Article Text

Abstract
Background: Although exercise training improves exercise tolerance in most patients with chronic obstructive pulmonary disease (COPD), some patients with severe disease may not be able to tolerate exercise training due to incapacitating breathlessness. Transcutaneous electrical muscle stimulation (TCEMS) has been shown to improve muscle strength, muscle mass, and performance in paraplegics, patients with knee ligament injury, and patients with peripheral vascular disease. We hypothesised that TCEMS of the lower extremities can improve muscle strength and exercise tolerance in patients with moderate to severe COPD.
Methods: A randomised controlled trial of TCEMS of the lower extremities was performed in 18 medically stable patients of mean (SD) age 60.0 (1.5) years with a mean forced expiratory volume in 1 second (FEV1) of 1.03 (0.10) l (38% predicted) and residual volume/total lung capacity (RV/TLC) of 59 (2)%. Stimulation of the lower extremities was performed three times a week, 20 minutes each session, for six continuous weeks. Quadriceps and hamstring muscle strength, exercise capacity, and peak oxygen uptake were measured at baseline and after 6 weeks of stimulation.
Results: TCEMS improved both the quadriceps strength (by 39.0 (20.4)% v 9.0 (8.1)%, p=0.046) and hamstring muscle strength (by 33.9 (13.0)% v 2.9 (4.7)%, p=0.038) in the treated (n=9) and sham treated (n=9) groups, respectively. The improvement in muscle strength carried over to better performance in the shuttle walk test in the treated group (36.1% v 1.6% in the treated and sham groups respectively, p=0.007, Mann-Whitney U test). There was no significant change in lung function, peak workload, or peak oxygen consumption in either group. Muscle stimulation was well tolerated by the patients with no dropouts and better than 95% compliance with the protocol.
Conclusions: TCEMS of peripheral muscles can be a useful adjunct to the comprehensive pulmonary rehabilitation of patients with COPD.
- chronic obstructive pulmonary disease
- exercise
- electrical muscle stimulation
Statistics from Altmetric.com
Poor exercise capacity is a common manifestation of chronic obstructive pulmonary disease (COPD). Central cardiopulmonary factors, respiratory muscle dysfunction, gas exchange abnormalities, and skeletal muscle dysfunction all play a role in limiting exercise capacity.1–3 Skeletal muscle dysfunction in COPD is thought to be secondary to hypoxaemia, inactivity leading to deconditioning and disuse atrophy, systemic inflammation, as well as nutritional and electrolyte disturbances.4 This skeletal muscle dysfunction manifests as reductions in fat free mass,5 oxidative enzyme capacity,6,7 and atrophy of type I and type IIa fibres.8
Exercise training is an important treatment modality for patients with COPD that can improve exercise endurance, aerobic fitness, and skeletal muscle oxidative capacity.9–11 However, some patients with severe COPD may have difficulty participating in exercise training (especially high intensity exercise) because of limited cardiopulmonary reserve. Abstinence from exercise often results in gradual deterioration in exercise capacity and muscle strength. Transcutaneous electrical muscle stimulation (TCEMS) is a method of augmenting muscle performance. This technique has been shown to increase the capillary/fibre ratio, the fibre cross sectional area, as well as muscle mass and the number of type I and type II fibres in humans.12 It has also been shown to improve oxidative potential of the muscle.13 Moreover, clinical trials in humans have shown that electrical stimulation improves muscle strength and performance in patients with major knee ligament injuries14,15 and those who are immobile after surgery,16 promotes muscle growth in paraplegic patients,17 and improves the performance of ischaemic muscles in patients with peripheral vascular disease.18
We hypothesised that TCEMS of the lower extremities would lead to an improvement in muscle strength and exercise performance in patients with severe COPD. This method may be particularly useful to improve the functional status of patients with severe cardiopulmonary limitation, arthritic joints, or acute exacerbation of COPD that may preclude participation in conventional exercise training programmes.
METHODS
Study design and subjects
A randomised controlled double blind study was conducted to examine the effects of TCEMS on muscle strength and exercise capacity in patients with moderate to severe COPD. The protocol was approved by the institutional human investigations committee. Informed consent was obtained from all patients prior to participation in the study.
Eighteen patients with moderate to severe COPD and poor exercise tolerance were recruited from Yale-New Haven Hospital and West Haven Veterans Administration Hospital chest clinics. Patients were included in the study if they had: (1) forced expiratory volume in 1 second (FEV1) <65% of predicted value with an FEV1 to forced vital capacity (FVC) ratio of <70%, hyperinflation based on residual volume/total lung capacity (RV/TLC) ratio >40%, and reduced lung transfer factor; (2) age <70 years; (3) self-reported exercise limitation despite pharmacological treatment; and (4) were otherwise medically stable. Patients with a history of cardiovascular and neuromuscular disease, active or debilitating joint disease, and formal pulmonary rehabilitation within 2 years of the date of inclusion into the study were excluded.
Physiological measurements:
Patients who met the above inclusion criteria underwent an initial training session to familiarise themselves with the exercise and measurement protocol and equipment. Following the initial day of familiarisation with the protocol, the following measurements were made at baseline and 6 weeks after lower extremity electrical muscle stimulation.
Quadriceps and hamstring maximal isokinetic strengths were measured in the seated position at an angular velocity of 60°/s using a Lido Multi Joint II isokinetic dynamometer (Lido Multi Joint II, Loredan Biomedical Inc, Davies, CA).19–22 Five duplicate leg extension and flexion measurements from a resting knee joint angle of 90° were made with adequate rest periods in between efforts. The best peak torque value in N.m unit was recorded. These measurements were made by one investigator who was blinded to the nature of intervention on all patients to minimise inter-observer variance.
Exercise tolerance was assessed using an incremental shuttle walking test (SWT) after completing a practice run on a separate day. The SWT measures the maximal distance walked by a patient at a pace set by audio signals from a cassette tape,23 Minute-by-minute walking speed is increased until the subject achieves exhaustion. In addition, a maximal symptom limited incremental cardiopulmonary exercise test was performed using a calibrated cycle ergometer (Monark, Monark-Crescent, Varberg, Germany) with a pedalling frequency of 40 revolutions per minute, during which the workload increased by 5–20 W increments every minute depending on subjects exercise capacity. The degree of perceived exertion was assessed using a Borg scale.24 Breathing rate, tidal volume, minute ventilation, and electrocardiography were measured continuously. Oxygen consumption and carbon dioxide production were calculated from the fractional concentrations of oxygen and carbon dioxide in the mixed expired gas using a SensorMedics metabolic system (SensorMedics Inc, Loma Linda, CA). Respiratory muscle strength, which included inspiratory (MIP) and expiratory (MEP) mouth pressures, were measured in triplicate using the method described by Black and Hyatt.25 All patients were instructed to use their inhaled bronchodilator within 2 hours of the evaluation appointments. These tests were carried out on three separate non-consecutive days to avoid the effect of fatigue on performance.
Transcutaneous electrical muscle stimulation
After the initial evaluation, patients were randomised into two groups. The active treatment group received TCEMS using an Omnistim FX-2 (Accelerated Care Plus, Sparks, NV) with two surface patch electrodes (8 × 6 cm) applied to each quadriceps, hamstring and calf muscles. The knee angle remained at 90° during simultaneous muscle stimulation to prevent joint movement. Electrical stimulation was performed for 20 minutes on each limb, 3 days/week for 6 continuous weeks on an outpatient basis. The stimulator generated brief bursts of electrical impulses at 50 Hz lasting 200 ms every 1500 ms. The muscles were stimulated by an asymmetrical square wave pulse with an initial intensity that was set to create a visible contraction ranging from 55 mA to 120 mA. The intensity increased weekly by approximately 5 mA. The initial and final mean intensities were 56.7 (1.7) and 95.0 (4.2) mA, respectively. The stimulation sequence pattern was based on electromyographic activation timing of the quadriceps and hamstrings for strength training according to the technique of Hallett et al.26
The control group had the same electrode, stimulator set up, and connection system with the unit on for identical time periods in the same setting but received no active electrical stimulation during the visits. Since patients did not know what, if any, sensations to expect during the electrical stimulation and were not in contact with each other, they remained blinded to the randomisation. Both the patients and all but one investigator were blinded to the type of treatment to eliminate the possibility of higher motivation and expectation in the treated subjects.
During the study period the patients continued to receive routine medical care from their primary physicians. No formal pulmonary rehabilitation programme was pursued by any of the patients during the study period.
Statistical analysis
Data are presented as mean (SE) values. The data were analysed using the unpaired Student’s t test or Mann-Whitney U test for anthropometric measurements and physiological parameters. The effect of stimulation on muscle strength and walking performance was analysed for between group differences using analysis of variance with the baseline value as a covariate. The sample size was based on assumptions of 80% power to detect an improvement of more than 20% in measured outcomes at a level of significance of p=0.05.
RESULTS
The baseline characteristics of the subjects reported in this study are shown in table 1.
Demographic and functional characteristics of study subjects
As a group, the patients had a moderate to severe degree of airflow obstruction with a mean FEV1 of 1.03 (0.10) l (38% predicted) and marked hyperinflation with RV/TLC of 59 (2)% and decreased transfer factor. The body mass index was within normal limits for both groups. There was no difference in baseline spirometry or respiratory muscle strength between the two groups (table 2).
Pulmonary function tests before and after transcutaneous electrical muscle stimulation
Effect of TCEMS on muscle performance
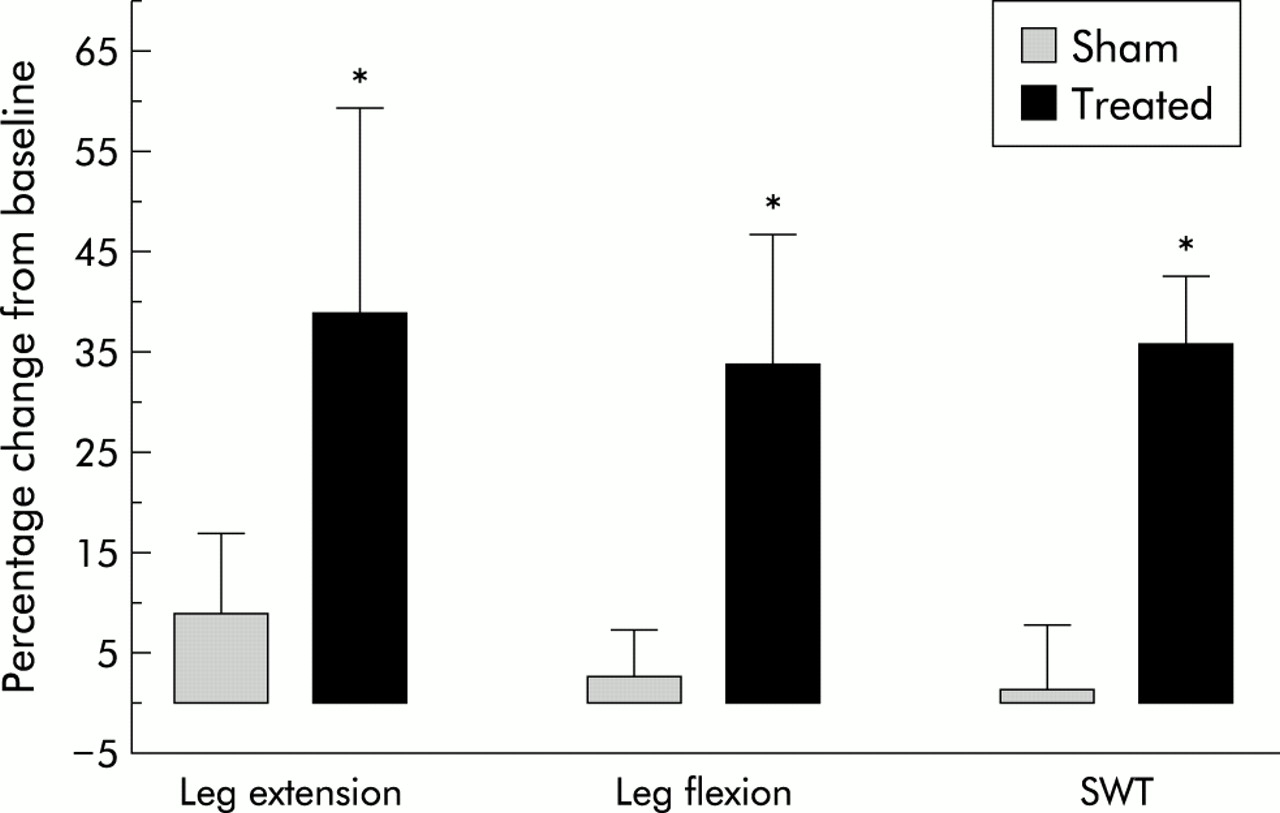
There were no significant differences between the groups in pulmonary function test data at baseline and after the treatment period (table 2). After 6 weeks of TCEMS of the lower extremities the maximum quadriceps strength improved significantly in the treatment group (from 44.7 (6.5) to 55.2 (6.6) N.m, p=0.004) but not in the control group (from 49.7 (5.5) to 53.6 (6.2) N.m, p=0.29) using the paired t test (table 3). Likewise, hamstring strength was also significantly improved in the treatment group (from 34.2 (4.2) to 43.6 (5.3) N.m, p=0.02) compared with the controls (from 38.1 (3.7) to 38.9 (3.9) N.m, p= 0.6). In addition, these data were analysed for between group differences using a two tailed Mann-Whitney U test and the percentage change from baseline for each strength measurement. The percentage changes were 39.0 (20.4)% in the treated group and 9.0 (8.1)% in the control group for leg extension (p=0.046), and 33.9 (13.0)% in the treated group and 2.9 (4.7)% in the control group for leg flexion (p=0.038, fig 1).
Muscle performance and exercise capacity in control and treated patients

{kind=link}
Percentage change from baseline values in maximal leg extension and flexion and walking distance (SWT, shuttle walking test) in treated and sham stimulated groups. *Leg extension, p=0.046; leg flexion, p=0.038; SWT, p=0.007.
Exercise capacity
A significant increase in the shuttle walking distance was observed in the treatment group with a mean improvement of 36.1% compared with 1.6% in the sham treated group (p=0.007, fig 1). This difference was also observed by analysing the actual data by employing analysis of variance with baseline performance on the SWT as covariate. All patients had low ventilatory reserve based on the ratio of peak minute volume over maximum minute ventilation (Ve/MVV) of 92 (6)% and 96 (6)% in the treated and control groups, respectively, during cardiopulmonary exercise testing. The subjects stopped cycling because of dyspnoea and/or leg fatigue. A small but statistically significant reduction in dead space (Vd/Vt) at peak exercise was noted in the treatment group (from 0.32 (0.024) to 0.30 (0.021), p=0.02) that was not observed in the control group (from 0.30 (0.015) to 0.30 (0.013), p=0.87). Similarly, there was a modest but significant improvement in the Borg scale of perceived exertion at a given level of exercise for each patient in the treatment group (from 12.7 (0.64) to 10.1 (0.90), p=0.01) but not in the control group (from 12.8 (0.88) to 12.6 (0.76), p=0.79). Only two of the 18 patients reached anaerobic threshold, as defined by RQ >1.0 and the inflection point of the minute ventilation curve during the cardiopulmonary exercise study. Overall, there was a trend towards improvement in oxygen consumption at peak exercise in the treatment group (from 867 (103) ml/min to 920 (114) ml/min, p=0.314) but not in the control group (from 954 (73) ml/min to 938 (76) ml/min, p=0.614). A similar pattern was observed in the peak workload achieved primarily in the treatment group (52.2 (7.3) W v 56.5 (6.1) W, p=0.34) compared with the control group (57.8 (4.2) W v 58.5 (4.7) W, p=0.84) as shown in table 3.
All the subjects completed the study. Compliance with the protocol was 95% in the treatment group and 97.5% in the control group. The stimulation was well tolerated. Five of the nine patients in the treatment group reported mild self-limited muscle cramps. Two patients in the control group complained of paraesthesia in their thighs while in the study. All of the 18 patients initially included in the study completed it. One patient in the treatment group was on a low dose of prednisone (5 mg daily).
DISCUSSION
Exercise training and pulmonary rehabilitation are integral parts of the medical management of patients with COPD. Upper and lower extremity exercise training is a major component of rehabilitation of these patients.10,11 These training exercises have been shown to improve the functional status of these patients.27–34 Greater improvements in cardiorespiratory fitness have been noted following high intensity training.30 However, some patients with severe ventilatory limitation may be unable to tolerate high intensity training, especially at the outset.9 Lack of tolerance may affect compliance with training, limit the incorporation of regular exercise into routine lifestyle, and, in turn, limit the benefits of the training programme. Moreover, reduced physical activity often leads to deconditioning and disuse muscle atrophy.
TCEMS is an alternative strategy that can improve muscle performance in humans independently of volitional exercise. Since submission of the present study, a report by Neder et al35 has shown that home based neuromuscular electrical stimulation in a group of patients with advanced COPD improved leg muscle strength and peak oxygen uptake. Fifteen patients with severe COPD (FEV1 38–39.5% predicted) underwent quadriceps femoris neuromuscular electrical stimulation 5 days a week for 6 weeks in a non-blinded fashion. Our findings are consistent with that study and show that, in patients with severe COPD, TCEMS of the lower extremities for a period of 6 weeks in the absence of concurrent active formal exercise training can significantly improve muscle strength and functional exercise capacity in the absence of changes in pulmonary function. However, there are some differences in the experimental design and the technique of neuromuscular stimulation. Our study was a randomised placebo controlled double blind trial to try to eliminate any potential confounders such as the influence of coaching during outcome measurements and self-motivation. Although our study showed a trend towards higher oxygen uptake in the treated group, it is difficult to explain a 20% increase in peak oxygen uptake during a maximal exercise on the basis of only quadriceps training in the aforementioned study. Despite the differences in the stimulation protocol between our study and that of Neder et al, the leg extension peak torque increased by a similar degree (39% and 42%, respectively) and the subjects were able to perform better during exercise. Although the patients in this study were not incapable of traditional exercise training, this study shows that TCEMS can lead to improved exercise tolerance in the absence of traditional endurance or strength training of skeletal muscle in patients with severe COPD. The technique may prove to be an ideal therapeutic modality for improving exercise capacity in patients with severe ventilatory limitation and/or chronic disabling joint disease who are unable or unwilling to undertake routine exercise training.
The findings of our study are comparable with previous reports on the use of low intensity peripheral muscle conditioning improving exercise tolerance.34,36 In the study by Simpson et al36 8 weeks of weightlifting exercises three times a week in a group of patients with moderate to severe COPD (FEV1 39.5% predicted) resulted in 44% and 16% improvements in knee extension and leg press, respectively, in the training group compared with 10% and –3% in the control group. There was a positive trend towards a treatment effect on the six minute walking test and a statistically significant improvement in endurance to fatigue during cycling at 80% of maximum exercise capacity in the trained group, with no change in the control group. Similarly, a 12 week low intensity repetitious exercise of the upper and lower extremities improved endurance of individual muscles but also increased the total work performed on the treadmill.34 These studies, like ours, show that low intensity muscle training can not only increase the strength of individual muscles, but also exercise tolerance and walking endurance. Our muscle conditioning protocol was similar but more intense than the one used by Simpson and co-workers which required 30 repetitions of knee extension and leg press during each triweekly session.36 Our TCEMS induced muscle contractions lasted 200 ms every 1.5 seconds for 20 minutes. This protocol increased both the strength and endurance of the muscle groups as reflected by knee extension and flexion force generation and distance covered during the walking test.
The mechanisms for the improvements seen in muscle strength and exercise tolerance resulting from TCEMS are not certain. However, TCEMS has been shown to increase the capillary/fibre ratio, fibre cross sectional area, muscle mass, and the number of type I and type II fibres in humans.12 The stimulation also enhances citrate synthase activity and oxidative capacity of the muscle as well as lactate transport.13,37
Two further points in this study need to be highlighted. Firstly, low to moderate conditioning of peripheral muscles is associated with improved exercise tolerance without an increase in maximum aerobic capacity. Secondly, we observed a small but statistically significant reduction in dead space ventilation and perceived exertion during exercise in the trained group but not in the controls. Although we have no plausible explanation for the increase in alveolar ventilation during exercise, the decrease in perceived exertion could potentially be on this basis. Clark and colleagues also observed a trend towards a decrease in dead space ventilation in their subjects with COPD who underwent peripheral muscle training.34
In summary, TCEMS improves muscle strength and exercise capacity during exercise in patients with severe COPD. It may be a useful component of pulmonary rehabilitation programmes, particularly in patients who have difficulty tolerating exercise training. Moreover, it may be a useful method for maintaining or improving the conditioning of peripheral muscles during acute exacerbations of COPD or any illness that may preclude regular exercise training in this population. Further studies are needed to examine the long term effect and the mechanisms by which electrical muscle stimulation improves exercise performance in patients with COPD.
Acknowledgments
This study was supported in part by the departmental fund, Yale Section of Pulmonary and Critical Care.