Article Text

Abstract
Objective To determine whether a narrower gauge needle used in ABG sampling is associated with lower pain scores and complication rates without increasing the level of difficulty of the procedure.
Methods We performed a prospective single-blinded randomised control study of patients from a tertiary-level emergency department in Sydney who required an ABG analysis over the period of June 2010–July 2012. Patients were randomised to either a 23G or 25G needle and the primary outcome that included pain experienced by these patient were recorded as pain scores on a 10 cm hatched visual analogue scale. The difficulty scores and complications were also noted from the operator.
Results Data for 119 consenting eligible patients were included in the analysis. 63 patients were allocated to the 23G needle group and 56 to the 25G needle group. The mean pain score was 3.5 (SD=2.7) for the 23G group and 3.4 (SD=2.7) for the 25G group with a mean difference between the pain scores of 0.1 (95% CI −0.9 to 1.1, p=0.83). The 23G and 25G mean difficulty score was 3.4 (SD=2.6) and 4.3 (SD=2.4), respectively, with a mean difference of 0.9 (95% CI −0.03 to 1.7, p=0.06). 21.6% of patient in the 23G needle group experienced some complication with regard to the sampling in the form of haematoma, tenderness or paraesthesia in comparison to 5.4% of patients in the 25G needle group (p=0.03).
Conclusions There was no significant difference in pain scores experienced by patients undertaking ABG sampling with either a 23G or 25G needle.
Trial registration number ACTRN12609000957291.
- equipment evaluation
- clinical assessment
- research, clinical
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Key messages
-
What is already known on this subject?
-
It has been assumed that smaller gauge needles would inflict less pain on patients undergoing radial artery blood gas sampling, although there have been limited studies to confirm this theory.
-
What this study adds?
-
There was no significant difference in pain scores experienced by patients undertaking arterial blood gas sampling with either a 23 gauge or 25 gauge needle.
-
The patients exposed to the 23G needle had a higher percentage of complications.
Introduction
ABG analysis forms an essential tool for the assessment of gas exchange and acid–base balance in critically ill patients who present to the emergency department. The pain experienced by patients can be significant in arterial puncture1 compared with venous puncture due to the greater innervation of the arterial sites as well as the need to puncture deeper into the skin.
It has been assumed in the past that smaller gauge needles would inflict less pain on patients although there have been limited studies to confirm this theory.2 ,3 We hypothesised that a narrower gauge needle would be associated with lower pain scores and complications rates without increasing the difficulty of the procedure.
Methods
Study design and setting
We undertook a prospective single-blinded randomised control study at Westmead Hospital between June 2010 and July 2012. Westmead Hospital is a tertiary adult referral hospital in Sydney with an annual emergency department attendance of approximately 59 000. Approval of the study was obtained from South Western Area Health Services Human Research Ethics Committee and registered with the Australian New Zealand Clinical Trials Registry prior to commencement of the study.
Participants
All patients presenting to the emergency department deemed to need an ABG analysis as part of their diagnostic work up and able to consent were eligible to participate in the study.
Absolute Exclusion Criteria
-
patients with altered mental/cognitive states including language difficulties and unable to convey pain score accurately;
-
unwell patients requiring emergent medical intervention that precludes informed consent;
-
patients <16 years old.
Intervention
Candidates were randomised to the needle size by computer-generated block randomisation of 104 patients at a time in blocks of 8. Consent packs with information regarding the study were distributed by the doctors to potential study candidates. Once informed consent was obtained, the doctors would access the Study Pack, which contained all the equipment for the procedure including preallocated needle size, thus ensuring allocation concealment. The blinding process required patients to wear opaque glasses or close their eyes during the arterial puncture. A standardised data form was used to record all data collected during the procedure (figure 1). The primary outcome was the 10 cm hatched visualised analogue scale to record pain associated with the procedure (figure 2). A successful outcome was defined by collection of 0.5 mL arterial blood sample confirmed on analysis. A failed attempt was defined as <0.5 mL collection (inadequate sample volume), or a sample deemed venous on the blood gas analysis or more than three attempts were made by two proceduralists. At our institution, local anaesthetic use for urgent ABG sampling is not standard practice.
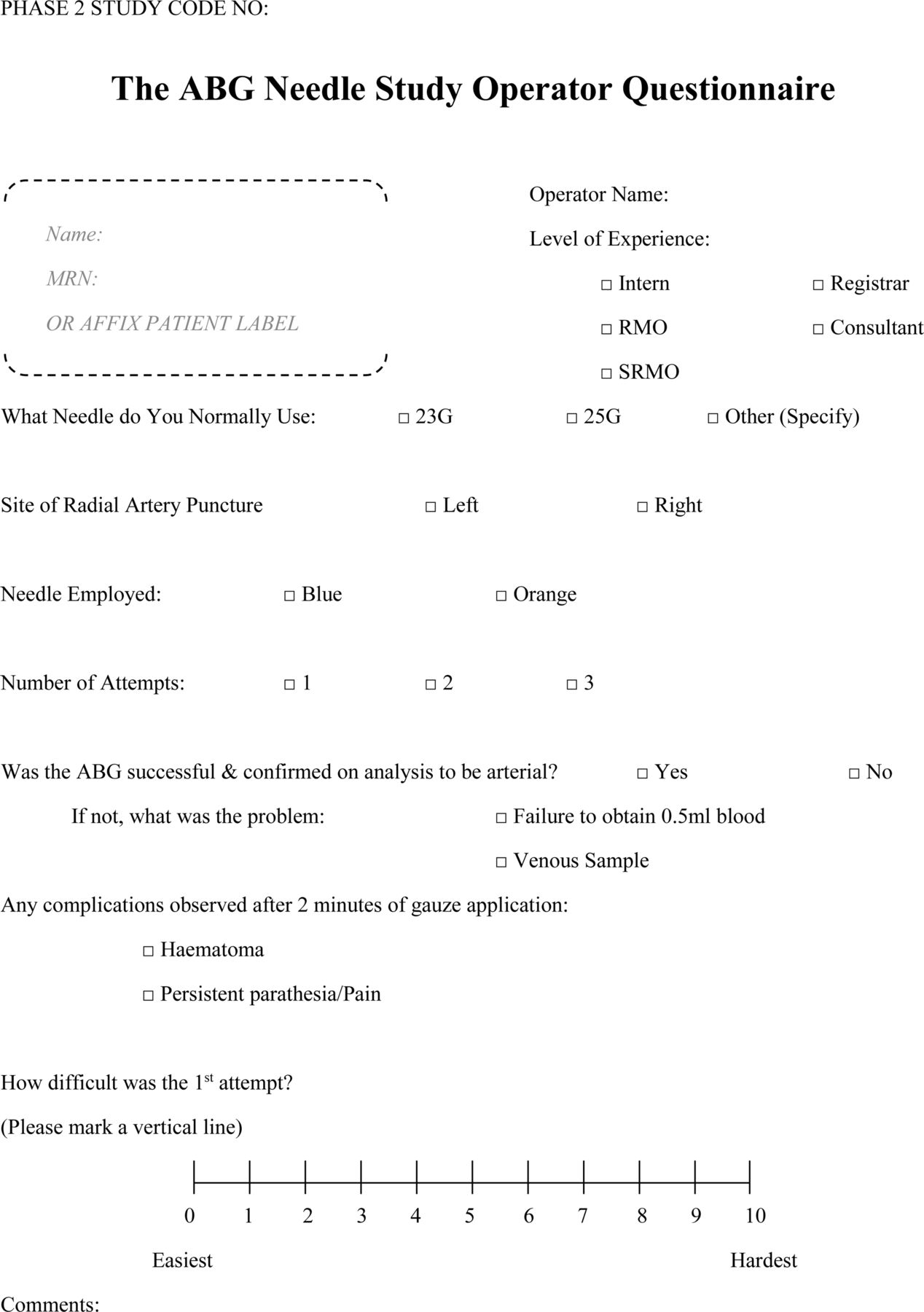
Operator questionnaire.

Patient questionnaire.
Equipment
The equipment used for the study included safePICO (Radiometer, Denmark) self-fill arterial sampler syringe with 60 IU balanced heparin, 23G (0.6 mm×32 mm) and 25G (0.5 mm×16 mm) needle (Becton Dickson Company PrecisionGlide Needle, Belgium).
Study outcome
Primary outcome
The degree of pain experienced by patients during an ABG puncture with different gauge needles measured on a 10 cm visual analogue scale (VAS).
Secondary outcome
The success rates during an ABG puncture with different gauge needles. Procedural difficulty as rated by the doctor performing the arterial puncture was also measured on a 10 cm VAS.
Additional data regarding complications were collected, although no predetermined definitions were incorporated into the study.
The categorical variables included site, gender, complications and operator experience level.
The continuous variables included pain and difficulty score.
Data analysis
Data were analysed using IBM SPSS Statistics for Windows V.21 (IBM Corporation 2012, Armonk, New York, USA). Two-tailed tests with a significant level of 5% were used throughout the analysis including comparing mean pain VAS scores. Fisher's exact test and Pearson's χ2 (as appropriate) were used to compare the distribution of categorical variables between needle groups.
Initial sample size calculations suggested the need for 200 patients to achieve statistically meaningful results. Due to patient recruitment difficulty, the study was discontinued after enrolment of 113 patients. Assuming a common SD of 2.7 for the pain scores in the two needle groups, our study had a 73% power to detect a difference of 1.3 or more in pain scores and a 97% power to detect a difference of two or more. A difference of at least 1.3 or more in the pain score has been demonstrated in the literature to be of clinical significance.4 ,5
Results
A total of 126 patients were enrolled in the study with 7 of them withdrawn due to incomplete data (figure 3). Three had no pain scores, two had no difficulty scores, one had neither pain/difficulty scores and one had no patient details. The groups did not differ in age or sex with the average age of the patient being 64.9 years (SD=15.6 years) and 51.3% of the participants were males (table 1). The preferred site was the right radial artery in 61.9% of cases, and this was similar between both groups (p=0.952). The mean pain score of the 23G needle group was 3.5 (SD=2.7) and for the 25G needle group 3.4 (SD=2.7) (table 2 and figure 4). The mean difference between the pain scores was 0.1 (95% CI −0.9 to 1.1, p=0.83).
Characteristics of study groups
Results of the ABG needle study

Consort diagram.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
First pain score.
Patients in the 23G needle group experienced a significantly higher number of complications. 21.6% of patients in the 23G needle group experienced a complication in the form of a haematoma (n=11), tenderness (n=1) or paraesthesia (n=1) in comparison to 5.4% of patients in the 25G needle group (p=0.03, table 2). The number needed to treat was 6.6 to reduce one complication in the 23G needle group.
The success rate between 23G and 25G group was not significantly different (92.1 and 91.1%, respectively, with p=1.0). The 23G and 25G mean difficulty score was 3.4 (SD=2.6) and 4.3 (SD=2.4), respectively, with a mean difference of 0.9 (95% CI −0.03 to 1.7, p=0.06). There was also no significant difference between the difficulty score even if the needle used was not the operator's preferred size (p=0.921).
Discussion
The study showed there was no clinical difference in pain score experienced by emergency patient between the use of a 23G versus a 25G needle. There were no major complications noted during the study, although the minor complication rate was significantly higher than the 2–13% rate previously published in the limited literature6 ,7 The discrepancies between the literature complication rates and the study group rates may have been related to the differences in technique and site of procedure performed. Nevertheless, the most common complication reported was haematoma of the puncture site, and this was more prominent in the 23G needle group (17.5%).
We found that there was no significant difference in the difficulty score between needle groups and no significant difference in reported difficulty scores if operators did not use their preferred needle size. This suggests that the 23G and 25G needles can be interchanged and users can readily adapt to either.
Even though the randomisation was computer generated, there was a discrepancy noted between the 23G group of 63 patients and the 25G group of 56 patients. Contributing to this was the fact that five patients in the 25G study group and two in the 23G group were not included in the final analysis due to incomplete data. In the majority of cases, this was due to an incomplete pain or difficulty score.
Limitations
This was a single institution study conducted in one public hospital emergency department in the metropolitan area employing one particular brand and type of needle and thus might not be generalisable to all emergency departments. It is a proof-of-concept approach to the question of whether two different gauge needles would affect the pain experienced by patients undergoing an ABG analysis. The manufacturer use of colour coding for their needle size meant that this was only a single-blinded randomised control trial, which may have led to operator variability. Also, the data presented and predominantly analysed was the first pain and difficulty score due to the limited number of second and third attempts. There were assumptions made that patients were physically blinded, although this could not have been audited. Finally, while patients and operators were asked to draw a single line on the VAS for pain and difficulty, there were 50 patient forms and 58 operator forms where the number was circled instead. This may have implications regarding results analysis due to discrepancies with the methodology. Definitions were not provided regarding the meaning of complications, and therefore, the results regarding this aspect need to be interpreted with care. The use of local anaesthetic prior to arterial puncture, the possible alternative of venous blood gas sampling and the use of other size/length needles are beyond the scope of this study.
Acknowledgments
We thank the medical statistician Karen Blyth for her help in data analysis. We acknowledge the support of the medical and nursing staff of the emergency department at Westmead Hospital for undertaking of this study.
Footnotes
-
Contributors All authors formulated the study question and design. KY submitted study to ethics committee for approval and registration on the Australian New Zealand Clinical Trials Registry. KY made the consent/study packs used by patients and operators in the study. All authors were responsible for the supervision of the study. KY collated the data and performed the statistical analysis with Karen Byth (Hospital Biostatistician). All authors interpreted and wrote the paper.
-
Competing interests None.
-
Ethics approval South Western Area Health Services Human Research Ethics Committee (Westmead Hospital, Sydney Australia). Australia and New Zealand Clinical Trial Registry: ACTRN12609000957291.
-
Provenance and peer review Not commissioned; externally peer reviewed.