Article Text

Abstract
Background In mild asthma exercise-induced bronchoconstriction (EIB) is usually treated with inhaled short-acting β2 agonists (SABAs) on demand.
Objective The hypothesis was that a combination of budesonide and formoterol on demand diminishes EIB equally to regular inhalation of budesonide and is more effective than terbutaline inhaled on demand.
Methods Sixty-six patients with asthma (>12 years of age) with verified EIB were randomised to terbutaline (0.5 mg) on demand, regular budesonide (400 μg) and terbutaline (0.5 mg) on demand, or a combination of budesonide (200 μg) + formoterol (6 μg) on demand in a 6-week, double-blind, parallel-group study (ClinicalTrials.gov identifier: NCT00989833). The patients were instructed to perform three to four working sessions per week. The main outcome was EIB 24 h after the last dosing of study medication.
Results After 6 weeks of treatment with regular budesonide or budesonide+formoterol on demand the maximum post-exercise forced expiratory volume in 1 s fall, 24 h after the last medication, was 6.6% (mean; 95% CI −10.3 to −3.0) and 5.4% (−8.9 to −1.8) smaller, respectively. This effect was superior to inhalation of terbutaline on demand (+1.5%; −2.1 to +5.1). The total budesonide dose was approximately 2.5 times lower in the budesonide+formoterol group than in the regular budesonide group. The need for extra medication was similar in the three groups.
Conclusions The combination of budesonide and formoterol on demand improves asthma control by reducing EIB in the same order of magnitude as regular budesonide treatment despite a substantially lower total steroid dose. Both these treatments were superior to terbutaline on demand, which did not alter the bronchial response to exercise. The results question the recommendation of prescribing SABAs as the only treatment for EIB in mild asthma.
- Asthma
- Exercise
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Key messages
What is the key question?
-
Does on-demand treatment with the combination of budesonide/formoterol improve asthma control as assessed by exercise induced bronchoconstriction (EIB)?
What is the bottom line?
-
The combination of an inhaled corticosteroid (ICS) and a long-acting β2 agonist (LABA) on demand yields better asthma control than a short-acting β2 agonist (SABA) on demand and is non-inferior to regular ICS treatment.
Why read on?
-
Current recommendations of treating EIB with a SABA on demand as the only medication in patients with mild asthma does not improve bronchial response to exercise over time and could therefore be questioned. On-demand treatment with an ICS/LABA combination improves asthma control and should be considered as an alternative in patients who otherwise would be treated with regular ICS.
Introduction
Exercise-induced bronchoconstriction (EIB) is a common feature in asthma1 and exercise-induced symptoms constitute a substantial impact on daily life.2 Asthma medications reduce exercise-induced symptoms and improve physical fitness3 but, despite treatment being given according to current guidelines,1 many patients with asthma experience symptoms in connection with physical exercise.
In current recommendations short-acting inhaled β2 agonists (SABAs) are advocated for patients who experience EIB despite otherwise controlled asthma and in patients in whom exercise is the only trigger for asthma symptoms.1 In patients with insufficient disease control, despite inhaling β2 agonists prior to exercise, the addition of controller medications, inhaled glucocorticosteroids or antileukotrienes is recommended.1 In real-life practice it may be difficult to determine when controller medication should be introduced.
Inhalation of β agonists, prior to exercise or when EIB has occurred, reduces or even abolishes EIB.4 During continuous treatment the protective effect of β2 agonists against EIB diminishes with time and does not offer the same protection after a few weeks of treatment as after the first dose.5 ,6 Tachyphylaxis with regard to the protective effect of β2 agonists has been demonstrated for bronchoconstriction induced by methacholine,5 adenosine,6 exercise7 ,8 and allergen.9
The aim of this study was to evaluate the effect of three different treatment regimens on asthma control by the response to exercise not preceded by bronchodilator treatment. The aim was thus not to study the direct effect of treatment on EIB. Currently recommended treatment, that is, SABAs inhaled on demand (ie, before training and for symptom relief) was compared with regular treatment with an inhaled glucocorticosteroid and a β2 agonist on demand and a fixed combination of an inhaled glucocorticosteroid and a rapid long-acting β2 agonist (LABA) inhaled only on demand. We hypothesised that the fixed combination on demand provides better asthma control than monotherapy with a β2 agonist on demand and is non-inferior to regular treatment with an inhaled glucocorticosteroid with a β2 agonist on demand.
Material and methods
Study design
In a randomised, double-blind, double dummy, parallel-group, 6-week trial the protective effect of three treatment regimens on EIB was investigated in adults and adolescents with mild asthma. The treatment alternatives were as follows:
-
regular placebo once daily and a fixed combination of 200 μg budesonide and 6.0 μg formoterol metered dose (Symbicort, AstraZeneca AB, Sweden) on demand;
-
regular placebo once daily and 500 μg terbutaline metered dose (Bricanyl, AstraZeneca AB) on demand;
-
regular inhalation of 400 μg budesonide metered dose (Pulmicort, AstraZeneca AB) once daily and 500 μg terbutaline metered dose (Bricanyl, AstraZeneca AB) on demand.
On demand means inhalation of study drugs before exercise and for symptom relief at any time. The participating subjects were instructed to perform physical exercise three to four times a week during the 6-week treatment period.
The trial was conducted at 10 study sites in Sweden and Norway. All study subjects attended two screening visits prior to randomisation.
At the first visit a standard skin prick test, spirometry, physical examination, vital signs control, demography, control of medical history and concomitant medication were conducted and the Asthma Control Questionnaire 5 (ACQ5) was completed. Eligible subjects underwent a maximal exercise test on a treadmill.
At the second visit a 6 min standardised exercise test was performed on a treadmill at 90% of maximal aerobic capacity, while breathing dry air.10 If post-exercise forced expiratory volume in 1 s (FEV1) was reduced by ≥10% compared with the pre-exercise value, the patient was included.
At the third visit the patients were randomised to one of the three treatment regimens. Three weeks and 6 weeks after randomisation an exercise test, identical to visit 2, was performed (figure 1).

Study design.
Subjects
Eligible subjects were outpatients ≥12 years of age with mild asthma,1 a history of EIB and who used reliever medication for asthma symptoms up to four times per week with a FEV1 >80% of predicted normal value11 ,12 and who performed physical exercise on a regular basis (at least three times per week). Smokers and ex-smokers who quit during the last year were excluded. Other exclusion criteria were indication for treatment with anti-inflammatory asthma medications (investigator’s judgment), use of oral corticosteroids during the month prior to the study and significant diseases other than asthma.
All patients provided written informed consent. The study was approved by the Ethics Committee of Stockholm (D5890L00032) and the Regional Ethics Committee of Health Region South East of Norway. The study is registered at ClinicalTrials.gov (identifier NCT00989833).
Spirometry
Pulmonary function was measured according to the European Respiratory Society/American Thoracic Society guidelines.13 The spirometers were calibrated on a daily basis. If FEV1 was between 75% and 80% of predicted value the spirometry was repeated 15 min after inhalation of 0.4 mg of salbutamol. If salbutamol induced an increase of FEV1<12% of the preinhalation value and <200 mL, the patient proceeded to the maximal exercise test.
Skin prick test
A skin prick test with 10 common allergens (ALK Abello Soluprick SQ allergen solution, Copenhagen, Denmark) was performed with histamine (10 mg/mL) as a positive and the diluent as a negative control. Positive response was specified as a wheel ≥3 mm.
Maximal exercise test
A maximal exercise test was performed on a treadmill while breathing ambient air according to a predefined protocol starting at 50 W, which was then increased by 10 or 15 W (depending on body weight) every minute. Heart rate was monitored by ECG and registered during the last 15 s of each workload level. Dyspnoea and leg fatigue were registered according to the Borg CentiMax scale (CR100) at every second workload.14 Maximal heart rate and the workload at the time of stopping were registered.
Standardised exercise test
A 6 min standardised exercise test was performed at approximately 90% of maximal aerobic capacity (based on the maximal exercise test at visit 1) while breathing dry air (Aiolos Astmatest, Aiolos Medical AB, Karlstad, Sweden). Exercise was identically performed on a treadmill at visits 2, 4 and 5.10 During exercise the patients wore a nose clip and breathed through a tube connected to a gas cylinder containing dry air. FEV1 was measured 15 min before exercise and 1, 5, 10, 15 and 30 min after conclusion of the exercise after which terbutaline was inhaled (2 mg in patients ≥15 years old and 1 mg in patients <15 years old) and FEV1 was measured 15 min later.
If the exercise test at visits 4 or 5 was finished before the stipulated endpoint defined at visit 2, the patient was rescheduled another test or excluded from the study (investigator’s choice).
No asthma drugs were allowed 24 h prior to the exercise tests. Patients were instructed to perform physical exercise 24–48 h before and to abstain from physical exercise during the 24 h prior to the exercise tests.
Diary recording of asthma symptoms
At the third visit the patients gained access to an electronic diary (uniform resource locator (URL)) to record physical activities, asthma symptoms and use of as-needed medication on a daily basis. Asthma symptoms were rated on a scale from 1 to 5, with higher scores indicating less asthma control.
A shortened version of the ACQ5 was completed at visits 1, 3, 4 and 6.15
Outcome measures
The primary outcome variable was the change in maximal post-exercise decrease of FEV1 following a standardised exercise test, performed after 6 weeks of treatment, without any medication during the 24 h prior to the test, and compared with the pretreatment result.
Secondary outcome variables were the alteration of maximal post-exercise FEV1 fall after 3 weeks, ACQ5, patient-reported symptoms and use of study drugs inhaled prior to training sessions and for symptom relief.
Safety outcome measures included adverse events, serious adverse events and changes in vital signs (pulse and blood pressure).
Statistical analyses
Results are presented as mean±SD or 95% CI. Maximal change in post-exercise FEV1 before and after 6 weeks of treatment was analysed by analysis of covariance, with treatment as a factor and the baseline value of the post-exercise FEV1 before treatment as the covariate. Secondary variables were similarly analysed and used to evaluate the protective effect of the treatments over time. All analyses were prespecified.
Based on previous results, a non-inferiority limit for the comparison between the protection against EIB in the formoterol/budesonide group and the regular budesonide group was defined as a difference in post-exercise FEV1 fall <7.28%.16 Non-inferiority analysis was based on a sample size of 66 randomised patients, with 80% power, assuming a SD of 7.13 (estimated from Jonasson et al16) with a 5% significance level. Statistical analyses were performed using SAS V.9.2 (SAS Institute Inc). Randomisation envelopes were generated by a central randomisation system (GRAND, AstraZeneca AB).
Results
Patients and baseline characteristics
Patients were enrolled from September 2009 to July 2010. A total of 189 patients were assessed for eligibility, of whom 66 were randomised and allocated to study treatment. Reasons for exclusion were a post-exercise FEV1 fall <10% at visit 2 (n=94), a baseline FEV1 < 80% of predicted value at visit 1 (n=9), other diseases (n=8), clear need for continuous treatment with inhaled steroids (n=6) and other, not specified, reasons (n=6).
Primary outcome data were available at visit 5 in 59 patients. Results and safety analyses from patients with missing data at visit 5 (n=7) were carried forward from visit 4 and included in the full analysis set of 66 patients. Four of these patients were excluded from the per protocol analysis set, three in the budesonide group due to non-compliance with maintenance budesonide treatment and one in the budesonide+formoterol group who took extra medication on most days.
Patient characteristics are presented in table 1. There were more ex-smokers in the budesonide/formoterol group than in the other groups, but lung function did not differ between ex-smokers (FEV1 99.4±11.9% of predicted value; FEV1/forced vital capacity (FVC) 0.81±0.06) and never-smokers (FEV1 98.6±10.2% of predicted value; FEV1/FVC 0.80±0.08). Relevant medical conditions other than asthma were found in 27 patients (most commonly, allergic rhino-conjunctivitis and rhinitis).
Patient characteristics at baseline (visit 1)
Exercise tests
The maximal workload at the maximal exercise test was 246.4±61.7 W. Mean maximal leg fatigue Borg score was 81.0±24.0 and the maximal dyspnoea score was 89.1±22.4, indicating breathlessness limiting physical performance rather than leg fatigue.
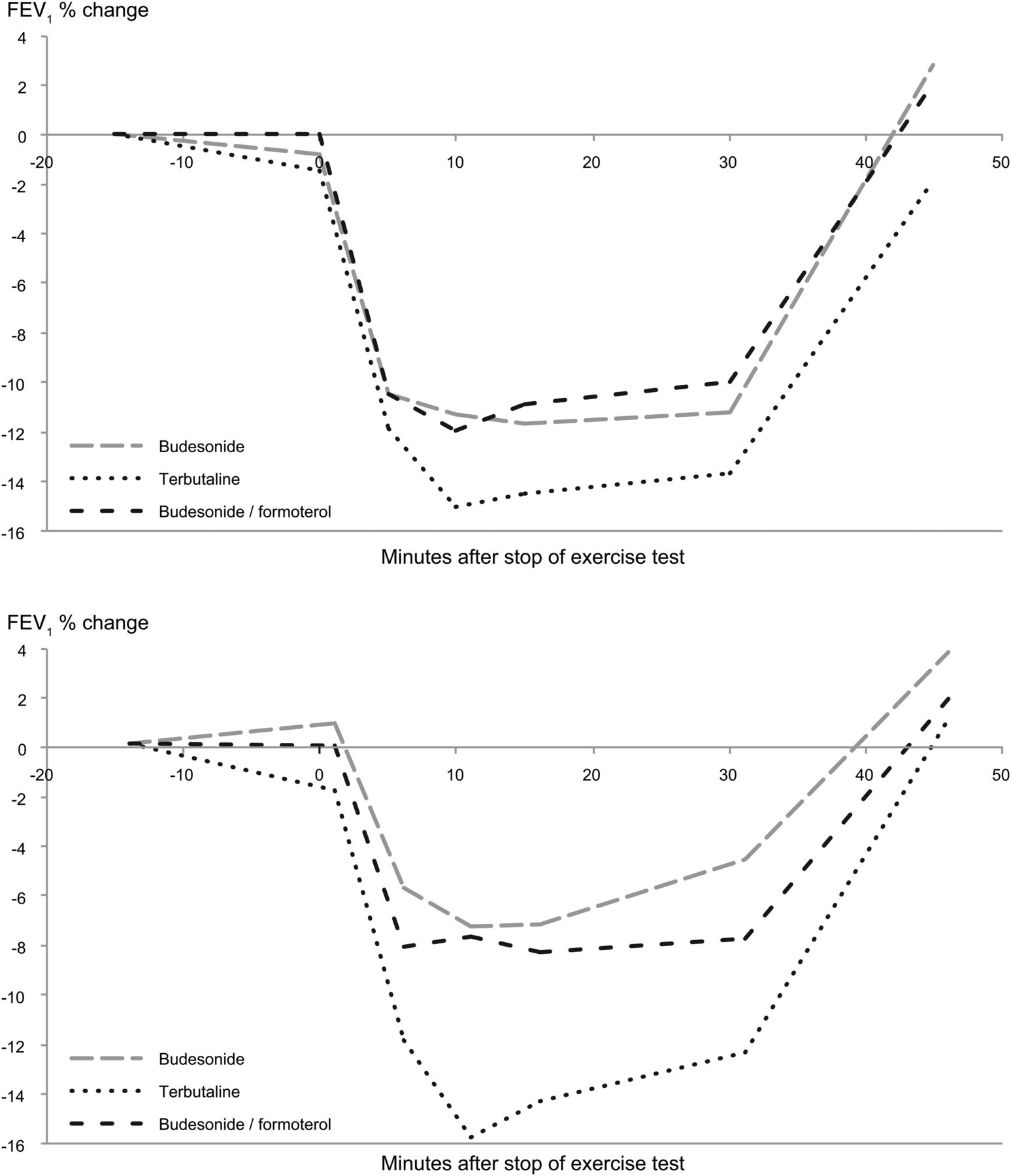
Compared with the exercise test performed before treatment, the maximum post-exercise FEV1 fall after 6 weeks of treatment was 5.4% (mean; 95% CI −8.9 to −1.8) smaller in the budesonide/ formoterol on-demand group, 6.6% (−10.3 to −3.0) smaller in the regular budesonide group and 1.5% (−2.1 to+5.1) greater in the terbutaline on-demand group (table 2, figure 2). Compared with pretreatment results, EIB was reduced by 28.5% in the budesonide/formoterol on-demand group and by 38.6% in the regular budesonide group, and increased by 8.9% in the terbutaline on-demand group after 6 weeks of treatment (table 2).
The maximal post-exercise fall in FEV1 compared with pre-exercise values at baseline (ie, at randomisation) and after 3 and 6 weeks of treatment in the group inhaling regular placebo and terbutaline on demand, regular budesonide and terbutaline on demand and regular placebo and the combination of budesonide+formoterol on demand

Forced expiratory volume in 1 s (FEV1) before and after a 6 min standardised exercise test on a treadmill, while breathing dry air, before treatment (upper panel) and after 6 weeks of treatment (lower panel) with the three different treatments.
The effect of treatment on post-exercise FEV1 fall differed between the terbutaline on-demand group and the budesonide/formoterol group (p=0.017) and the regular budesonide group (p=0.026).
After 3 weeks a small reduction in EIB was observed in the budesonide/formoterol group (p=0.051) and the regular budesonide group (p=0.113) but not in the terbutaline group (table 2).
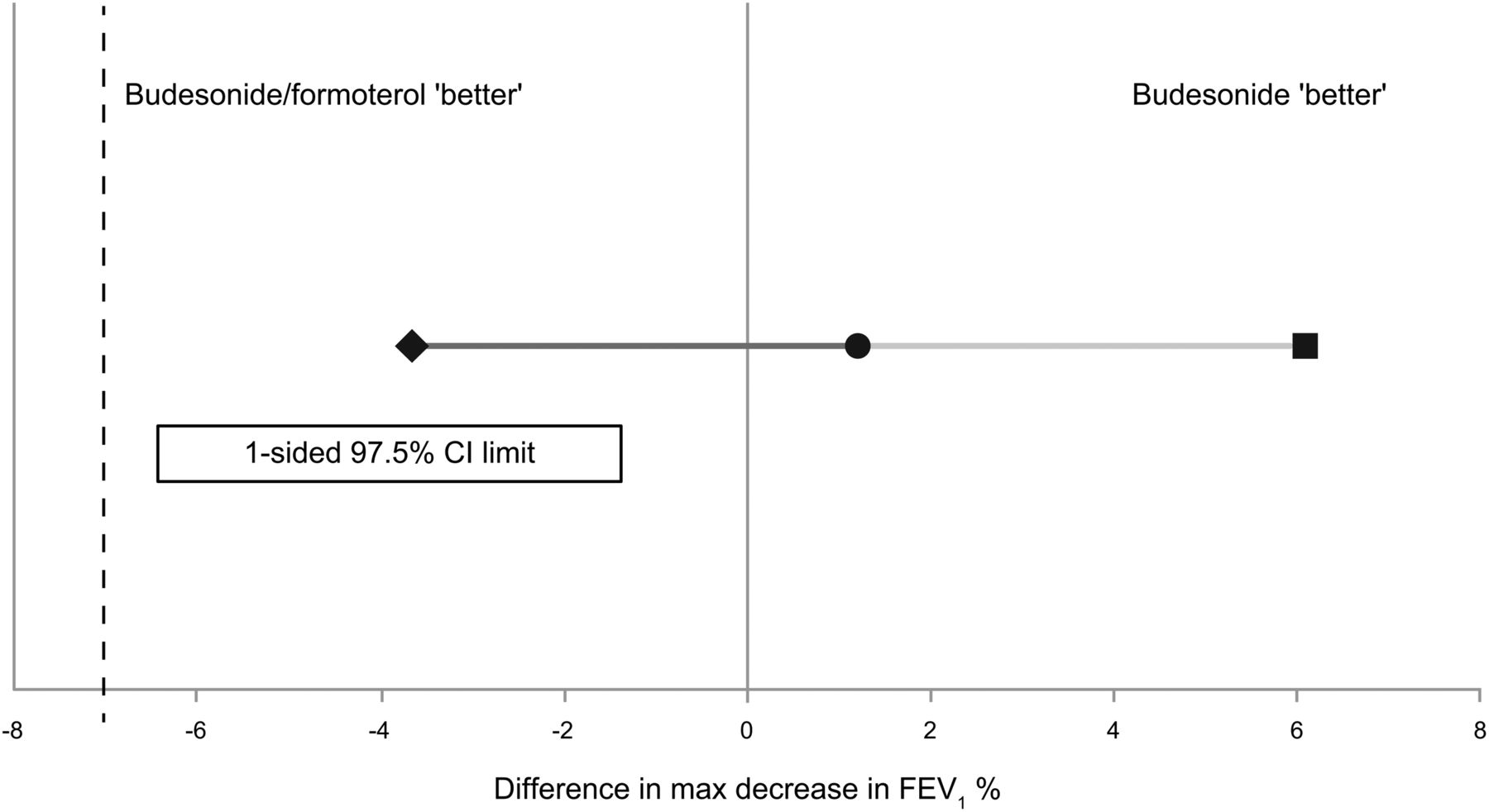
Maximal post-exercise FEV1 fall after 6 weeks was 1.2% in favour of regular budesonide treatment compared with the budesonide/formoterol on-demand group. Non-inferiority for the combination treatment on demand compared with regular budesonide treatment was proven for the main outcome variable (figure 3).
{kind=link}
{kind=link}
{kind=link}
Demonstration of non-inferiority between budesonide on a regular basis (400 μg daily) and terbutaline (0.5 mg) on demand versus the combination of budesonide (400 μg) and formoterol (6.0 μg) on demand in the per protocol population. FEV1, forced expiratory volume in 1 s.
Effects on other variables
Asthma was well controlled after 6 weeks of treatment (ACQ5, table 3). Symptom score was low on days with exercise and there were almost no symptoms on days without exercise (table 3). Symptoms and ACQ scores did not differ between the groups at any visit.
Measures of asthma control
The daily dose of inhaled budesonide was on average 393 μg in the regular budesonide group and 163 μg in the group who inhaled the combination on demand (table 4). The need for extra medication, prior to exercise and for symptom relief, was similar in the three groups (table 4).
Intake of study drugs throughout the study
Safety
All treatments were well tolerated and no drug-related adverse events or serious adverse events were reported. No patient discontinued treatment due to an adverse event. The most common adverse events reported by the patients (n=66) were common cold, cough, sore throat and gastroenteritis.
Discussion
In this study it was demonstrated that a 6-week treatment regimen with inhalation of a combination of budesonide and formoterol on demand was superior to on-demand inhalation of a SABA in reducing EIB, assessed by an exercise test performed after a 24 h period free from any medication. Furthermore, the reduction in EIB after 6 weeks of treatment with inhaled budesonide/formoterol on demand was non-inferior to daily inhalation of budesonide. This finding clearly indicates that treatment with three to four doses per week of the combination is sufficient to provide good asthma control, implying no need for regular treatment with inhaled corticosteroids (ICS) in patients with mild asthma.
According to current guidelines, patients with EIB should inhale a rapid-acting β2 agonist prior to exercise and if reliever medication is needed more than twice a week, regular controller therapy with ICS should be considered.1 Our study included patients with mild asthma in whom inhaled steroids were not indicated according to the treating physician and who inhaled reliever medication up to four times a week. These patients often inhale a β2 agonist before exercise as routine, implying that the exact need for treatment is not known. In clinical practice these patients are frequently treated with a rapid SABA or LABA on demand as the only medication. In the present study all three groups of patients seemed have well controlled asthma from a clinical point of view, as their consumption of extra medication was approximately one inhalation per week or every second week. This shows that the favourable result obtained in the budesonide/formoterol group cannot be explained by a higher number of extra inhalations.
Although terbutaline protected against EIB when inhaled on demand throughout the study, as indicated by the low symptom scores even on exercise days, the bronchial response to exercise was unaltered, or even slightly increased, after 6 weeks of treatment with inhaled terbutaline on demand as monotherapy. As the symptom scores did not differ between groups on the exercise days, the patients did not seem to perceive a difference in the protective effect between terbutaline and budesonide/formoterol when inhaled prior to exercise. However, the results clearly indicate that treatment with the combination on demand provides better protection for occasional, unplanned exertion than terbutaline on demand as monotherapy. Continuous treatment with a β2 agonist may increase the bronchial response to methacholine17 and exercise.18 In addition, the enhancement of bronchial response to methacholine induced by repeated low-dose allergen challenges is counteracted by inhalation of a combination of a steroid (budesonide) and a rapid-acting β2 agonist (formoterol) but not by inhalation of formoterol alone.19 There are thus a number of studies showing that regular treatment with a β2 agonist alone has no beneficial effect on airway responsiveness over time. The present study is in agreement with these findings, as treatment with a β2 agonist alone did not alter airways response to exercise over time. We conclude that monotherapy with a β2 agonist on demand, which is not indicated for regular use in more severe asthma,20–22 may also be avoided in patients with mild asthma.
In our study, the long-term protective effect on EIB was similar in the groups who received budesonide, demonstrating that budesonide+formoterol inhaled on demand was non-inferior to regular, daily corticosteroid therapy, despite a 2.5-fold lower total corticosteroid dose. The combination of budesonide and formoterol, used as maintenance and reliever therapy, prevents exacerbations and symptoms more effectively than regular inhalations of the combination with rapid-acting bronchodilators as reliever.23–26 In all these studies the ICS/LABA combination has been given as maintenance and as reliever therapy. This treatment strategy has been used in subjects with more severe asthma, that is, in patients who need regular treatment with a combination of inhaled steroids and LABAs. For the first time it was shown that on-demand use of an ICS/LABA combination is non-inferior to regular treatment with an ICS in patients with asthma and EIB, indicating that treatment with the combination on demand is an alternative to regular corticosteroid treatment in patients with mild asthma.
It could be argued that 6 weeks of treatment may be too short to achieve the full effect of the steroid on EIB and that the dose of budesonide may be too low to achieve maximal effect. In a 3-month study of children with a history of wheezing, but not documented EIB, a daily dose of 400 μg of beclomethasone dipropionate totally abolished post-exercise bronchoconstriction after 1 month of treatment.27 Six weeks of inhaled budesonide, 1600 μg daily, reduced EIB compared with placebo in adults.28 In children with asthma EIB was reduced after 3 weeks of treatment29 and in another paediatric study a daily dose of 200 μg fluticasone reduced EIB within 4 weeks of treatment.30 The effect of inhaled steroids on EIB thus appears after a few weeks of treatment, indicating that 6 weeks of treatment is sufficient for a study of this type.
A high dose of budesonide (1600 μg/day) reduced EIB by 17% in adult patients with asthma who had a pretreatment post-exercise FEV1 fall of 26%.28 In our study the post-exercise FEV1 fall prior to randomisation was 15–18%, indicating that the patients had mild asthma and there was not much room for improvement. Although studies in children clearly indicate that the effect of inhaled steroids on EIB appears at low doses, we cannot exclude the possibility that a higher dose of budesonide in the group that received regular treatment would have improved the results further. The present data do not allow any conclusions to be drawn regarding possible dose–response relationships between on-demand medication with the combination of budesonide/formoterol and the protection against EIB.
In conclusion, in mild asthma a combination of an inhaled corticosteroid and a long and rapid-acting β2 agonist used on demand is superior to the use of an inhaled SABA alone in reducing EIB. In addition, inhalation of the combination on demand is not inferior to regular treatment with the corticosteroid alone in these patients, despite a 2.5-fold lower dose of the steroid. The results may have implications for treatment guidelines in patients with mild asthma.
References
Footnotes
-
Contributors KL: study design. NL, BD, LB, TP, GH and KHC: patient recruitment, enrolment, randomisation and follow-up. LJ and TE: collection of data. LJ: statistical analysis. NL, LJ, TE, GH, TP, LB, BD, KHC and KL: analysis, interpretation of the data and writing of the manuscript.
-
Funding The study was sponsored by Astra Zeneca.
-
Competing interests NL has served as a speaker and/or participated in education arranged by Takeda. LB has, during the past 5 years, on one or more occasion served on an advisory board and/or served as a speaker and/or participated in education arranged by Aersonett, Aerocrine, Almirall, Andre-Pharma-Chiesi, AstraZeneca, Boehringer Ingelheim, GSK, Meda, MSD, Niigard, Nycomed, Novartis and Takeda. BD has, during the past 5 years, on one or more occasion served on an advisory board and/or served as a speaker and/or participated in education arranged by Actelion, Meda and Novartis. TP has, during the past 5 years, on one or more occasion served on an advisory board for MSD and served as a speaker in education arranged by Meda, GSK and ALK. GH has in relation to this paper no conflict of interest. KHC has no conflict of interest related to the present manuscript. He has served on consultatory boards over the past 3 years for Boehringer – Ingelheim, Meda and Nycomed. He has given lectures for Boehringer – Ingelheim, Meda, Nycomed and Merck. He has received unrestricted research grants from The Norwegian Health Authority South-East. KL has, during the past 5 years, on one or more occasion served on an advisory board and/or served as a speaker and/or participated in education arranged by AstraZeneca, Boehringer Ingelheim, GSK, Meda, MSD, Nycomed, Novartis, Takeda, and Pfizer. Kjell Larsson has also received unrestricted research grants from AstraZeneca, Boehringer Ingelheim, and GSK.
-
Patient consent Obtained.
-
Ethics approval The Ethics Committee of Stockholm (D5890L00032) and the Regional Ethics Committee of Health Region South East of Norway.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves