Article Text

Abstract
Introduction Non-invasive ventilation (NIV) is part of standard care in amyotrophic lateral sclerosis (ALS). Intolerance or unavailability of NIV, as well as the quality of correction of nocturnal hypoventilation, has a direct impact on prognosis.
Objectives We describe the importance of NIV failure due to upper airway obstructive events, the clinical characteristics, as well as their impact on the prognosis of ALS.
Methods Retrospective analysis of the data of 190 patients with ALS and NIV in a single centre for the period 2011–2014. 179 patients tolerating NIV for more than 4 h per night without leaks were analysed.
Results Among the 179 patients, after correction of leaks, 73 remained inadequately ventilated at night (defined as more than 5% of the night spent at <90% of SpO2), as a result of obstructive events in 67% of cases (n=48). Patients who remained inadequately ventilated after optimal adjustment of ventilator settings presented with shorter survival than adequately ventilated patients. Unexpectedly, patients with upper airway obstructive events without nocturnal desaturation and in whom no adjustment of treatment was therefore performed also presented with shorter survival. On initiation of NIV, no difference was demonstrated between patients with and without upper airway obstructive events. In all patients, upper airway obstruction was concomitant with reduction of ventilatory drive.
Conclusions This study shows that upper airway obstruction during NIV occurs in patients with ALS and is associated with poorer prognosis. Such events should be identified as they can be corrected by adjusting ventilator settings.
Statistics from Altmetric.com
Introduction
Amyotrophic lateral sclerosis (ALS) is a neurodegenerative disease of unknown origin. After onset of the first symptoms, the median survival without respiratory assistance is 19 months1 and about 7 months in patients with documented diaphragmatic involvement.2 Most deaths are due to respiratory causes.3 For these reasons, non-invasive ventilation (NIV) is now part of standard care of ALS.4 ,5 By delivering positive pressure ventilatory assistance via a nasal or face mask, NIV relieves dyspnoea and improves quality of life.6 The survival benefit of NIV has been reported to range from 7 months7 to 12 months or more.8 ,9 Intolerance of NIV or lack of availability of NIV8 ,9 is a missed opportunity to improve quality of life and prognosis.4 However, initiation of NIV is more difficult in patients with ALS than in patients with other neuromuscular diseases,10 while the quality of correction of nocturnal hypoventilation has a direct impact on prognosis.11 The failure of NIV to maintain satisfactory ventilation at night is related to the presence of leaks in more than half of the cases,11 but other mechanisms, sometimes associated, are also involved, including upper airway obstructive events, central events comprising reduction of the ventilatory drive and patient-ventilator asynchrony.11 ,12 When nocturnal hypoventilation persists after correction of leaks, it is recommended to perform respiratory polygraphy during NIV to identify the mechanisms responsible.13 We describe the role of upper airway obstructive events in failure of NIV in patients with ALS, their clinical characteristics and their intrinsic prognostic impact.
Material and methods
Background
This single-centre observational study was conducted in the Department of Respiratory Medicine and Medical Intensive Care of a 1600-bed university hospital. This department is associated with the rare diseases reference centre for ALS in the same hospital. Initiation and surveillance of NIV in patients with ALS is performed in an 8-bed day-care unit, according to a recently validated model,14 which devotes 80% of its activity to the management of respiratory failure in ALS.11
Patients
Between 2011 and 2012, NIV was initiated in our centre in 190 patients with definite or probable ALS according to El Escorial criteria,15 and the patients' outcome was followed until 2014. NIV was well tolerated (NIV >4 h/24 h) by 179 of these patients8 (figure 1). All these patients were included in the analysis. Analysis of these data was approved by the Institutional Review Board of the Société de Pneumologie de Langue Française (French learned society for respiratory medicine), and all patients provided their written informed consent to the anonymous use of their personal data. All the patients received riluzole, and, as appropriate, secretions management with In/Exsuffflator and gastrostomy. The patients and their caregivers all received logistical and psychological support from the Paris ALS Network care.16
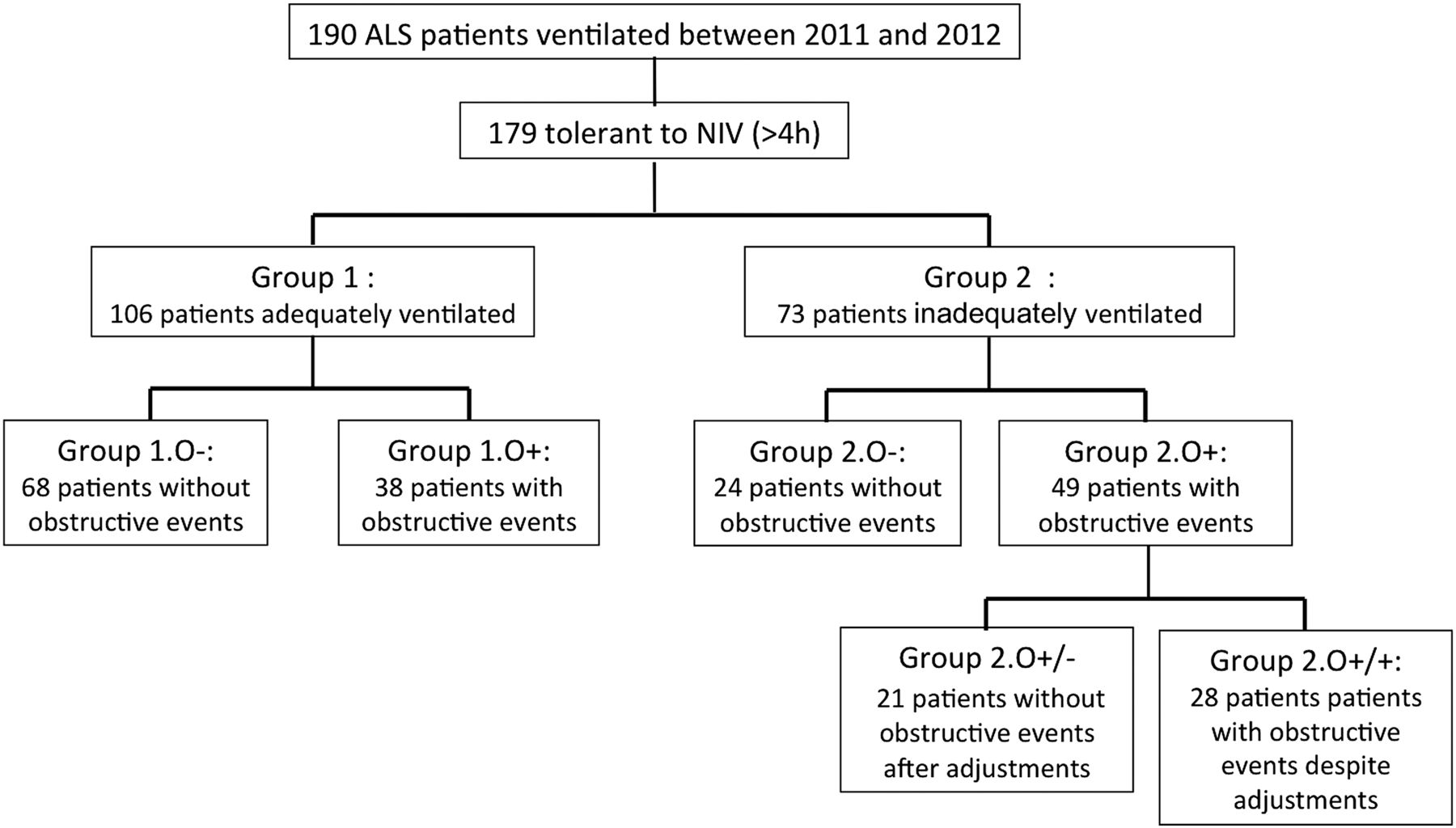
Flow chart of the patients included.
Respiratory management and evaluation
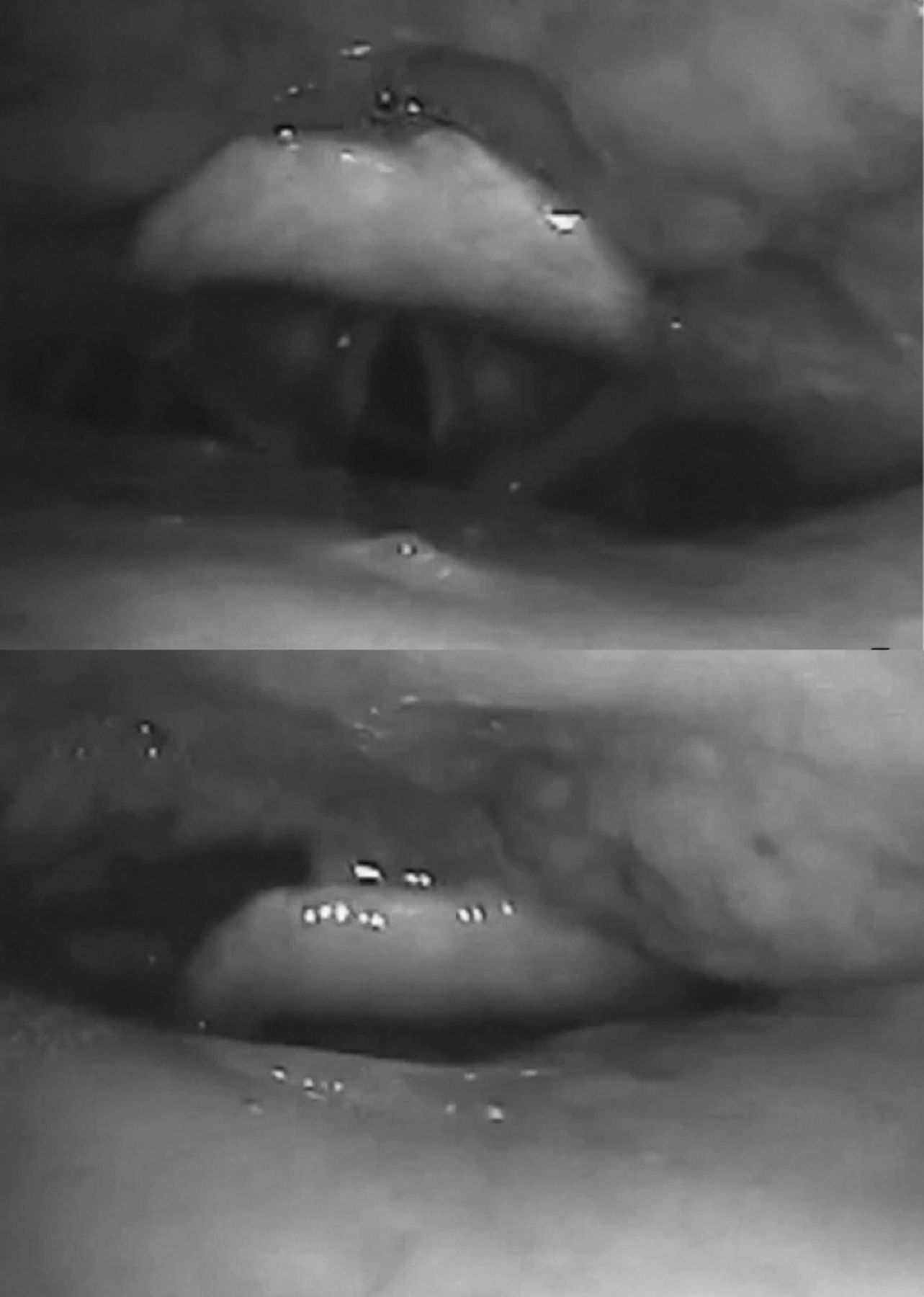
The indication for NIV was based on the current consensual criteria.5 NIV was initiated according to the current standardised procedure in the department over a period of 3–5 days17 (table 1). During the follow-up, the effectiveness of NIV was assessed in terms of symptoms (including NIV-related discomfort), blood gases, the analysis of ventilator-recorded tracings and nocturnal oximetry. This was performed in all patients in a systematic manner after 1 month of NIV (M1) and then every 3 months as described previously in detail.11 Patients were considered to be inadequately ventilated (16) at night when they presented with nocturnal SpO2<90% for more than 5% of the nocturnal recording time.11 Built-in monitoring software was used to detect air leaks, which were then corrected. In the absence of leaks,18 ventilator software was able to detect with good accuracy possible obstructive events (see previous report for details11) (figure 2) and nap polygraphy (or polysomnography for five patients) was then performed in all the patients who were inadequately ventilated and who were suspected to have upper airway obstructive events (figure 2).13 An obstructive event on NIV was defined by a ≥50% drop in airflow for 10 s or longer19 with no concomitant changes in the amplitude of the pressure signal13 and was considered to be associated with a reduction in the ventilatory drive13 when it occurred in the absence of an associated thoracoabdominal paradox.19 The absence of obstructive events was defined by an obstruction index <5/h on the ventilator software.20 All the patients were ventilated with a respiratory backup rate to provide for central apnoeas.13 Pharyngolaryngeal assessment was also performed by nasal endoscopy (Pentax, VNL-1190STK) during spontaneous breathing in 11 patients and non-invasive ventilation in one patient (figure 3 and online supplementary video).
Patient characteristics

Upper part: Example of decreased nocturnal SpO2 recorded on polysomnography with reduction of flow (arrows) despite effective ventilator pressure, indicating obstruction associated with reduction or even absence of thoracoabdominal muscle movements. This obstructive event was corrected by increasing EPAP (circle). Lower part: same event recorded by the ventilator built-in monitoring software showing decreased flow rate (arrows) despite effective ventilator pressure (Rescan, Resmed, Sydney, Australia). EPAP, expiratory positive airway pressure

Awake nasopharyngeal fibre-optic endoscopy on spontaneous breathing (upper part) and on NIV (lower part): Immediate obstruction of the upper airway at all the levels, from the tongue to the glottis. NIV, non-invasive ventilation.
Supplementary video
Interventions in case of inadequate ventilation due to obstructive events
After correction of the leaks, the corrective interventions in patients were, in this order: 1/a step-by-step increase in expiratory positive airway pressure (EPAP) to a maximum of 10 cmH20, if tolerated; 2/trial use of self-adapting inspiratory pressure devices (IVAPS mode, Resmed, Sydney, Australia; AutoAdvanced, Philips Respironics, Pensylvania, USA); 3/switch to volume-controlled mode; 4/trial of other mechanical treatments (mandibular advancement device, cervical collar).
Statistical analysis
Descriptive statistics used numbers and percentages for qualitative variables and Quantitative variables were described in terms of their median and IQR because of the strong skewness in some distributions. Comparisons between groups of patients used χ2 tests for qualitative variables and Wilcoxon-Mann-Whitney tests for quantitative variables. Prognostic factors were analysed in the framework of survival analysis. Survival time was defined as the time between first signs of the disease and date of death. Patients alive at the date of analysis were considered to be censored at this date. Survival functions were estimated by the Kaplan-Meier method and between-group comparisons were tested by log-rank tests. All computations were performed by SAS V.9.3 (SAS Institute Inc, Cary, North Carolina, USA).
Results
After correction of leaks, 106 of the 179 patients evaluated were considered to be adequately ventilated at night (group 1) and 73 remained inadequately ventilated (group 2) (see online supplementary table S2 and figure 1).
Supplemental material
In group 2, for 49 patients (67% of inadequately ventilated patients), poor ventilation was due to obstructive events (group 2 O+). Correction was obtained in 21 of these 49 patients after adjustment of ventilator settings (group 2 O±) (titration of EPAP up to 10 cm H2O guided by polygraphy and tolerance, followed, in the case of failure, by a trial of automatic modes (figure 2) and finally a trial of volume-controlled mode). Obstructive events could not be eliminated in 28 patients despite adjustment of ventilator settings (group 2 O+/+). In this case, ventilator settings were adjusted to ensure the least residual apnoeas and the best subjective tolerance.
In group 1, 38 patients presented with upper airway obstructive events (group 1 O+). However, in the absence of nocturnal desaturation and symptoms, no change of treatment was proposed in this group.
Results of pharyngolaryngeal endoscopic assessment in 11 patients are listed in the online supplementary material (figure 3 and online supplementary video).
Patients who remained inadequately ventilated after optimisation of NIV settings (to uncorrected obstructions (group 2 O+/+) or other causes (group 2 O−)) presented with shorter survival (respectively 14 [7–27] months and 12 [6–23] months) than ventilated patients without or corrected upper airway obstructive events (group 1 O− and group 2 O±) (respectively 26 [13–45] months (p=0.04 and 0.03) and 29 [20–53]months, (p=0.01 and 0.01)) (figure 4). Unexpectedly, Patients who remained inadequately ventilated after optimisation of NIV settings (due to uncorrected obstructions (group 2 O +/+) or other causes (group 2 O−)) presented shorter survival (13 [7–40] months) than did adequately ventilated patients without upper airway obstructive events after adjustments group 2 O+/− (p=0.026); and a survival that was not significantly different from that of patients considered to be inadequately ventilated.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Patient survival from onset of disease according to the presence of obstructive events, whether or not they were corrected. Group 1 O−: Group of patients without obstructive events and immediately adequately ventilated. Group 1 O+: Group of patients with obstructive events considered to be adequately ventilated. Group 2 O−: Group of inadequately ventilated patients without leaks or obstructive events. Group 2 O+/−: Group of patients with obstructive events inadequately ventilated and then adequately ventilated after treatment. Group 2 O+/+: Group of patients with obstructive events inadequately ventilated and remaining inadequately ventilated after treatment.
In the light of these results, we compared patients without and with upper airway obstructive events on the first recording (O−, n=92, ie, 51% and O+, n=87, ie, 49%, respectively). No significant difference was demonstrated between O+and O− patients at the time of initiation of NIV (table 1), except that group O− comprised more patients with bulbar onset ALS (24 patients vs 12, p=0.034), but with no significant difference of the bulbar score at the time of initiation of NIV, and Group O− comprised more patients with gastrostomy (n=21, 23%, vs n=9, 10%, in group O+, p=0.02), without difference in survival in patients with or without gastrostomy in the whole group. In the adequately ventilated patients, the patients with upper airway obstructive events had more desaturations but all for less than 5% of the night, and a shorter use of NIV (see online supplementary table S3).
In all O+ patients, obstructive events were consistently associated with a reduction of the ventilatory drive (figure 2). In the 20 patients in whom complete polysomnography (PSG) was performed, obstructive events occurred predominantly during rapid eye movement (REM) sleep but were always associated with loss of accessory respiratory muscle activity.
None of the patients presented with hyperventilation on NIV (table 1), and no significant difference in variations of PaCO2 without and with NIV was observed between O+ patients and O− patients.
The majority of patients were ventilated with a face mask, with no significant difference between the two groups.
O+ patients presented with more criteria of NIV failure: diurnal alveolar hypoventilation was less well controlled by NIV (PaCO2: 50 [44–55] mm Hg vs 43 [41–48] mm Hg in O− patients, p<0.001 and 67% of O+ patients (n=57) were hypercapnic (PaCO2 >45 mm Hg) on NIV versus 34% of O− patients (n=37), p<0.001.
Effective interventions in patients of group 2 O+ (n=49) were: (1) increased EPAP to the maximum of our protocol (10 cm H2O) for 18 patients (figure 2) (2) use of self-adapting inspiratory pressure devices in eight patients (IVAPS mode, Resmed, Sydney, Australia or AutoAdvanced mode, Philips Respironics, Pensylvania, USA) for three patients, (3) switch to volume-controlled mode in one patient (VT 500 mL, Ti1,3 EPAP 4). Other treatments were tried without success: a custom-made mandibular advancement device, as also recently described by Veldhuis et al,21 was tried in addition to NIV in four patients, but was discontinued after 3–6 months due to poor tolerance. Owing to the possible role of the oronasal mask, it was replaced by a nasal mask, which was not supported by the patients concerned due to air leaks. Anterior dislocation of the jaw using a cervical collar was tried, but without success, in three patients.
Discussion
This study confirms that upper airway obstruction is one of the mechanisms of NIV failure in ALS.10 ,11 ,21 ,22 The prevalence of upper airway obstruction, which has not been previously evaluated systematically, is high (45% of our patients after correction of leaks). It is noteworthy that NIV-related upper airway obstructive events in patients with ALS appear to be mediated by central mechanisms, as obstructive events (defined as cessation or a marked decrease of flow with maintained airway pressure) are associated with decreased or abolished thoracoabdominal movements (figure 2). Finally, obstructive events in this setting are associated with poorer prognosis, even when they do not reduce the efficacy of NIV to correct desaturations (group 1 O− patients) (figure 4). Correction of obstructive events improves survival (figure 4).
Putative mechanisms
Abnormal upper airway collapsibility in ALS
A number of ALS-related factors can theoretically increase upper airway collapsibility. Upper airway involvement has been extensively described in this disease, particularly in the pharynx and larynx,23 ,24 due to degeneration of corticobulbar fibres, with bilateral glossopharyngeal and hypoglossal nerve lesions responsible for so-called ‘bulbar’ symptoms with impairment of voice and swallowing, atrophy of the tongue with fasciculations and abnormal corticobulbar reflexes.23 ,25 Very heterogeneous appearances in endoscopy were observed, ranging from a completely normal airway to complete collapse of the entire airway (figure 3 and online supplementary video). However, recent studies in ALS have confirmed that the endoscopic appearance of the pharynx and larynx may be normal despite the spontaneous and permanent electromyographic activity of the tongue in a great majority of patients,26 although demonstration of fasciculations is limited by the marked difficulty of obtaining complete relaxation of the tongue (only 6% of patients25). More simply, DePaul et al24 demonstrated decreased strength of the tongue in almost all patients, even in patients with no dysarthria or swallowing disorders. The decreased strength of the tongue would constitute a predisposing factor to increased upper airway collapsibility and we believe that the prevalence of this abnormality in ALS (with or without an obvious bulbar lesion) is probably severely underestimated. Clinical evaluation (bulbar score) and nasal endoscopy are clearly unable to identify patients at high risk of upper airway collapse when treated by NIV, indicating the need for a specific diagnostic approach. We did not have enough data to differentiate between bulbar and pseudobulbar patients, a differentiation that should be explored in future studies. Finally, other mechanisms, described in different diseases, may also be responsible for upper airway obstruction; these include, for example, chronic irritation of the surface of the pharynx,27 ,28 a higher propensity of the airways to collapse at low lung volume29 ,30 or upper airway nocturnal redistribution of interstitial fluid.31
NIV-related inhibition of compensatory mechanisms
ALS-related obstructive events are observed only during sleep and/or NIV, suggesting the existence of wakefulness-related compensatory mechanisms that have been shown to involve cortical processes. A similar finding has been observed in obstructive sleep apnoea syndrome (OSAS), in which snoring and obstructive events are not observed during wakefulness, despite the fact that the upper airways of patients with OSAS present anatomical and functional abnormalities predisposing to airway collapse. These abnormalities are compensated for by the increased ventilatory drive to the upper airway dilator muscles,32 ,33 in which a specific cortical drive participates.34 NIV could affect this compensation via several mechanisms. First, NIV may reduce PaCO2, which would decrease the global ventilatory drive and could promote glottal closure phenomena in the same way as induction of hypocapnia in healthy participants.35 Second, NIV could induce mechanical inhibition of the ventilatory drive, independent of any variations in CO2, and related to changes in thoracic afferents36 and their cortical processing,37 as NIV abolishes the cortical activity related to breathing that characterises some patients with ALS, which has been interpreted to be a compensatory mechanism.38 Finally, a third mechanism could be related to sleep induction, as described in OSAS.39
Prognostic impact
In the patients of this series, obstructive events were associated with poorer prognosis, without any obvious confounder for low survival (smoking habits, riluzole use, respiratory secretions management and nutritional support). Of note, the presence of a gastrostomy was noted less often in the patients with obstructive events, probably because of the lower number of bulbar patients in this group (table 1). We did not find any difference in survival between patients with or without gastrostomy, as all the patients received nutritional support. We were surprised to find that a poorer survival was observed both in patients considered to be inadequately ventilated and in patients considered to be adequately ventilated, that is, with no nocturnal desaturations (group 1 O+ patients). Nocturnal SpO2 monitoring is therefore probably not sufficiently precise to detect poor quality sleep in patients with obstructive events or the criteria of nocturnal SpO2<90% for more than 5% of the nocturnal recording time11 could be too high as suggested in table 3 of supplementary material. However, this is an important point, as correction of obstructive events is associated with improved survival. The present study shows that adjustments of ventilator settings can control obstructive events in 58% of cases, with no survival difference between patients corrected during treatment and those who were adequately ventilated immediately. The most frequently effective treatment was to try to reduce upper airway collapsibility by increasing EPAP to high levels. Unfortunately, this was not always effective and no therapeutic intervention effective in all patients has yet been identified. Nethertheless, these differences in survival must be analysed with caution in this not controlled, retrospective study and should be confirmed in future controlled studies.
In conclusion, upper airway obstructive events associated with a decreased ventilatory drive and promoted by NIV are observed in more than half of the ventilated patients with ALS. The presence of this phenomenon must be systematically investigated, as it can be corrected by adjusting ventilator settings in the majority of cases. Although the retrospective and single-centre design of this study limits its impact, obstructive events nevertheless appear to be an important phenomenon with an impact on survival.
References
Footnotes
Contributors MG, VA, CM-P and JG-B were involved in the conception and design, acquisition of data, analysis, interpretation of data, drafting the work or revising. JLG, FS and TS were involved in the conception and design, analysis, interpretation of data, drafting the work or revising. LC-B was involved in the conception and design, acquisition of data, interpretation of data, drafting the work or revising. J-MC was involved in the acquisition of data, interpretation of data. AT, EM and VT-D were involved in the conception and design, acquisition of data, drafting the work or revising.
Funding This work was supported by the program "Investissement d'Avenir ANR-10-AIHU 06 of the French Government".
Competing interests None declared.
Ethics approval Institutional Review Board of the Société de Pneumologie de Langue Française (French learned society for respiratory medicine).
Provenance and peer review Not commissioned; externally peer reviewed.