Article Text

Abstract
Objective: To determine the effects of a multifaceted paediatric rapid response system on the duration of predefined clinical instability and the subsequent rate of cardiac arrests.
Methods: An interrupted time series study coupled with a retrospective chart review to evaluate the effects of implementing a four component paediatric rapid response system. All patients in a 136-bed university-affiliated paediatric hospital from August 2003 to May 2007 were considered. The main outcome measures included rate of cardiac arrests as indicated by the number of patient days between ward paediatric cardiac arrests and duration of predefined clinical instability before evaluation by critical care personnel.
Results: The mean time interval between cardiac arrests increased significantly with the establishment of the rapid response system from a baseline of 2512 to 9418 patient days. The median duration of clinical instability decreased from 9 h 55 min to 4 h 15 min post intervention (p = 0.028).
Conclusions: The implementation of a paediatric rapid response system is associated with a significant reduction in the rate of cardiac arrests and duration of clinical instability before evaluation by critical care personnel. This study provides evidence that implementation of a rapid response system brings emergency personnel to deteriorating patients earlier, thus preventing cardiac arrests.
Statistics from Altmetric.com
Despite advancements in resuscitation, the death rates for hospitalised patients who had cardiac arrest remain high.1 2 3 4 Only 17% of adults and 27% of paediatric patients survive to hospital discharge after cardiac arrest.5 6 It is well established that antecedents often exist before cardiac arrest.7 8 9 10 11 12 13 The prevalence of such warning signs prompted the creation of rapid response systems (RRS) to allow for rapid evaluation and treatment of any patient meeting predetermined criteria for clinical instability. Individual centres with these systems have reported significant decreases in hospital cardiac arrests and mortality in adult and paediatric patients.14 15 16 17 18 19 However, the only randomised multicentre study showed no difference in mortality or cardiac arrests between groups.20 A driving force to investigate the effective aspects of RRS is fuelled by pressure from healthcare regulating and safety organisations to implement these systems throughout all hospitals.21 22
It has been theorised that the implementation of an RRS improves efficiency in recognising and responding to clinically deteriorating patients.15 23 We hypothesised that implementation of a four component paediatric rapid response system (PRRS) would decrease the rate of cardiac arrests and the duration of clinical instability before critical care personnel evaluation.
Methods
Context
This study was conducted at a 136-bed university-affiliated paediatric hospital with approximately 5900 annual admissions. All patients in the hospital from August 2003 to May 2007 were considered with full implementation of a PRRS completed on 1 August 2005. All paediatric medical and surgical services are provided including emergency, outpatient, trauma, cardiac surgery, organ transplantation and extra corporeal life support. This study was approved by the Institutional Review Board. Requirement for informed consent was waived.
Development of a PRRS
Prior to development of the PRRS, the emergency response system was structured according to the “traditional” cardiac arrest team concept in which the team was summoned for a cardiac or respiratory arrest. Critical care assessment for less emergent cases involved the typical chain of events leading to unplanned admission to the paediatric intensive care unit (PICU) as shown in fig 1 (before PRRS).
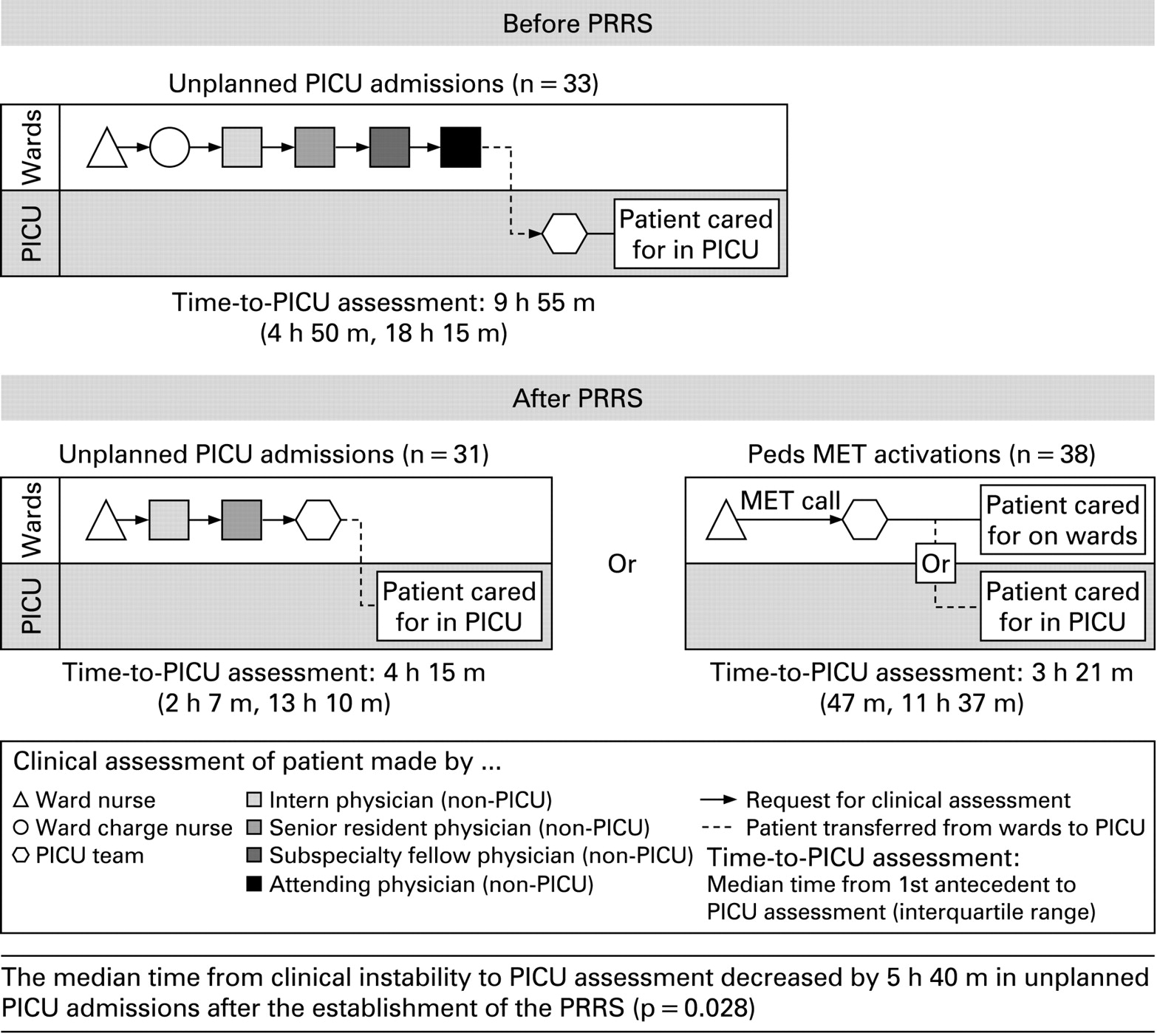
Process flow map from clinical instability to PICU assessment—before and after PRRS. The median time from clinical instability to PICU assessment decreased by 5 h 40 min in unplanned PICU admissions after the establishment of the PRRS (p = 0.028).
The PRRS was designed to include four components: (1) afferent, (2) efferent, (3) process improvement and (4) administrative limb. The afferent limb is the component of the system that is able to detect an event and trigger a response. The efferent limb provides a crisis response including the responding medical emergency team (MET). The process leading to activation of the PRRS is shown in fig 1 (after PRRS). The process improvement limb exists to improve patient care and safety. Finally, the administrative limb exists to implement and sustain the service.23
Published antecedents along with antecedents identified in chart reviews of cardiac arrests from our institution were used to establish the criteria for activation of the PRRS.7 8 9 10 11 12 13 Activation criteria were displayed in poster format throughout the hospital. The MET included a paediatric critical care fellow, resident, critical care nurse and respiratory therapist. The MET had all of the following competencies: (1) ability to prescribe therapy; (2) advanced airway management; (3) capability to establish central venous access; and (4) ability to begin ICU care at the bedside.23
All PRRS and code blue calls were regarded as possible cardiac arrests. The same team responded to all paediatric medical emergencies in areas excluding the neonatal and paediatric ICU and operating suites. Upon arrival the MET provided medical evaluation and treatment as required. A PRRS data collection form was completed by the MET and then collected by the investigators. The timeline illustrating implementation of the four component PRRS is shown in fig 2.

PRRS implementation timeline. *Root cause analyses conducted as needed.
Outcome measures
The primary outcome measures included:
Number of patient days between ward cardiac arrests (ward is defined as any patient area excluding any ICU, operating room or emergency department)
Duration of clinical instability before evaluation by critical care personnel
Secondary measures included:
Number of ward cardiac arrests/1000 ward admissions
Number of ward and PICU deaths/1000 ward and PICU admissions
Process measures
Number of PRRS activations/1000 ward admissions
Time interval ICU personnel were away from PICU
Two independent physicians conducted a retrospective review of the patient charts for which the PRRS was activated during the 12 months after implementation. There were a total of 68 PRRS activations but only 59 charts available for review. In addition, 42 of 126 unplanned PICU admissions that occurred during the 12-month period before PRRS and 41 of 128 unplanned PICU admissions from the 12-month period after PRRS were randomly selected for review. The unplanned PICU admissions reviewed did not include cardiac arrests, respiratory arrests or PRRS activations. All charts were reviewed to evaluate the type of event and presence and duration of documented clinical instability during the 24 h before the event. The reviewers were not blinded from the patient outcomes and PRRS intervention but were not aware of the other physician reviewer’s analysis.
Events were classified as unplanned PICU admissions, PRRS activations, cardiac arrests or respiratory arrests. An unplanned PICU admission was defined as any patient who was transferred from the wards to the PICU. A PRRS activation was defined as any patient for whom the MET responded. Using Utstein reporting guidelines, cardiac arrest was classified as the cessation of detectable cardiac mechanical activity, determined by the absence of a palpable pulse, responsiveness and apnoea.24 25 To determine duration of clinical instability, documented antecedents were recorded if they met the predefined criteria described in table 1.
Reviewer analysis for antecedents
Only antecedents documented with both a time and date were recorded. If only one reviewer found an antecedent in the medical record that antecedent was excluded. If both reviewers recorded an antecedent but at different time intervals, the time nearest that of critical care personnel assessment (ie, shortest duration of instability) was used in the analysis.
Statistical analysis
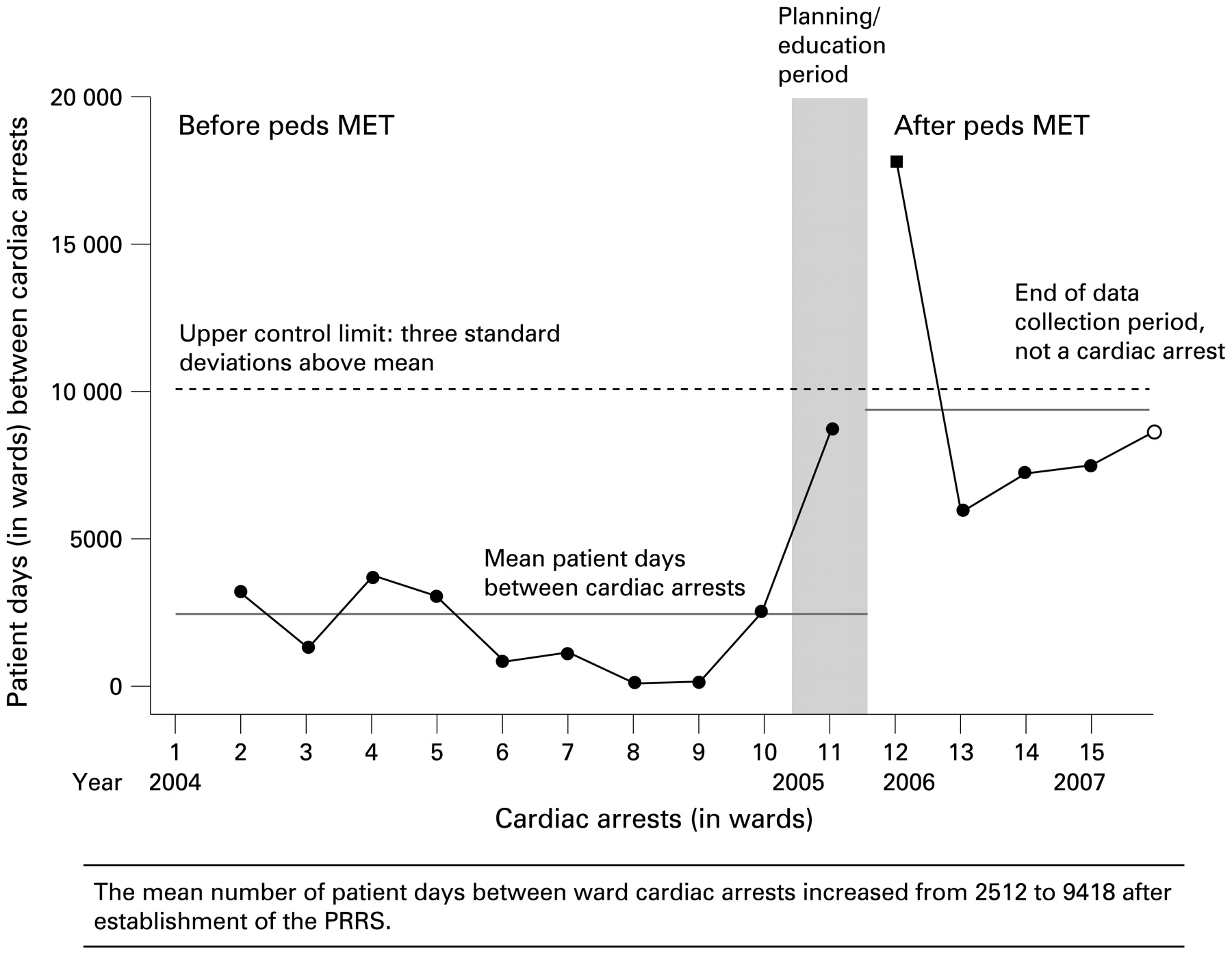
Minitab V.15.1 was used to analyse data. Measures such as number of patient days between a cardiac arrest follow a geometric distribution. Each patient day is considered an independent Bernoulli trial with the same probability of an arrest (fig 3). The horizontal lines plotted on the control chart are computed based on the geometric distribution. The mean and upper control limits define the central tendency and expected spread of the data for a stable system. A stable system is one in which the natural variation for the system occurs over time. Following Shewhart’s method, the control limits are 3 SDs from the mean and points outside a limit indicate a significant change in the system. This method was used to analyse cardiac arrest data.28 29
{kind=link}
{kind=link}
{kind=link}
Patient days (in wards) between cardiac arrests (n = 15 cardiac arrests). The mean number of patient days between ward cardiac arrests increased from 2512 to 9418 after establishment of the PRRS.
Mortality and cardiac arrest rates were calculated per 1000 admissions. Statistical analysis consisted of the one-tailed Fisher’s exact test. Statistical p values and risk ratios (RR) with associated 95% confidence intervals (CI) are reported with significance defined as p<0.05.
To document the inter-rater reliability, the number of disagreements was divided by the number of dual-reviewed charts times the nine potential antecedents per chart. One minus this number yielded an inter-rater reliability index. A one-tailed Mann-Whitney test was used to evaluate non-normally distributed data, such as median time interval from first documented antecedent to ICU assessment.
Results
The mean number of patient days between ward cardiac arrests increased significantly from 2512 to 9418 after establishment of the PRRS (fig 3). The data point outside the upper control limit indicates a significant change to the system. The ward cardiac arrest rate/1000 ward admissions was 1.27 before PRRS implementation and 0.45 after PRRS implementation with an RR of 0.35 (95% CI: 0–1.24; p = 0.126) (table 2).
Mortality and cardiac arrests
The ward death rate/1000 ward admissions was 1.5 before PRRS implementation and 0.45 after PRRS implementation with an RR of 0.30 (95% CI: 0–1.04; p = 0.070). This death rate included patients with do not resuscitate orders since there was not a reliable means for querying the mortality data for do not resuscitate orders.
A total of 151 charts were examined by both reviewers. Of 1359 opportunities for disagreement, only 184 disagreements occurred yielding an inter-rater reliability of 86.5%. Antecedents were found by both reviewers in 38 of 59 PRRS activations, 33 of 42 unplanned PICU admissions (before implementation of the PRRS) and 31 of 41 unplanned PICU admissions (after implementation of the PRRS). There was no significant difference in the number of unplanned PICU admissions, hospital admissions or paediatric cardiac surgery cases in the study periods.
In the evaluation of unplanned PICU admissions the median time interval was determined by the amount of time from first documented antecedent to ICU assessment (fig 1). This time interval decreased from 9 h 55 min before PRRS implementation to 4 h 15 min after PRRS implementation (p = 0.028). Likewise, for PRRS activations the median time interval from first documented antecedent until ICU assessment was 3 h 21 min.
The measures used to evaluate the PRRS such as activation personnel, activation criteria and outcomes are summarised in table 3. The median duration of MET assessment, or time away from the ICU, was 19 min. The median number of PRRS activations was 14/1000 ward admissions.
PRRS activations from August 2005 to July 2006 (n = 68)
Discussion
In contrast to prior studies, this is the first to demonstrate that a PRRS significantly reduces the time interval from documented clinical instability to ICU staff assessment. The duration of clinical instability significantly decreased for unplanned PICU admissions whether or not assessed by the MET, indicating that implementation of a PRRS resulted in a hospital-wide culture change favouring early critical care personnel assessment. The group with the shortest duration of documented clinical instability was the PRRS activation group. As demonstrated in the only multicentre trial of METs, the isolated intervention of making an MET available in a hospital setting does not ensure success in decreasing cardiac arrests and mortality.20 In fact, similar to this study, centres with reported decreases in cardiac arrests and mortality have utilised RRS interventions with several components in addition to the MET.23
In this study, we showed a decrease in cardiac arrest rate as indicated by a significant increase in patient days between cardiac arrests. For events that yield high death rates, like cardiac arrests, Shewhart control charts improve the likelihood of identifying rate changes in a clinically significant period. Traditional statistical tests such as the Fisher’s exact test require unfeasible periods to detect a significant change for rare event data such as paediatric cardiac arrests. The use of this approach to evaluate rare event data is recommended by many industry and healthcare organisations.28 29 30 This method of analysis is the most appropriate model for our study examining paediatric cardiac arrest rates. During the study period, we did not detect an increase in cardiac arrest rates in the intensive care unit. In fact, there was a decrease in cardiac arrest rates of the combined PICU and ward cardiac arrests per 1000 admissions from 4.07 to 2.04 after the PRRS intervention. This contradicts the theory that patients were transferred to the ICU and merely experienced cardiac arrest in a different location.
As with every research endeavour, there were limitations to our study. First, we were reliant upon humans to trigger the system. While non-human based monitoring systems able to recognise an escalating risk of cardiac arrest and activate an RRS do exist, they have not been well studied and are not available for a paediatric population. Second, this study was an interrupted time series in one hospital. There is the possibility of some other factor contributing to the increase in days between cardiac arrests and reduction in duration of clinical instability. However, we are unaware of any factors that could have influenced our results in this period. Finally, it is possible that the benefits described in our paper occurred by merely focusing hospital-wide efforts on improving recognition and resuscitation skills. Although we believe that the sustained improvement we found could not be attributed to education alone, it is not clear which components of the PRRS are the most important in preventing cardiac arrests.
Conclusions
In conclusion, the introduction of a PRRS was associated with both an increase in the number of patient days between ward cardiac arrests and a decrease in the duration of clinical instability before critical care personnel assessment. It is likely that earlier assessment of deteriorating patients by critical care personnel can prevent cardiac arrests and lead to the increased number of patient days between ward cardiac arrests. A recent commentary’s authors cautioned that efforts to improve patient safety, such as RRS, should be supported by sufficiently strong evidence to warrant such a commitment of resources.31 This effective system was implemented without the need for additional staff or unfeasible work load additions to the MET members. We believe the traditional structure of a “code blue team” is unsatisfactory and the need for a carefully designed system change to prevent cardiac arrests such as an RRS is a feasible way to prevent in-hospital cardiac arrests.
Acknowledgments
We thank Lloyd Lloyd Provost, MS, of Associates in Process Improvement, Austin, Texas, USA, for his advice and assistance in creating rare event control charts and statistical analysis.
REFERENCES
Footnotes
Competing interests None.