to a reduction of the physiological dead space) and the provision of a distending pressure are considered the most relevant.14–18 While the first is specific to HHHFNC, the application of a distending pressure to maintain lung volume recruitment and airway patency is the rationale of using NCPAP. Although during HHHFNC and NCPAP the developed pressure is due to a gas flowing across a resistance, the flow and the resistance involved in the process differ in the two approaches. During NCPAP pressure is generated within the device and is dependent on the flow in the expiratory line, while resistance is provided by the expiratory valve. By contrast, during HHHFNC pressure is developed within the nasal cavity and results from the flow through the cannula in combination with the infant’s breathing, while resistance is determined by the leak between the nares and the cannula.18 Because of this difference in the modality of generating pressure, the pressure developed during HHHFNC cannot be easily monitored1 ,2 and, most importantly, the retropharyngeal pressure (Prp) might present larger within-breath changes associated with the breathing flow.19 To the best of our knowledge, the effects of the differing working mechanisms of NCPAP and HHHFNC on lung mechanics and work of breathing (WOB) have been compared only in a single study in which NCPAP at 6 cmH2O was related with HHHFNC at different flow rates, therefore, the comparison was not performed matching the distending pressure developed by the two techniques.20
In this study, we aimed to identify whether the differing mechanisms of generating Prp in HHHFNC compared to NCPAP affect WOB, breathing pattern, lung mechanics and gas exchange when the same level of continuous Prp is provided in preterm infants with RDS.
Methods
The study was approved by the human ethics committee of the Fondazione IRCCS Ca’ Granda, Ospedale Maggiore Policlinico in Milan, and informed parental consent had been obtained prior to the study.
Study population
Preterm infants between 28+0 and 32+6 weeks gestational age (GA) and postnatal age <96 h receiving either NCPAP or HHHFNC for mild to moderate RDS were studied. According to the institutional guidelines, the criteria to commence NCPAP or HHHFNC were a Silverman score >5 and/or fraction of inspired oxygen (FiO2) >0.3 for target peripheral oxygen saturation (SpO2) of 88–92%. Infants were studied once they were deemed stable by the treating clinical team. Exclusion criteria were intraventricular haemorrhage or major congenital abnormalities.
Experimental protocol and measurements
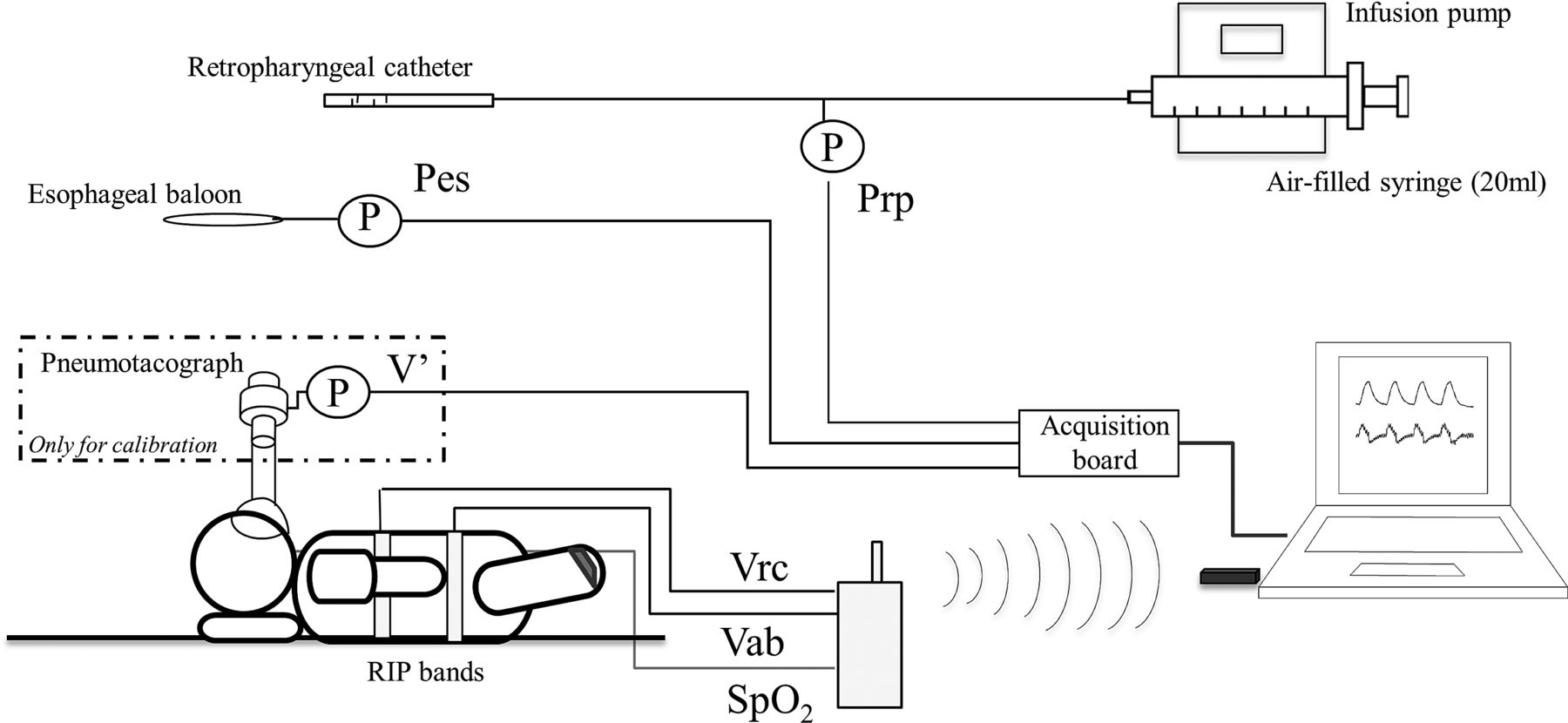
Experimental setup is shown in figure 1. SpO2, heart rate, transcutaneous partial pressure of oxygen (PtcO2) and carbon dioxide (PtcCO2) were continuously measured (IntelliVue X2, Philips, Best, The Netherlands and MicroGas 7650, Linde Medical Sensors, Basel, Switzerland). SpO2, Pes, Prp and lung volume (VL), were continuously recorded at 200 Hz for the last 5 min at each NCPAP/HHHFNC setting. PtcO2 and PtcCO2 were recorded at the end of each protocol step.
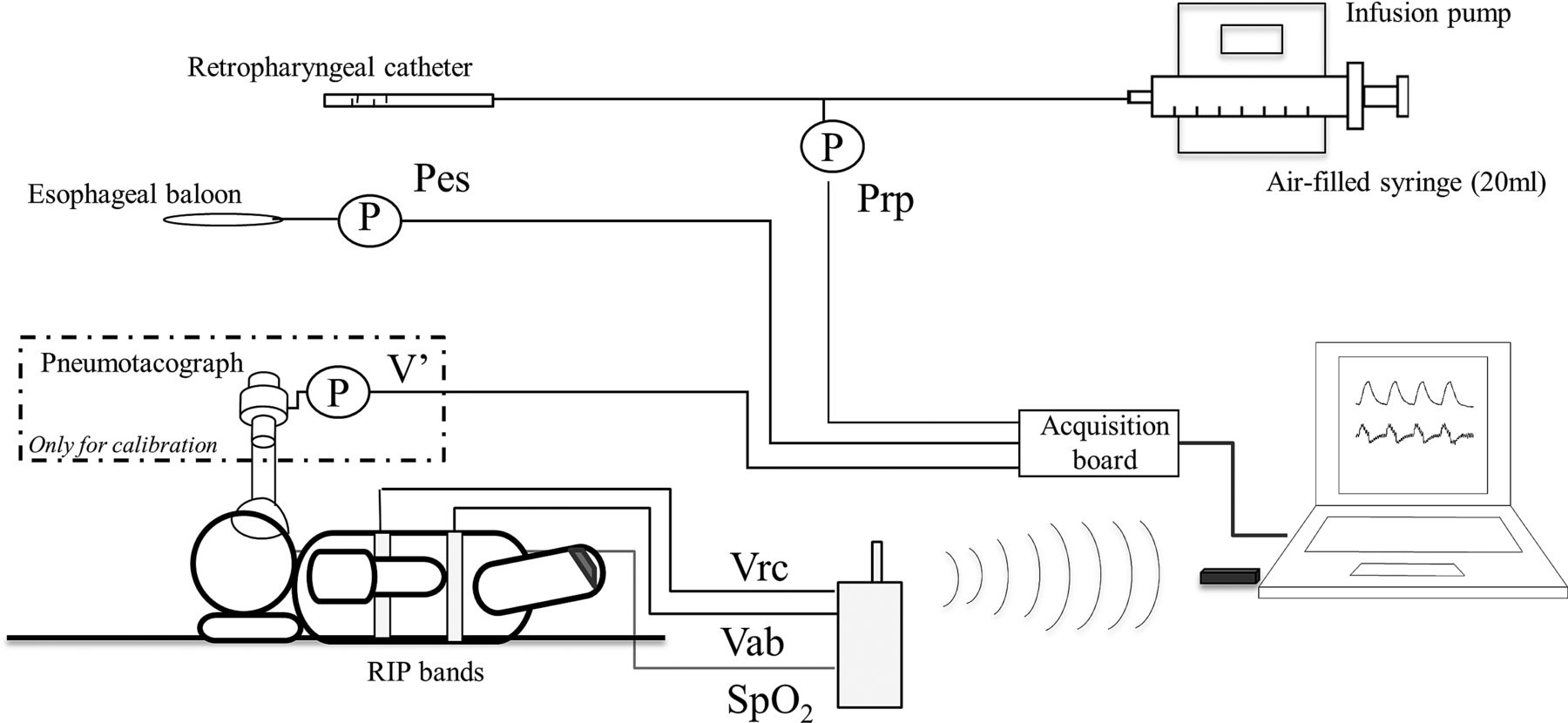
Experimental setup. The pneumotachgraph was only used for calibration.
Tidal changes in VL were computed from the abdominal (AB) and thoracic (RC) displacements measured by respiratory inductance plethysmography (RIP) (Bioradio 150 CleveMed, Cleveland, Ohio, USA). Direct comparison of tidal changes in VL measured by a face-mask pneumotachography (8410A Hans Rudolph, Kansas City, Missouri, USA) over several spontaneous breaths allowed calibration of the RIP.
Intrapleural pressure was estimated by measuring the oesophageal pressure (Pes) through a neonatal oesophageal balloon placed in the lower third of the oesophagus and connected to a pressure transducer (DCXL30D, Honeywell, New Jersey, USA). Correct position of the oesophageal pressure was confirmed by evaluation of the pressure waveform and, when possible, by the occlusion technique.21 ,22
A 6 Fr feeding catheter with four side holes at the distal extremity was inserted in the pharynx and connected to a pressure transducer to measure Prp. To avoid occlusions of the catheter by secretions, a 40 mL/h airflow produced by a microinfuser was applied at the inlet of the catheter.
NCPAP and HHHFNC strategies
The study design was a randomised cross-over trial. Each infant was treated with NCPAP (SiPAP, Viasys, Healthcare, Palm Springs, California, USA) and HHHFNC (Precision Flow-Vapotherm, Stevensville, USA) applied in random order.
During NCPAP, pressures of 2, 4 and 6 cmH2O were applied in a randomised sequence. As it was not feasible to adjust HHHFNC in real time to provide to each newborn similar distending pressures, HHHFNC flow rates of 2, 4 and 6 L/min were applied to all infants, again in a randomised sequence, with the aim of selecting a posteriori, for each infant, the flow rates in which Prp matched the values applied during NCPAP. Each setting during NCPAP and HHHFNC was applied for 15 min.
The size of the nasal prongs for HHHFNC did not exceed 80% of the nares diameter in order to allow adequate air leak. For the purpose of this study, mouth air leaks were avoided by gently closing the mouth during data collection in both HHHFNC and NCPAP.
Data analysis
From the recorded data the following parameters were computed:
Breathing pattern: respiratory rate (RR), tidal volume (VT), minute ventilation (MV), percentage contribution of the rib cage to VT (%RC), Inspiratory Asynchrony Indices (IAI), laboured breathing index (LBI),23 and pressure time product (PTP). IAI was defined as the fraction of the inspiratory time during which the abdomen and the ribcage move in opposite directions.23
Lung mechanics: Lung resistance (RL) and dynamic lung compliance (Cdyn) were estimated by fitting the transpulmonary pressure (PL=Prp−Pes) and VL signals to the equation of motion of the respiratory system by the least-squares method.24
Work of breathing: The WOB and its components were estimated from Pes and lung volume changes measured by RIP as described in Saslow et al.20 The total WOB was divided into its elastic (eWOB), resistive (rWOB), inspiratory (WOBi) and expiratory (WOBe) components. As it is not possible to obtain an accurate passive pressure-volume relationship for the chest wall in spontaneously breathing preterm newborns, the contribution of the chest wall to eWOB has been neglected. Finally, we computed the resistive WOB associated with upper airways (WOBup) considering the difference between pressure at the end of the nasal cannula and Prp. The pressure at the end of the nasal cannula was considered constant and equal to the Prp at zero flow. With this assumption, WOBup includes the resistance of the upper airways and the load due to the fluctuation of the generated pressure. To account for variations in VT, WOB was normalised by it.
In order to better compare the effect of NCPAP and HHHFNC, the comparison was performed at the same level of Prp (max difference 1 cmH2O). In particular, each parameter was evaluated at a Prp as close as possible to 2 and 4 cmH2O. A minimum of 15 breaths free from artefacts were selected, and the analyses were performed on each breath.
Statistical analysis
Sample size estimation was based on finding a clinically significant difference in WOB between NCPAP and HHHFNC. Calculations (Sigmaplot 11.0, Systat Software), indicated that 14 subjects would be sufficient to reject the hypothesis of equivalence with 80% probability using an α of 0.05, given that means differed by at least 40%. Mean and SD were taken from Saslow et al.20 To account for patients potentially unable to be included in the comparison, we recruited 20 subjects. ANOVA on ranks for repeated measurements was used to test the significance of differences among the six conditions of ventilation support. Multiple comparisons after ANOVA were performed using the Tukey test. Differences were considered statistically significant for p<0.05. Data are reported as median (IQR).
Results
Patients’ characteristics
Twenty infants were enrolled from December 2011 to June 2012. GA was 31 (30+6; 32) weeks, postnatal age 49 (35;79) hrs and birth weight 1490 (1404; 1657) g. Prior to commencement of non-invasive respiratory support the patients had a Silverman score of 6 (5; 6) and a FiO2 requirement between 0.3 and 0.6. At the time of the enrolment, 13 infants were receiving NCPAP at 4–6 cm H2O, while the other seven were on HHHFNC at 4–6 L/min. During the study, FiO2 was between 0.21 and 0.25 for both the modalities.
All ventilation modalities/settings were well tolerated by all infants. No interventions, including FiO2 adjustments, were required to maintain SpO2 in the range 88–93%, suggesting that, by the time of the study, most of the patients had improved. This consideration explains relatively high values of compliance found in few patients.
Generated end-expiratory pressure
Figure 2 shows experimental traces of a representative infant during NCPAP and HHHFNC at an end-expiratory Prp of 2 cmH2O. Changes in Pes and transpulmonary pressure (PL) are reported instead of absolute values as in supine patients only changes in pleural pressure can be accurately estimated from Pes.21 ,22 VT was similar in the two modalities, while Prp and Pes presented higher intratidal variations during HHHFNC.

Experimental tracings: retropharyngeal pressure (Prp), changes in oesophageal pressure (ΔPes), changes in transpulmonary pressure (ΔPL), volume changes (ΔVL), abdominal and thoracic contributions to lung volume changes (Vab and Vrb) of a representative infant during nasal continuous positive airways pressure (NCPAP), and heated, humidified, high-flow nasal cannula (HHHFNC) at a pressure of end-expiration Prp of 2 cmH2O.
The relationship between flow rate (V’) in HHHFNC and the level of end-expiratory Prp is shown in figure 3. There was a poor correlation between the variables as determined by linear regression, even when flow values were corrected for infants weight (Prp=0.3+0.7*V’; r2=0.37). The maximum Prp recorded at end-expiration was 7 cmH2O.

Linear regression between flow rate divided by infants’ weight and end-expiratory Prp in heated, humidified, high-flow, nasal cannula (HHHFNC) (Prp=0.3+0.7*V’; r2=0.37).
NCPAP at settings of 2, 4, 6 cmH2O achieved an end-expiratory pressures of 2, 4 and 6 cmH2O at the level of the retropharynx. HHHFNC was able to produce an end-expiratory Prp of 2 cmH2O in all 20 infants, while Prp of 4 cm H2O was obtained only in 15 infants and of 6 cmH2O in 5 infants. For this reason, the comparisons were limited to 15 infants at Prp of 2 and 4 cmH2O. During HHHFNC, Prp of 2 cm H2O was reached in 4 infants with 2 L/min and in 11 infants with 4 L/min, while Prp of 4 cmH2O was reached in 4 infants with 4 L/min and in 11 infants with 6 L/min.
Comparison between NCPAP and HHHFNC
Detailed comparisons between HHHFNC and NCPAP can be found in table 1. No statistically significant differences were found between HHHFNC and NCPAP on breathing pattern parameters, gas exchange and respiratory mechanics.
Pressure swings, breathing pattern, lung mechanics, gas exchange and WOB during HHHFNC and NCPAP at 2 and 4 cmH2O of end-expiratory retropharyngeal pressure
RR and %RC were lower and IAI was higher during HHHFNC than NCPAP but without reaching statistical significance. Increasing Prp from 2 to 4 cmH2O produced similar effects during the two modalities: a significant reduction in RR and a slight increase in VT and PtcO2.
Figure 4 shows WOBi, divided into WOBup and the component due to the lower part of the respiratory system. At a Prp of 4 cm H2O, the inspiratory WOBup was significantly higher during HHHFNC than NCPAP. However, we did not observe any significant difference in terms of WOBi, because WOBup contributes only a small part (16%) to the total.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Inspiratory work of breathing (rWOBi) with underlined the resistive component (rWOBi) and the component due to the upper airway (WOBup). * p<0.5 between WOBup during heated, humidified, high-flow, nasal cannula (HHHFNC), and nasal continuous positive airways pressure (NCPAP) at 4 cmH2O.
Discussion
This study compared the effects of HHHFNC and NCPAP on breathing pattern, gas exchange, lung mechanics and WOB in premature infants with RDS at equivalent applied Prp. At the considered Prp, there was no difference in gas exchange, WOB and lung mechanics between NCPAP and HHHFNC.
Generated end-expiratory pressure
In our study, during HHHFNC, only 75% of infants reached an end-expiratory Prp of at least 4 cmH2O and values over 5 cm H2O were rarely achieved, suggesting that HHHFNC, as currently applied in the clinical settings, provides lower continuous distending pressures than those commonly used in NCPAP.
The correlation between the HHHFNC flow rate and Prp was quite poor, consistently with previous reports.1–2 The slope of the linear regression differed from the one reported previously (1.1 cmH2O*min*kg/L)26 suggesting that, in addition to the wide intersubject and intrasubject variability in the amount of pressure developed for a given flow rate,25 there may also be large between-centre variability.
Comparison between NCPAP and HHHFNC
No statistically significant differences were found either in gas exchange, breathing pattern, thoraco-AB asynchrony or WOB between the two modalities, in agreement with previous studies.17 ,20 ,27 Interestingly, a lower mean RR was noticed in HHHFNC than in NCPAP, when compared at the same Prp. Although not statistically significant, the difference could be clinically important and has been previously reported in adult studies.28 It is important to underline that in this study, as distinct from the previous ones,20 ,27 the comparison of the two techniques at the same distending pressure was aimed to better understand the role of one of the possible mechanisms of action and, because of this, its application differs from how HHHFNC is most commonly applied in clinical practice.
Upper airways resistance during HHHFNC
Although no difference was found between NCPAP and HHHFNC in total WOB, at a Prp of 4 cmH2O the WOBi was slightly higher during HHHFNC than NCPAP. In particular, WOBiup was significantly higher during HHHFNC. This difference is likely due to the fact that within-breath changes in Prp are higher during HHHFNC than during NCPAP. In fact, during HHHFNC the resistance determined by the leak is flow-dependent, which means that even small changes in flow can produce significant changes in pressure. Moreover, the bias flow during HHHFNC (generally 2–8 L/min) is lower than during NCPAP (generally 15 L/min) and, therefore, the tidal flow associated to the infants’ spontaneous breathing (generally 1 L/min) plays a more significant role. However, as rWOBup represents a small part of WOBi, this potential drawback of HHHFNC appears not to be clinically relevant.
Limitations of the study
Changes in oesophageal pressure may not accurately reflect changes in pleural pressure because of suboptimal positioning of the balloon, or when the chest wall distortion results in an uneven distribution of pleural pressure changes. However, as no differences were observed in thoraco-AB asynchrony between NCPAP and HHHFNC, possible inaccuracies should have equally affected the measurements, allowing reliable intrasubject comparisons.
Even if RIP is considered reliable for determining tidal changes in VL in preterm infants,29 accuracy of the calibration coefficients may be affected by movements during measurements.
WOB has been computed without considering the relaxation curves of the lung and the chest wall, as they cannot be accurately assessed in spontaneously breathing infants. Therefore, the estimation of WOB is based on the following assumptions, commonly used in this kind of studies20: (1) changes in total respiratory system pressure-volume curve around the operating lung volumes are mostly due to the lung; (2) the compliance is constant over the breath and (3) end-expiratory lung volume does not change significantly within each protocol step.
Conclusions
When similar end-expiratory pressures are applied, in spite of the differing mechanisms of pressure generation, NCPAP and HHHFNC show comparable effects in terms of breathing pattern, gas exchange, lung mechanics and work of breathing in preterm infants with mild-moderate RDS.
Acknowledgments
We thank Branka Cupic, MD, for providing advices and assistance in the use of HHHFNC device.
References
Footnotes
-
Contributors AL: contributed to the study design, took part to the experimental activity, drafted the manuscript. CV: contributed to the study design, took part to the experimental activity, carried out data processing and drafted the manuscript; MC: contributed to the study design, data interpretation and manuscript revision. FC: took part to the experimental activity and data analysis. EZ: contributed to the interpretation of the data and to the preparation of the manuscript. MF, MD: took part to the experimental activity. FM: contributed to the study design and data interpretation and to the preparation of the manuscript. RLD: contributed to the study design, supervised the experimental activity and data interpretation and contributed to the preparation of the manuscript.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Human Ethics Committee of the Fondazione IRCCS Ca’ Granda, Ospedale Maggiore Policlinico in Milan.
-
Provenance and peer review Not commissioned; externally peer reviewed.