Article Text

Abstract
Background: A reduction in expiratory muscle (ExM) endurance in patients with chronic obstructive pulmonary disease (COPD) may have clinically relevant implications. This study was carried out to evaluate ExM endurance in patients with COPD.
Methods: Twenty three patients with COPD (FEV1 35 (14)% predicted) and 14 matched controls were studied. ExM endurance was assessed using a method based on the use of an expiratory threshold valve which includes two steps. In step 1 the load is progressively increased (50 g every 2 minutes) until task failure is reached, and the pressure generated against the highest tolerated load is defined as the maximal expiratory sustainable pressure (Pthmax). In step 2 subjects breathe against a submaximal constant load (80% of Pthmax) and the time elapsed until task failure is termed the expiratory endurance time (Tth80). In addition, the strength of peripheral muscles (handgrip, HGS) and respiratory muscles (maximal inspiratory and expiratory pressures, Pimax and Pemax, respectively) was evaluated.
Results: Patients with COPD had lower ExM strength and endurance than controls: Pemax 64 (19)% predicted v 84 (14)% predicted (mean difference 20%; 95% confidence intervals (CI) 14 to 39); Pthmax 52 (27) v 151 (46) cm H2O (mean difference 99, 95% CI 74 to 123); and Tth80 9.4 (6.3) v 14.2 (7.4) min (mean difference 4.8, 95% CI 1.0 to 10.4; p<0.01 for all). Interestingly, ExM endurance directly correlated with both the severity of airways obstruction (Pthmax with FEV1, r=0.794, p<0.01) and the reduction in strength observed in different muscle groups (Pthmax with HG, Pimax or Pemax, r=0.550, p<0.05; r=0.583, p<0.001; and r=0.584, p<0.001, respectively).
Conclusions: ExM endurance is decreased in patients with COPD. This impairment is proportional to the severity of the disease and is associated with lower strength in different muscle groups. This suggests that systemic effects are implicated in the impairment observed in ExM function.
- expiratory muscles
- endurance
- chronic obstructive pulmonary disease
- threshold loading
- Pimaxrv, maximal inspiratory pressure
- Pemaxtlc, maximal expiratory pressure
- Pthmax, maximal expiratory sustainable pressure
- Tth80, expiratory endurance time
- HGS, hand grip dynamometry
Statistics from Altmetric.com
- Pimaxrv, maximal inspiratory pressure
- Pemaxtlc, maximal expiratory pressure
- Pthmax, maximal expiratory sustainable pressure
- Tth80, expiratory endurance time
- HGS, hand grip dynamometry
Abdominal muscles (external oblique, internal oblique, rectus and transverse) are considered the main expiratory muscles (ExM). Their contraction compresses the abdominal content, causes the costal ribs to descend, and pushes the diaphragm towards the thorax. Along with the action of the internal intercostal muscles, abdominal muscles increase intrathoracic pressure, diminishing lung volume and facilitating expiratory flow.1 Moreover, the activity of ExM increases in proportion to ventilatory demands.2 ExM contraction also drives the execution of different expulsive efforts such as coughing.
ExM recruitment has been observed in patients with either chronic obstructive pulmonary disease (COPD) or asthma.3–,5 Although the clinical significance of this activation is unclear, ExM contraction is considered to be a mechanism that provides the system with functional reserve.1,2,5 However, it is well known that the function of different muscle groups can be impaired in patients with COPD.6 Although hyperinflation could explain the impairment observed in inspiratory muscles, other factors are more probably implicated in the deterioration reported in the strength of other muscle groups such as ExM or peripheral muscles. We believe that similar mechanisms would also lead to a reduction in ExM endurance in COPD. There is a rationale for hypothesising that this impairment would have clinically relevant implications. However, only a few attempts have been made to assess ExM endurance.2,7–,9 The current methods used for this purpose have been to breathe against resistive loading or to perform repeated maximal efforts until exhaustion. However, these techniques have important limitations. The present study was carried out to evaluate ExM endurance in patients with COPD using incremental as well as constant submaximal threshold loading.10,11
METHODS
Study population
Thirty seven sedentary men aged 61 (13) years were included in the study, 23 in the COPD group and 14 age and weight matched control subjects with normal lung function. The diagnosis of COPD was based on the patients' smoking history and spirometric testing showing non-reversible airways obstruction (FEV1/FVC <70%, FEV1 <80% predicted, and a lack of response to bronchodilators).12 Controls were recruited from the general population who visited the hospital for routine visual examination and all were non-smokers (present and past). Individuals with malnutrition, alcoholism (<80 g/day), neuromuscular or metabolic diseases, patients receiving chronic treatment with systemic steroids, systemic β agonists, calcium blocking agents or diuretics, and those undergoing rehabilitation programmes were excluded. The study was approved by the Research Committee on Human Investigation at our centre and informed written consent was obtained from each participant after full explanation of the purposes and characteristics of the study.
Pulmonary function tests and peripheral muscle strength
Spirometric parameters and measurements of static lung volumes and airways resistance were carried out on all subjects (Vmax, Sensormedics, CA, USA). Lung function variables are expressed in absolute values and as a percentage of the predicted normal values.13–,15 Blood samples were obtained from the radial artery of the non-dominant arm and blood gas tensions were measured by conventional polarographic techniques (ABL 330; Radiometer, Copenhagen, Denmark). Peripheral muscle strength was assessed using a handgrip dynamometer (HGS) (BIOPAC Systems Inc, Santa Barbara, CA, USA). After familiarising themselves with the test, subjects performed repeated attempts with both hands. The best of three consecutive manoeuvres was selected in each case.
Respiratory muscle strength
This was assessed at the mouth by measuring maximal respiratory pressures generated during forced inspiratory (Pimax) and expiratory (Pemax) efforts performed against an occluded airway. The mouthpiece used in the manoeuvres (Sibelmed, SIBEL, Barcelona, Spain) had a small orifice to minimise the participation of face and mouth muscles.16 For the measurement of Pimax the maximal inspiratory effort was performed at two different lung volumes: close to residual volume (Pimaxrv) and functional residual capacity (Pimaxfrc). To determine Pemax, maximal expiratory efforts were performed close to both total lung capacity (Pemaxtlc) and functional residual capacity (Pemaxfrc). Reference values were those published by Wilson et al.17
Study of expiratory muscle endurance
This was assessed using a technique recently described by our group. Briefly, the test consists of breathing against loads applied to an expiratory threshold valve and is divided into two parts. Subjects first breathe against incremental expiratory loads of 50 g every 2 minutes until the maximal expiratory sustainable pressure (Pthmax, defined as the maximal threshold pressure that can be tolerated for at least 60 seconds) is reached. The subjects then breathe against a constant expiratory submaximal load equivalent to 80% Pthmax and the time elapsed to task failure is defined as the expiratory endurance time (Tth80, expressed in minutes). The mechanics of the valve as well as technical characteristics of the test—such as reproducibility, oxygen uptake, and learning effects—have been explained in detail in previous papers.10,11
In the present study both parts of the test were carried out at least 30 minutes apart and the test ended when the subject was unable to open the valve in five serial and fully stimulated expiratory efforts. Dyspnoea was evaluated using the Börg scale. The following parameters were recorded (Biopac Recorder, Biopac Systems) throughout the test: mouth pressure (1050 BP transducer, Biopac Systems), electromyography (EMG) of the abdominal muscles using surface electrodes, airflow (TSD 117 Pneumotachometer, Biopac Systems), chest and abdominal movements (TSD 101 Respiration Transducer, Biopac Systems), oxyhaemoglobin saturation (BIOX 3740 Pulse Oximeter, Ohmeda, Louisville, CO), and electrocardiographic signal (Hollige, Servomed SMK, Würzburg, Germany). In addition, blood pressure was measured every 2 minutes using an automatic arm sphygmomanometer and Pemaxfrc, Pimaxfrc and inspiratory capacity (IC) were all measured at baseline and immediately after task failure. The ExM pressure-time index (PTExM) was calculated according to the equation: where Pth is the threshold pressure in each step, Te the expiratory time, and Ttot the total respiratory time.
where Pth is the threshold pressure in each step, Te the expiratory time, and Ttot the total respiratory time.
Statistical analysis
Results are expressed as mean (SD). Differences between COPD patients and controls were assessed using the non-parametric Mann-Whitney U test, while the association between continuous variables was evaluated using the Spearman coefficient. Differences between COPD and control groups are expressed as the mean with 95% confidence intervals (95% CI). A p value of ≤0.05 was considered significant.
RESULTS
The main general and pulmonary function data are shown in table 1⇓. Both groups had similar age and anthropometric parameters, but the patients with COPD had a mean (SD) FEV1 of 35 (14)% predicted (range 15–69) and 16 of them showed air trapping (residual volume >120% predicted).
General and lung function data
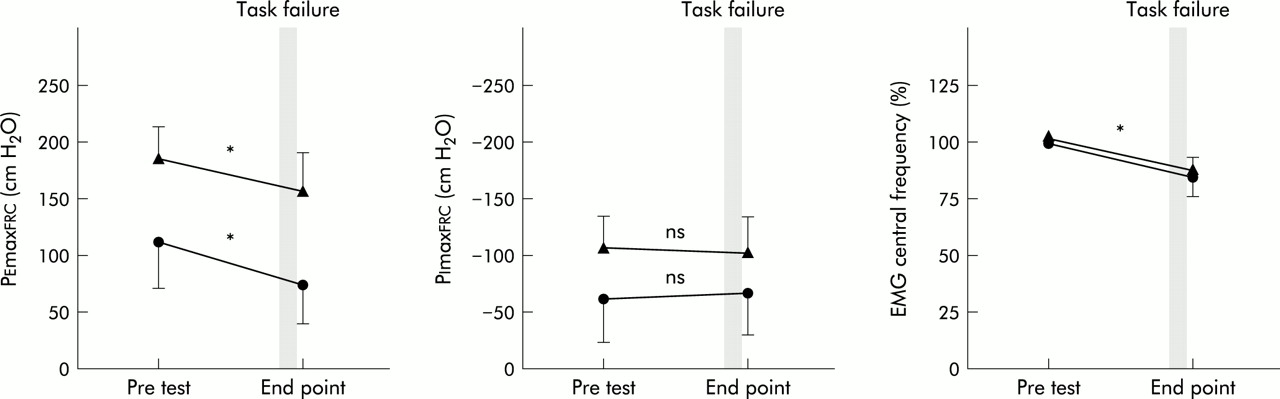
The presence of COPD was associated with a global decrease in muscle strength (table 2⇓) as shown by the lower values observed in HGS, Pimax, and Pemax. Patients with COPD also had lower values for both Pthmax and Tth80 (table 2⇓), although the impairment was higher for Pthmax (66% v 34%). Both patients with COPD and control subjects complained of extreme dyspnoea at the end point of both parts of the test, but no other complications were observed. In addition, patients with COPD had a PTExM of 0.18 (0.09) compared with 0.38 (0.12) in control subjects (p<0.05, mean difference 0.20, 95% CI 0.13 to 0.24) with a decrease of 17 (2)% in EMG centroid frequency compared with 15 (3)% in controls (mean difference 2, 95% CI 0.3 to 3.6) at the end point of the progressive loading test. Pemaxfrc obtained immediately after task failure was lower than the baseline value in both groups (72 (27) v 120 (38) cm H2O for patients with COPD and 160 (18) v 182 (16) cm H2O in controls, mean difference in the changes 26, 95% CI 11 to 30, p<0.001 for both), while no changes were observed in either IC or Pimaxfrc (fig 1⇓). With reference to the breathing pattern, an increase was observed in respiratory ratio (RR) in both groups but Te/Ttot remained stable in patients with COPD. On the other hand, the patients had a progressive increase in heart rate (from 85 (12) to 118 (19) bpm, p<0.05) but no changes were observed in either blood pressure or oxygen saturation. Interestingly, the Pthmax/Pemax ratio was found to be lower in patients with COPD (table 2⇓).
Respiratory and peripheral muscle function

Changes in maximal expiratory and inspiratory pressures (Pemaxfrc and Pimaxfrc, respectively) and electromyographic centroid frequency and their relationships with task failure during progressive expiratory loading. Patients with COPD are represented by circles and control subjects by triangles. *p<0.001.
Task failure occurred at PTExM of 0.16 (0.08) in patients with COPD and at 0.32 (0.06) in controls (p<0.001, difference 0.16, 95% CI 0.10 to 0.23) in the constant loading test. At that moment, EMG showed a 15 (2)% decrease in centroid frequency and Pemaxfrc was also reduced, with no changes in either Pimaxfrc or IC. Changes in all these parameters were very similar to those observed in controls.
The severity of the disease, assessed by the degree of airways obstruction, directly correlated with muscle function in all the muscle groups tested. When focusing attention solely on ExM, a direct relationship was observed between FEV1 and Pemax (r=0.546, p<0.01 for the overall population; not significant for COPD only), Pthmax (r=0.794, p<0.01 for the overall group; r=0.454, p<0.05 for COPD only) and Tth80 (r=0.370, p=0.05 for the overall group; not significant for COPD only; fig 2A and B⇓). No correlations were found between Pao2 and the ExM endurance variables. On the other hand, Tth80 correlated with Pthmax (r=0.474, p<0.01 for the overall group; not significant for COPD only; fig 2C⇓), and each one of these endurance variables in turn correlated with the strength of expiratory, inspiratory, and peripheral muscles: Pthmax with Pemax (r=0.584, p<0.001), Pimax (r=0.583, p<0.001), and HG (non-dominant, r=0.550, p<0.05), and Tth80 with Pemax (r=0.504, p<0.01), Pimax (r=0.440, p<0.05), and HG (non-dominant, r=0.510, p<0.05).

{kind=link}
{kind=link}
Relationships between airways obstruction (FEV1) and expiratory muscle endurance in the face of (A) incremental (maximal sustainable threshold pressure or Pthmax) and (B) constant expiratory loading (endurance time or Tth80). (C) Relationship between Pthmax and Tth80. Patients with COPD are represented by circles and control subjects by triangles.
DISCUSSION
This study shows that ExM endurance is impaired in patients with COPD and that this impairment is proportional to the severity of the disease. In addition, deterioration in ExM endurance is associated with parallel impairments not only in the strength of this muscle group but also of other muscle groups. The latter finding suggests that there are systemic effects on skeletal muscles in COPD.
ExM contraction results in an increase in intrathoracic pressure, allowing expiratory airflow to increase in normal subjects. In addition, ExM also participate in other functional situations such as those related to movements or fixation of the trunk.1 However, there is a surprising paucity of data related to ExM function in COPD. Although these muscles have been found to be recruited in such patients both at rest and during loaded breathing, the significance of this activation has not been well defined.1,3,5 However, several studies have focused on this point. Two studies18,19 have shown that ExM are progressively recruited when brochospasm is experimentally induced, and another study20 found an increase in ExM activity when patients with COPD were submitted to expiratory resistances, probably due to the necessity of increasing airflow. Other studies have shown that patients with COPD recruited ExM at the end of expiration.3,4,21 This would result in a passive onset of the next inspiration caused by the release of chest elastic recoil. In addition, ExM activity also appears to be present when there is an increase in inspiratory pressure.22,23
In summary, all these reports clearly indicate that ExM are recruited in patients with COPD under different circumstances. There is therefore a rationale for hypothesising that the impairment in ExM function is more than likely to have relevant clinical implications. However, functional evaluation of ExM is currently limited to assessing solely their strength through the measurement of maximal pressures. This would certainly be useful for evaluating some of their roles, such as those related to the efficiency of isolated cough efforts. However, this approach appears to be incomplete for predicting other ExM functions such as their tolerance to increased loads or persistent coughing. These circumstances are present in patients with COPD and can even be increased during exacerbations or exercise.
Although there are several reports showing that ExM strength can be impaired in COPD,24–,27 it is still unclear whether or not this is associated with an impairment in their endurance, and under which circumstances this may occur. This study shows that the endurance of ExM is significantly decreased in patients with COPD. Several factors could be involved in this impairment; some are local, such as alterations in the mechanics of their contraction, and others are systemic.
The possibility that the mechanics of ExM contraction are chronically impaired in COPD due to changes in the geometry of the thorax or abdomen is unlikely. In fact, the increase in lung volumes would passively lengthen these muscles, bringing them even closer to their optimal length-tension point.28–,30 One possible explanation for the endurance limitation observed in COPD is that this was related to the decrease in the ExM capacity for generating force. However, this is improbable since maximal sustainable pressure was only half of the maximal force (Pemax). In addition, if the decrease in ExM endurance were to be simply attributed to force limitation, the last increase in the load would have been immediately followed by task failure in the incremental loading test.31 The cessation of the task, however, always occurred 25–100 seconds after the imposition of the final load.
Another point when considering possible causes of impairment of ExM endurance in COPD is the analysis of those factors involved in ExM task failure within the test itself. Since the patients' inability to continue breathing against loads was associated with a decrease in Pemaxfrc and EMG centroid frequency, as well as a dramatic increase in PTExM values, we can assume that failure was mainly due to ExM muscle fatigue.32,33
An alternative explanation is that inspiratory rather than expiratory muscles became fatigued as a consequence of dynamic air trapping. However, no changes were observed in IC or Pimaxfrc at the end of the test.34 Another possibility is that task failure was related to neuropsychological factors. In fact, all the patients reported maximal dyspnoea at the end of the test. Nevertheless, this was not the main cause of cessation since, at this stage, all of them performed at least five unsuccessful expiratory efforts. On the other hand, to avoid bias due to different degrees of motivation, a well trained technician was assigned to encourage subjects throughout the test. Finally, regarding a potential learning effect, several precautions were taken. On the one hand, we used the same approach proposed by Martyn et al18 and Eastwood et al35 who argued that the progressive increase in loads would abolish potential bias due to learning. In addition, in a previous study we demonstrated that performing the endurance protocol on more than two occasions had a negligible effect on the outcome variables.11 Finally, the use of a control group minimised the effects of learning as a confounding factor. We feel that, if present, neuropsychological factors were secondary in explaining both ExM task failure and the differences between COPD patients and controls.
The second relevant finding in this study is that impairment in ExM endurance was associated with a parallel decrease in muscle strength. This was observed not only for ExM, but also for other muscle groups, reinforcing the notion that a factor(s) with systemic effects is present in COPD, playing a relevant role in their skeletal muscle dysfunction. However, the relevance of factors such as malnutrition, drugs, severe gas exchange abnormalities, or general deconditioning is unlikely in our study since patients were carefully selected, excluding these conditions. Nevertheless, other factors such as inflammation or redox imbalance36 could have been present. Whatever the driving factor may be, we have recently observed that there is a marked reduction in fibre size and a mild decrease in the proportion of type II fibres in the external oblique muscle in patients with severe COPD.37 These findings could be the cellular basis for the impairment observed in ExM function.
The method used in this study emulates the endurance tests introduced two decades ago for the study of inspiratory muscles18,35,38 and has been proved to be safe and reproducible in healthy subjects.11 We propose evaluating ExM endurance through two variables (Pthmax and Tth80) which would represent complementary aspects of this functional attribute. The Pthmax would assess ExM endurance in the face of incremental loading, with all the advantages of incremental tests, whereas Tth80 would represent a time-dependent effort against a constant submaximal load.9,39 Previous authors2,7 have used either repeated maximal expiratory efforts or breathing against resistive loading to evaluate ExM endurance. However, these methods have important disadvantages since a high degree of motivation is required to achieve the target pressure in the former, breathing pattern must be strictly controlled in the latter, and both dramatically limit the possibility of assessing individual ventilatory strategy when facing loads. To avoid these limitations, Suzuki et al8,9 used a threshold valve. However, they limited the assessment to the measurement of the endurance time breathing against constant submaximal loads. We feel that the two step method used in our study provides more complete information.
In summary, we have shown that endurance of the ExM is decreased in COPD. This impairment is related to the severity of airflow obstruction and is associated with a decrease in the strength of different muscle groups.
Acknowledgments
The authors thank Dr Alexander Grassino, Dr Lars Lindstrom, and Dr Pawel Sliwinski for their valuable suggestions and Joseph A Salazar and Dr Marta Pulido for editing the manuscript and editorial assistance.
REFERENCES
Footnotes
Antoni Ferrer was a Senior Researcher from the Consorci Hospitalari Parc Tauli, Sabadell. His stage of the study was funded by grant BAE-FIS (Spain).