

Abstract
BACKGROUND: We investigated the prevalence of depression among patients with COPD treated in long-term in-patient rehabilitation facilities, using the Center for Epidemiologic Studies Depression scale (CES-D). Furthermore, the relationship between the severity of air-flow obstruction (the percent of predicted FEV1), BODE (body mass index, degree of air-flow obstruction, dyspnea, exercise capacity) index, health-related quality of life (St George's Respiratory Questionnaire [SGRQ]), and depression were investigated.
METHODS: We recruited 74 in-patients (64 males, 10 females) with COPD. The mean age of the subjects was 72.7 years (range 52–85 y). Subjects completed the CES-D, and measurements were made of pulmonary function, body mass index, Modified Medical Research Council dyspnea scale, 6-min walk test (6MWT), and SGRQ.
RESULTS: Depression was evident in 48.6% (n = 36) of the subjects. A weak correlation was found between the CES-D scores and the percent of predicted FEV1. The prevalence of depression showed a significant association with BODE stage. Scores for the SGRQ activity and impacts domains, and total SGRQ score were significantly worse in the subjects who were depressed.
CONCLUSIONS: We found a high prevalence of depression among patients with stable COPD treated in long-term in-patient rehabilitation facilities. Depression among these patients, as measured by the CES-D, was associated with greater impairment in respiratory function and with poorer Modified Medical Research Council dyspnea scale and SGRQ scores. The prevalence of depression increased with BODE stage.
Introduction
COPD is expected to become the 3rd leading cause of death in the world by 2020.1 In Japan, Fukuchi et al2 conducted a large-scale epidemiological study (Nippon COPD Epidemiology Study [NICE]) in 2001 and estimated the number of COPD patients in Japan at 5,300,000. These authors2 reported that the prevalence rate for adults age 40 years and above would reach 8.5%, making it a potentially serious medical issue in the future. COPD causes not only dyspnea on exertion but is also associated with poor nutrition and restriction in daily activities, due to muscle atrophy and decreased exercise capacity. This negative spiral is thought not only to result in poor physical function but also to have an adverse impact on psychological status, leading to a decrease in quality of life (QOL), and it is well documented that this spiral leads to anxiety and depression among many COPD patients.3–10 Furthermore, because the presence of depression may be associated with exacerbations of COPD and/or an increase in mortality,11–15 therapeutic interventions that target psychological impairments are considered necessary.
According to the Global Initiatives for Chronic Obstructive Lung Disease (GOLD),16 released in 2006 (www.goldcopd.com), pulmonary rehabilitation has a high level of evidence (level A) for decreasing anxiety and depression in people with COPD. Therefore, when patients undergo pulmonary rehabilitation, it is necessary to objectively evaluate not only physical status but also psychological well-being.
In studies we have previously conducted in both in-patients and out-patients with COPD, we have found that the prevalence of depression varies, depending on the evaluation criteria, and that the severity of lung function has an impact on the prevalence of depression when the symptoms of depression were evaluated using the Center for Epidemiologic Studies Depression scale (CES-D).17,18 In addition, we observed a correlation between depression in patients with COPD and personality traits such as a sense of inferiority, nervousness, introversion, excessive punctuality, and unsociability.19 The CES-D was developed by the National Institute of Mental Health for the purpose of epidemiologic studies on depression.18 Because both the reliability and validity of the CES-D have been verified,4 it is appropriate for use by healthcare providers. However, studies investigating the relationship between depression, as measured using the CES-D, physical function, and health-related QOL in in-patients with COPD have not been reported.
The objective of this study was to determine the prevalence of depression in in-patients with stable COPD, using the CES-D, as well as to identify whether or not depression is related to lung function, body mass index (BMI), dyspnea, exercise capacity, BODE (body mass index, air-flow obstruction, dyspnea, exercise capacity) stage, and health-related QOL, with the overall aim of providing information that will be helpful for the respiratory management of patients with COPD.
QUICK LOOK
Current knowledge
The pathophysiologic changes in lung function associated with COPD restrict daily activities and lead to a reduced quality of life and an increased incidence of anxiety and depression. The presence of depression is associated with a greater number of exacerbations and mortality in these patients.
What this paper contributes to our knowledge
Depression was present in nearly half of COPD patients treated in an in-patient long-term care facility. The correlation between depression scores and percent of predicted FEV1 was weak. The prevalence of depression was strongly associated with the BODE (body mass index, degree of air-flow obstruction, dyspnea, exercise capacity) index and the scores for the activity and impact domains of the St George's Respiratory Questionnaire.
Methods
Subjects
The subjects were 54 in-patients with COPD, who were admitted to a hospital that focuses mainly on providing pulmonary rehabilitation, and 20 patients with COPD in a long-term care facility who commenced pulmonary rehabilitation upon reaching a stable state one month after an exacerbation. Data were collected between November 2007 and November 2010. The inclusion criteria were a diagnosis of COPD according to the GOLD criteria, and stable physical status, as determined by the patient's physician.16 The average age of the subjects was 72.7 years (52–85 y), and 64 (86%) were male. The subjects were prescribed supplemental oxygen according to international guidelines. Individuals were excluded from participating in the study if they had decreased comprehension due to conditions such as dementia. This study was approved by the ethics committee of Nagasaki University Graduate School of Biomedical Science, and subjects gave written, informed consent.
Evaluation Items
The subjects were reviewed based on the following evaluation items:
Smoking history
Modified Medical Research Council (MMRC) dyspnea scale
BMI
Pulmonary function tests. Spirometry was performed in accordance with recommended guidelines.20 Results are expressed as a percentage of the predicted normal values, using data published by the Japanese Respiratory Society.21
6-min walk test (6MWT). Functional exercise capacity was measured using the 6MWT, in accordance with the protocol published by the American Thoracic Society.22
BODE index. The BODE index is a multidimensional grading system that comprises the BMI, degree of airway obstruction (the percent of predicted FEV1), dyspnea (MMRC), and exercise capacity (6-min walk distance), that was developed to predict the risk of death from any cause and from respiratory causes in people with COPD.23 Scores that range from 0 to 3 are assigned to the subject's % predicted FEV1, MMRC score, and 6-min walk distance. BMI is scored as 0 or 1 point, a BMI > 21 kg/m2 being assigned 0 points. The BODE index is the sum of points for each variable, and ranges from 0 to 10. Scores derived using the BODE index can be divided into 4 quartiles: quartile I is a score of 0–2; quartile II is a score of 3–4; quartile III is a score of 5–6; and quartile IV is a score of 7–10.
Evaluation of depression. We used the Japanese version of the CES-D, which is a self-complete questionnaire consisting of 20 items. Each item has a 4-point response choice that ranges from 0 to 3. A total score of 16 points or greater, out of 60 points, is considered to indicate the presence of depression.18
Evaluation of QOL. Health-related QOL was assessed using the Japanese version of the St George's Respiratory Questionnaire (SGRQ),24 which is a disease specific questionnaire. The SGRQ is a self-complete questionnaire with 76 items that provide scores for the 3 domains of symptoms, activity, and impacts, and also a total score. The scores are weighted for each domain, with lower scores indicating less impairment in health-related QOL.
Statistical Analyses
Relationships between CES-D scores and the severity of the percent of predicted FEV1 were assessed using the Spearman rank correlation coefficient. Subjects were grouped according to quartiles for BODE scores and the prevalence of depression, and each BODE stage was evaluated using the chi-square test. The Mann-Whitney U test was used to compare MMRC, BMI, lung function, 6-min walk distance, the individual SGRQ domains, and the total SGRQ score between subjects grouped according to the presence (CES-D score ≥ 16) or otherwise of depression. Statistical analyses were performed using statistical software (SPSS 16.0, SPSS, Chicago, Illinois). A probability (P) value of < .05 was regarded as significant.
Results
Characteristics of the Subjects
The Table shows the characteristics of the 74 subjects. The average score on the CES-D was 15.7 ± 9.2 points, with 36 subjects (48.6%) obtaining a score of at least 16 points. Among the 74 subjects, 46 subjects (62%) were receiving long-term domiciliary oxygen therapy (LTOT), of whom 27 subjects had depression, as determined using the CES-D score. The number of current smokers was 3 (depression group 1, non-depression group 2), former smokers 67 (depression group 32, non-depression group 35), and never smokers 4 (depression group 3, non-depression group 1). Subjects with depression had significantly higher dyspnea (MMRC score) than those without depression (P = .04). With regard to lung function, the depression group had lower FEV1 and FVC, with the difference in FVC reaching significance (P = .03). Sixty-nine (93%) subjects were able to complete the 6MWT. Six-minute walk distance was significantly lower in the group with depression (238 ± 102 m vs 335 ± 98 m [P = .001]). Fifty-eight (78%) subjects (24 in depression group and 34 in non-depression group) completed the SGRQ. The group with depression had significantly higher scores, indicating greater impairment, in the activity (P = .02) and impacts (P = .003) domains, and the total score (P = .004), compared to the non-depression group. No significant differences between groups were found in age, sex, or BMI.
Subject Characteristics (n = 74)
Relationship Between the Percent of Predicted FEV1, BODE Stage, and Depression
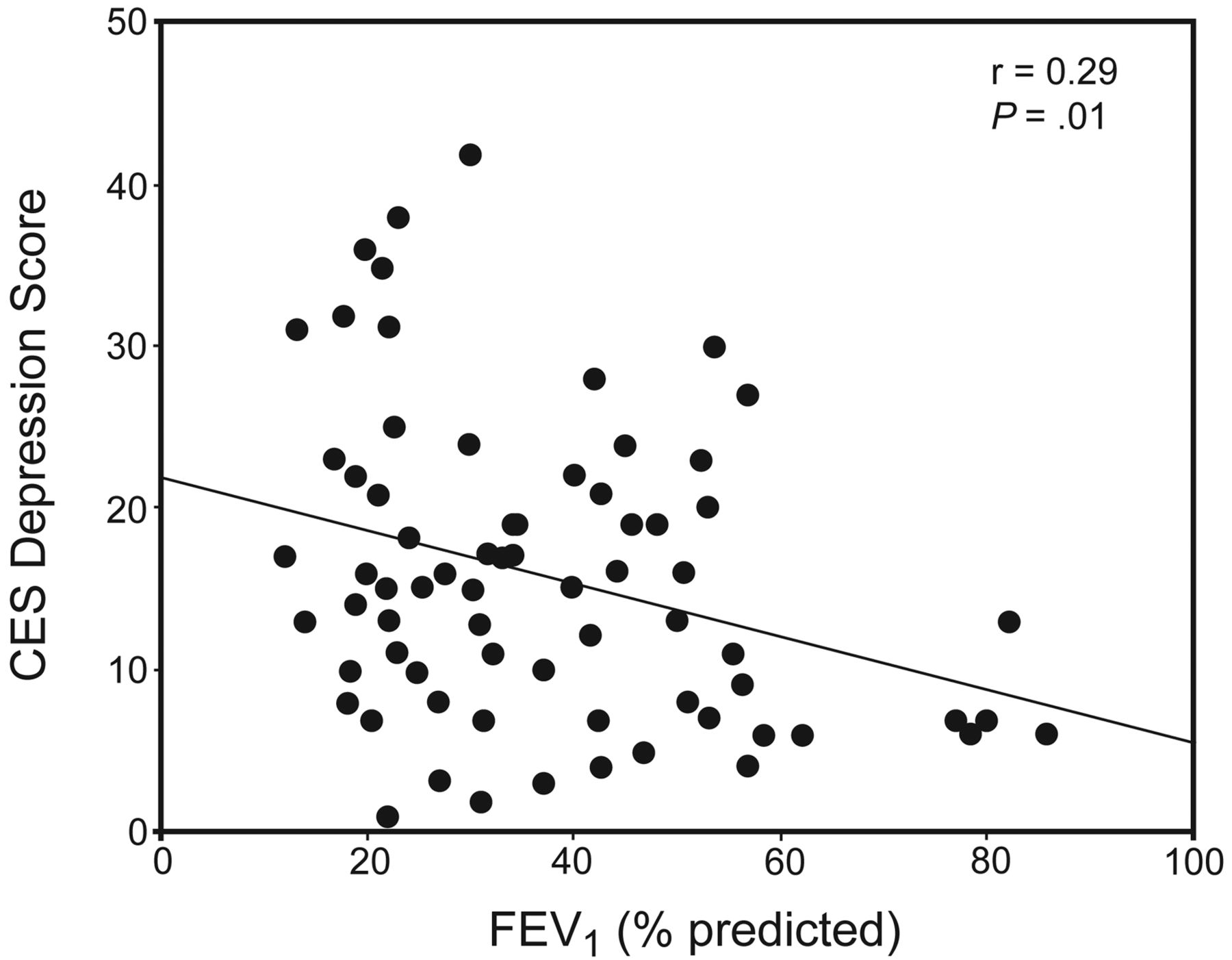
There was a weak correlation (r = −0.29, P = .01) between the severity of air-flow limitation (percent of predicted FEV1), and the CES-D score (Fig. 1). Figure 2 shows the prevalence of depression, with subjects grouped according to BODE stage. The prevalence of depression increased with BODE stage, being 12.5% (1/8) in stage I, 45.5% (5/11) in stage II, 38.2% (13/34) in stage III, and 75% (12/16) in stage IV (P = .02).

Relationship between depression and percent of predicted FEV1.
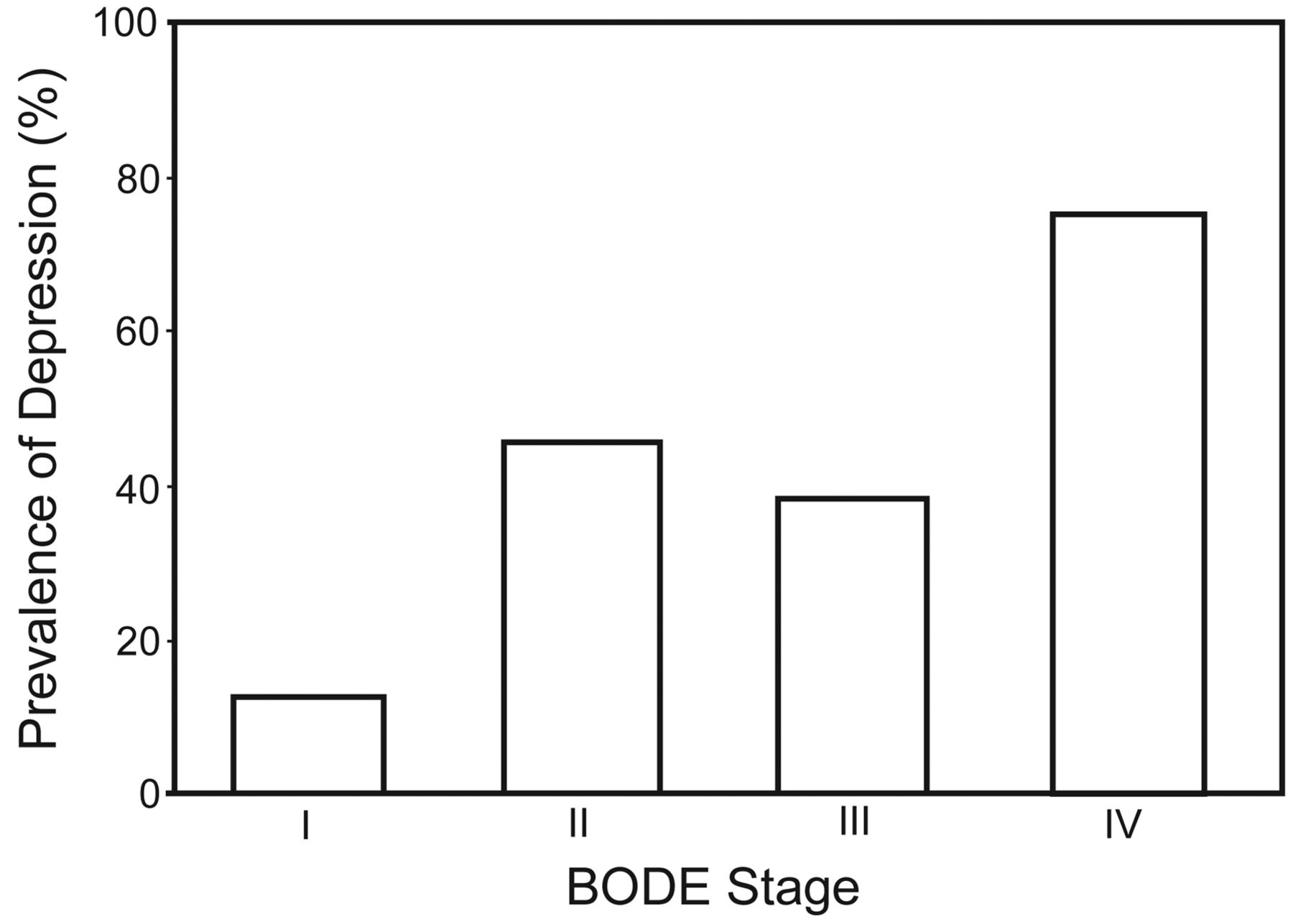
Prevalence of depression in patients with COPD classified according to the BODE (body mass index, degree of air-flow obstruction, dyspnea, exercise capacity) index stages.
Discussion
The objectives of this study were to describe the prevalence of depression in in-patients with stable COPD, to investigate the relationship between the severity of lung function impairment (the percent of predicted FEV1) and depression, to examine whether the prevalence of depression differed with scores for the BODE index, and to determine whether the presence of depression was associated with greater impairment in health-related QOL (SGRQ). While several methods exist for identifying the presence of depression, we used the CES-D; the reliability and validity of the questionnaire have been confirmed4,18 and it is easy to use.
The prevalence of depression was found to be 48.6%, affecting 36 of the 74 in-patients with COPD. According to previous studies, the prevalence of depression in patients with COPD has been reported to be higher, compared with a healthy population or people with conditions such as Parkinson disease.25–27 While many reports on the prevalence of depression in patients with COPD have been published,4–7,28 in the latest report pertaining to in-patients, Gudmundsson et al6 found depression in 29% of patients, while Ng et al28 reported a rate of 44%. Furthermore, based on reports on the prevalence of depression in Japan, Mishima et al observed a prevalence of 35% among out-patients with COPD who were receiving LTOT.9 Although our study showed a high prevalence of depression (48.6%), the reasons for this high rate may include the older age of the subjects (mean 72.7 years), the fact that our subjects were in-patients, and that a substantial proportion were receiving LTOT. Furthermore, Gudmundsson et al6 and Mishima et al9 used the Hospital Anxiety and Depression scale (HADS),29 which may account for the difference in prevalence rates. The CES-D and HADS instruments have been shown to estimate a different prevalence of depression within one COPD out-patient cohort.17 The prevalence of depression in COPD has ranged from 24% to 42% in international studies,7,12,30–32 and from 30% to 36% in previous studies from Japan.17,19
Although certain findings have not been obtained in previous studies on the relationship between the severity of lung function and depression in COPD patients, there have been reports indicating that there is no relationship between lung function and depression.6,9,25,33 Conversely, there are studies reporting that the severity of lung function affects depression.3,7,17,32,34 Van Manen et al7 assessed the prevalence of depression and related factors in 162 COPD patients, using the CES-D. They found the prevalence of depression to be 19.6% in patients with mild to moderate COPD, and 25.0% among patients with severe COPD,7 suggesting an association between the severity of lung function and depression. Dowson et al34 reviewed the prevalence of depression and anxiety, using the HADS, in 79 in-patients with COPD, and found that those with more severe impairment in lung function had higher scores of depression and anxiety. They acknowledged the association between COPD severity, depression and anxiety, indicating that disease severity affects the psychological status of patients and that improvement may be possible with interventions such as pulmonary rehabilitation.
Although our study showed that the lower the percent of predicted FEV1, the higher the prevalence of depression, the correlation was weak. However, according to the BODE index, our findings showed that the higher the BODE stage, the higher the prevalence of depression. In recent years, Funk et al,3 in a study of 122 in-patients with COPD, reported that the BODE index better reflects the prevalence of depression, as opposed to the GOLD classification, which is based on the severity of lung function. The results of the study by An et al35 provide support for this proposition. Our results are similar to those of Funk et al3 and show that not only lung function but also several other factors are related to depression in in-patients with COPD.
The effect of depression on the health-related QOL of patients with COPD is a serious problem. Using the SGRQ to assess health-related QOL, a significant correlation was found between the presence of depression and the domains of activity and impacts and the total score. With respect to the relationship between psychological status and QOL, Hajiro et al,33 in a study carried out in Japan, reported an association between depression evaluated by HADS and SGRQ. Furthermore, Lacasse et al8 also reported that there was a relationship between depression in out-patients with COPD, who were undergoing LTOT, and the Medical Outcomes Study Short-Form 36 questionnaire scores for most of the domains. Other reports, by Quint et al12 and Balcells et al,36 stated that the presence of depression seemed to decrease QOL when measured using the SGRQ, thus clearly indicating that depression is significantly related to QOL.
Quint et al12 also reported that patients with frequent exacerbations showed significantly higher average scores for depression than those without recurrent exacerbations, suggesting the importance of measures aimed at preventing exacerbations in people with COPD.
Although one previous study has reported that pulmonary rehabilitation has no impact on depression,37 most have shown that pulmonary rehabilitation decreases anxiety or depression.31,34,38,39 When implementing treatments, including pulmonary rehabilitation for COPD patients in the future, objective evaluation and understanding of psychological aspects such as depression, as well as physical function and QOL, will be major issues. Furthermore, because the relationship between patients with COPD with depression and their personality characteristics has been found in our previous study,19 taking personality traits into consideration may be helpful in understanding and providing care for COPD patients in the future.
It is difficult to compare this study population to COPD cohorts described elsewhere, in part due to international differences in healthcare delivery. Limitations of this study include: The subjects were not randomly selected; the sample size was relatively small; the majority were male, reflecting the gender difference in disease morbidity; and we made no assessment of social background. Therefore, studies taking these points into consideration are recommended.
Acknowledgments
We thank all the patients and staff members at each rehabilitation facility who kindly participated in our study. We also acknowledge the assistance of Dr Sue Jenkins, School of Physiotherapy, Curtin University of Technology, Perth, Western Australia, for proof-reading this paper.
Footnotes
- Correspondence: Hideaki Senjyu PhD, Course of Health Sciences, Graduate School of Biomedical Sciences, Nagasaki University. E-mail: senjyu{at}nagasaki-u.ac.jp.
This study was supported by a grant from the Environmental Restoration and Conservation Agency of Japan. The authors have disclosed no conflicts of interest.
- Copyright © 2013 by Daedalus Enterprises









{kind=link}
{kind=link}