Article Text

Abstract
Objective: To systematically review the evidence for the medium to long term benefits and risks of montelukast as add-on therapy to inhaled corticosteroids (ICS) in comparison with placebo and active controls in mild to moderate asthma.
Data sources: Medline, Embase, Cochrane Register of Controlled Trials, reference lists of retrieved articles, clinical trial registries and study results databases.
Review methods: Systematic review of randomised controlled trials (duration ⩾12 weeks) in adolescents and adults comparing montelukast/ICS versus ICS monotherapy or montelukast/ICS versus active control/ICS. Meta-analyses were conducted where feasible. The main focus was on clinical outcomes (eg, exacerbations). Adverse events were also assessed.
Results: 13 studies meeting all of the inclusion criteria were identified: 7 studies, including constant or tapered doses of ICS, compared montelukast/ICS with ICS monotherapy. Six studies compared add-on montelukast with an add-on active control (salmeterol). Overall, the data indicated that montelukast/ICS was clinically more effective than ICS monotherapy. The ICS sparing potential of montelukast was clearly demonstrated in one study. Montelukast/ICS and ICS monotherapy showed similar safety profiles. In the active controlled studies, montelukast/ICS was clinically less effective than salmeterol/ICS in the 12 week trials (pooled proportion of patients with ⩾1 exacerbation: p = 0.006). However, separate analysis of active controlled 48 week trials showed comparable proportions for patients with ⩾1 exacerbation in both groups.
Conclusions: Montelukast as add-on therapy to ICS improves control of mild to moderate asthma compared with ICS monotherapy. Although the addition of salmeterol to ICS is clinically as effective as or even more effective than the addition of montelukast, montelukast may have a better long term safety profile and offer a treatment alternative for asthma patients.
Statistics from Altmetric.com
Asthma is characterised by a chronic inflammation process with increased numbers of activated eosinophils, mast cells, macrophages and T lymphocytes in the airway mucosa and lumen, which produce mediators of inflammation such as histamine, prostaglandins and leucotrienes. Cysteinyl leucotrienes are potent inflammatory mediators produced by the 5-lipoxygenase pathway of arachidonic acid metabolism, and are believed to play a major role in the pathophysiology of asthma by mediating bronchoconstriction and inflammatory reactions.1
Leucotriene modifiers, including leucotriene receptor antagonists (LTRA), are a relatively new class of antiasthmatic drugs. Evidence exists that LTRA, by blocking the leucotriene receptors of the smooth airway muscles, reduce airway eosinophilic inflammation and alleviate symptoms of airway obstruction.2 3 Many clinical trials have shown LTRA to be effective in asthma therapy.4 They also have the advantage of being administered orally. However, as inhaled corticosteroids (ICS) are more effective than LTRA in reducing asthma exacerbations,5 ICS remain the first choice in asthma management whereas LTRA are recommended as an add-on therapy to ICS.6–8
In a Cochrane review by Ducharme, the efficacy of LTRA as add-on therapy to ICS was assessed, and LTRA were shown to achieve modest improvement in asthma control.9 In a further Cochrane review by Ram et al, LTRA were found to be inferior to long acting β2 agonists (LABA) in asthmatic patients whose symptoms were suboptimally controlled with ICS therapy.10 Trials with a relatively short duration of treatment (minimum of 28 days) were included in both Cochrane reviews. However, conclusions about the long term efficacy (including the possible development of tolerance) and safety of antiasthmatic drugs in chronic asthma should be supported by trials of at least 6 months’ duration.6 11 Long term drug effects may be a crucial point when comparing LTRA with LABA as add-on therapies. Pooling of data without a separate analysis of long term trials may make it difficult to identify these long term effects.
In most European countries, montelukast is the only approved LTRA, and is licensed as an add-on therapy to ICS in patients with mild to moderate chronic asthma. Both Cochrane reviews (as well as most other previous reviews) included LTRA not approved in Europe (eg, zafirlukast and pranlukast).5 9 10 12 13 Therefore, the results of these reviews are not applicable to the European healthcare setting and to clinical practice guidelines, such as the British and German asthma guidelines.7 8 Furthermore, many previous reviews focused on lung function as a primary outcome, and less emphasis was placed on clinical outcomes.5 9 10 12 13
This systematic review evaluates the scientific evidence for the benefits and risks associated with the medium to long term use (⩾12 weeks) of montelukast as add-on therapy to ICS in asthmatic adolescents and adults compared with ICS monotherapy or other treatment options recommended by guidelines.6 7 As montelukast is approved in Europe only for the treatment of mild to moderate asthma, this review only included studies in appropriate patients, and focused on outcomes relevant to patients, such as disease related symptoms and quality of life.
METHODS
The German Institute for Quality and Efficiency in Health Care
This systematic review formed part of a health technology assessment of montelukast carried out by the German Institute for Quality and Efficiency in Health Care (Institut für Qualität und Wirtschaftlichkeit im Gesundheitswesen, IQWiG). The full (German language) report is available on the institute’s website.14 The responsibilities and methodological approach of IQWiG are described in its methods paper.15
Search strategy
We searched MEDLINE (1966 to November 2006), EMBASE (1980 to November 2006) and the Cochrane Central Register of Controlled Trials (CENTRAL, November 2006) for randomised controlled trials (RCTs) using a comprehensive search strategy including the following keywords: asthma, bronchospasm, bronchoconstriction, leucotriene antagonist, antileucotriene, montelukast and singulair. Details of the full search strategy have been described elsewhere.14 The Cochrane Database of Systematic Reviews, the Database of Abstracts of Reviews of Effects and the Cochrane HTA Database were searched for relevant secondary publications. We also reviewed the references cited by the publications identified to obtain details of further studies. Clinical trial registries and study results databases available on the internet were also screened, as well as the websites of the European Medicines Agency and US Food and Drug Administration.11 16 Moreover, the pharmaceutical companies producing montelukast (MSD Sharp and Dohme GmbH (MSD), Haar, Germany) or the active comparator used in the studies identified (salmeterol; GlaxoSmithKline (GSK), Munich, Germany) were asked to supply additional unpublished data.
Study selection
We included all publications that presented original data from RCTs if they fulfilled the following criteria: investigation of montelukast as add-on therapy to ICS in adults and adolescents (⩾12 years) with mild to moderate asthma; language of publication: English, German, Dutch, French, Spanish or Portuguese; evaluation of at least one of the following predefined outcomes: asthma symptoms, exacerbations with or without emergency treatment, hospitalisation and/or outpatient treatment, adverse events, activities of daily living, disease related quality of life, treatment satisfaction, physical capacity, asthma related mortality and total mortality. As asthma is a chronic condition, short term trials (<12 weeks) were excluded. Although guidelines recommend 24 week trials to evaluate the effects of long term treatment, we also included medium term trials with a study period ⩾12 weeks in order to perform separate analyses to assess the effect of study duration.
Relevant publications retrieved from the primary literature search were identified independently by two reviewers (SJ, AM); firstly, by perusal of the study titles and abstracts to exclude evidently irrelevant publications, and secondly, by assessing the full texts of the remaining potentially relevant publications. The classification of the trials (relevant or not relevant) was subsequently discussed with BW, UG and TK, and any disagreement was settled by consensus.
As the review aimed to investigate montelukast in patients with mild to moderate asthma, trials in patients with severe asthma were excluded. It was originally planned to evaluate asthma severity using the definitions provided in the individual trials. However, this approach proved to be impossible, because information on asthma severity was insufficient in most publications. As a consequence, the proportion of patients with severe asthma (defined as forced expiratory volume in 1 s (FEV1) per cent predicted ⩽60% at baseline) was estimated from available FEV1% predicted data, and subsequently studies with more than 20% of patients with severe asthma were excluded from the review. To investigate the impact of this exclusion, a sensitivity analysis was conducted considering the results of trials in patients with severe asthma, and the conclusions of the review were reassessed.
Data extraction and validity assessment
Data extraction and quality assessment of the trials were conducted according to the methods of the IQWiG.15 Information and data from publications were supplemented by publicly available reports from study registries and unpublished study reports provided by MSD and GSK (table 1). Firstly, data were extracted by two of the authors (SJ, AM) using standardised extraction forms. Secondly, the consistency of data within the publication and with additional data sources such as the corresponding study report was assessed. The third step was a global appraisal of the study and publication quality based on the following quality criteria: characteristics of the study design, appropriate randomisation and allocation concealment, blinding of patients and investigators, sample size estimation, complete description of dropouts and appropriate application of the intention to treat principle.
Trials were then classified using the following quality categories: “no deficiencies” (study meets all quality criteria); “minor deficiencies” (deficiencies exist that do not affect the main conclusion); and “major deficiencies” (deficiencies exist that challenge the main conclusion).
Methods of quantitative data synthesis
Results for each of the predefined outcomes were compared between studies. If feasible and meaningful, data were pooled by means of meta-analyses. Effect measures were reported as relative risks (for binary data). A fixed effect model was used primarily to calculate a pooled effect estimate. As I2 as a measure of heterogeneity of effect sizes between studies17 was 0 in all pooled analyses presented in this article, fixed effect models were used. Statistical significance was assumed for p<0.05.
RESULTS
Trial flow
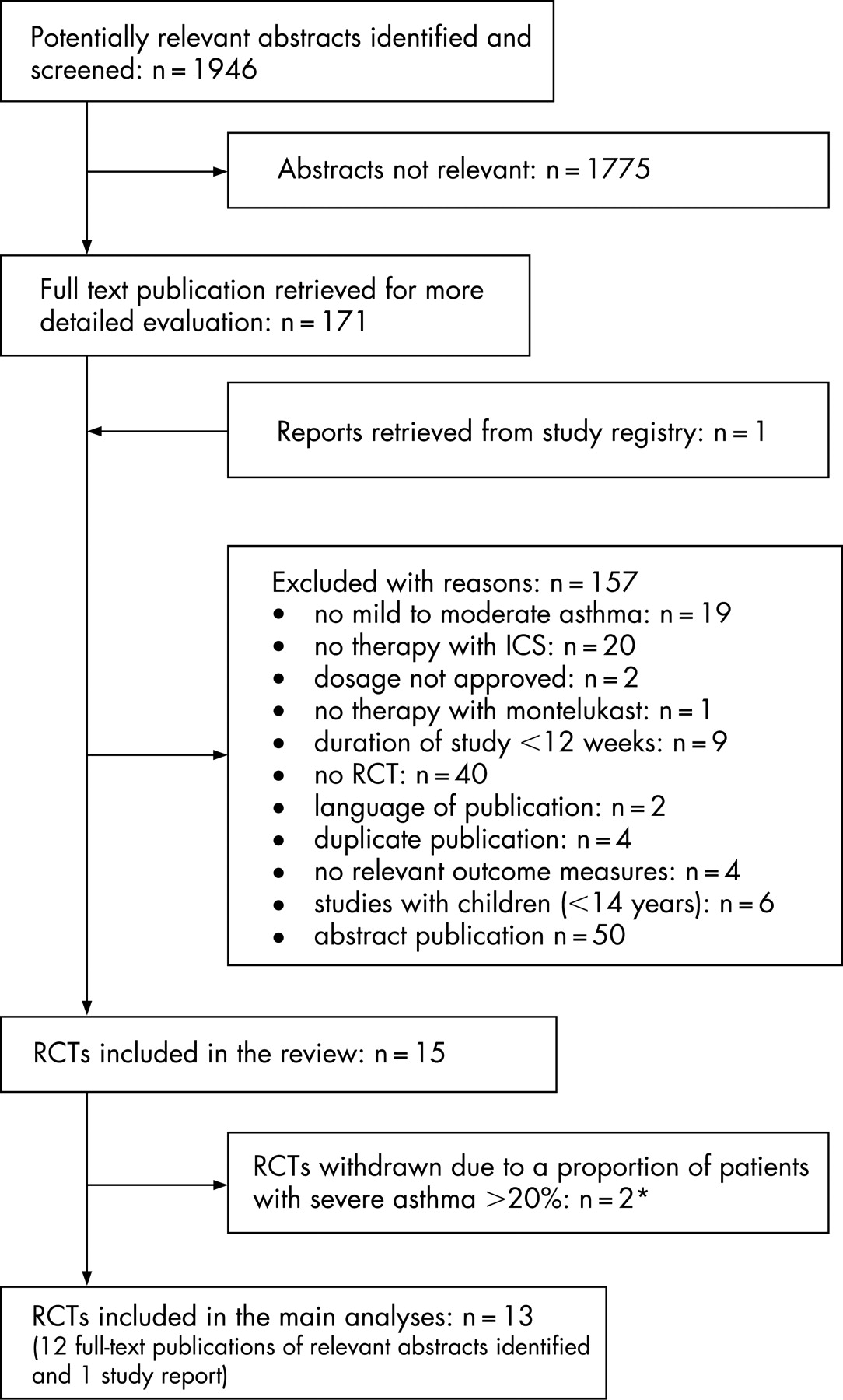
Of 1637 potentially relevant abstracts, 12 studies fulfilled the inclusion criteria. In addition, one relevant study report was identified (fig 1).
Study characteristics
Table 1 shows the main characteristics of the studies included. In most studies, the mean age of participants ranged from 38 to 45 years. Treatment duration ranged from 12 to 48 weeks. The number of patients included per study varied between 30 and 1490. Mean FEV1 at baseline was between 70% and 99% predicted.
Three types of protocols were used: (1) montelukast as add-on therapy to constant dose ICS versus constant dose ICS monotherapy (with or without placebo)18–20; (2) montelukast as add-on therapy to tapered doses of ICS versus tapered doses of ICS monotherapy (with or without placebo)21–24; (3) montelukast versus salmeterol as add-on therapy to constant dose ICS.25–30
In all studies, montelukast 10 mg was given as add-on therapy to ICS. Steroid regimens (dosage and agent) varied in the trials investigated. In the studies with tapered doses, ICS were reduced either according to a predefined protocol21 23 or according to clinical asthma scores.22 24 In five active controlled studies, addition of montelukast to constant dose fluticasone 100–250 μg twice daily was compared with the addition of salmeterol 50 μg twice daily.25–30 In the Grosclaude study,27 constant dose beclomethasone was administered in the montelukast group while fluticasone was used in the salmeterol group. In three studies,26 27 29 salmeterol and fluticasone were administered as a fixed combination.
In all studies, there was a run-in phase of 1–7 weeks, and in some studies all patients were switched to the same ICS agent during this phase.
In general, rescue β2 agonists were permitted; however, in two studies, this was not clearly described.23 25
Table 2 summarises the methodological quality of the trials: six trials had minor or no deficiencies; seven trials failed to show sufficient methodological quality to draw a conclusion about the results of these studies. Common shortcomings included deficiencies in the randomisation and allocation concealment process, missing sample size calculations and incomplete description of dropouts. Furthermore, nearly half of the studies lacked, or had inappropriate application of, an intention to treat analysis. A double blind design was used except for three trials,19 23 27 two of which had an open label design and one whose design was unclear. As the extent of potential bias in open studies cannot be estimated, open studies were allocated to the category “major deficiencies”.
Quantitative data synthesis
The outcome measures investigated were not consistent between studies (tables 3, 4). In one of the studies, one death was reported (“death with severe asthma attack” after 15 days of treatment with salmeterol/fluticasone).25
Montelukast as add-on therapy to constant dose ICS versus constant dose ICS monotherapy
Only one study20 was of good methodological quality. Overall, symptom control was significantly better with montelukast, as shown by asthma symptom scores,18 the number of asthma-free days20 or nocturnal awakenings18 20 (table 3). Exacerbations were also significantly reduced with montelukast.18 20 However, regarding quality of life and treatment satisfaction, there were no significant differences between treatment groups.18 20 The addition of montelukast did not result in higher overall adverse event rates or increased withdrawal rates as a result of adverse events. There were no data on hospitalisation and additional visits to physicians available.
Montelukast as add-on therapy to tapered doses of ICS versus tapered doses of ICS monotherapy
Of the four studies assessing the ICS sparing potential of montelukast, only the study of Löfdahl et al fulfilled all of the quality criteria.22 Furthermore, this study was the only one that included a dose optimisation period in the run-in phase. The “last tolerated dose” of ICS was the primary outcome measure, and addition of montelukast allowed a significant reduction in ICS baseline dose (last tolerated dose 526 μg/day (montelukast/ICS) vs 727 μg/day (ICS only); p = 0.046).
In the study by Kanniess and colleagues,21 daytime symptoms after ICS dose reduction were not altered in the ICS monotherapy group but significantly reduced by montelukast (data not shown, p<0.05).
Montelukast versus long acting β2 agonists (salmeterol) as add-on therapy to constant dose ICS
With regard to asthma symptoms and exacerbations, most of the active controlled trials (of which two-thirds were of good or acceptable methodological quality) showed that patients benefit more from salmeterol than from montelukast as add-on therapy (table 4). In a meta-analysis of the 12 week trials, salmeterol was significantly superior regarding the proportion of patients with exacerbations (RR 2.03, 95% CI 1.23 to 3.37, p = 0.006) (fig 2). However, in the respective analysis of the 48 week trials, the difference between the montelukast/ICS and salmeterol/ICS groups was not significant (fig 2). One 48 week trial25 demonstrated the non-inferiority of montelukast compared with salmeterol with regard to exacerbations, while in the other,28 non-inferiority was not shown.

The rates for hospitalisation and emergency treatment were similar between groups whereas the data on additional visits to physicians were inconclusive (table 4). In the studies of Ilowite and colleagues28 and Ringdal and colleagues,30 quality of life and treatment satisfaction, respectively, were evaluated significantly more positively by patients in the salmeterol group. In contrast, Bjermer and colleagues25 found no difference in quality of life between treatment groups.
The overall adverse event rates were comparable. However, separate meta-analyses of 12 and 48 week trials indicated that salmeterol had a less favourable long term safety profile; the pooled data of the Bjermer and Ilowite studies25 28 showed a significantly higher rate of serious adverse events in the salmeterol group (RR 0.68, 95% CI 0.49 to 0.94, p = 0.021) (fig 3).

{kind=link}
{kind=link}
{kind=link}
Sensitivity analysis
Two studies were excluded from the main analysis because they included more than 20% of patients with severe asthma (estimation of proportion of patients with FEV1% predicted ⩽60% based on mean and SD of FEV1% predicted at baseline).31 32 The study by Price and colleagues31 investigated montelukast/budesonide 800 μg versus budesonide 1600 μg. Comparable outcomes were observed. Thus the Price study confirms an ICS sparing potential of montelukast; this was also reported by Löfdahl and colleagues.22 The study by Fish and colleagues,32 which described a pooled analysis of two 12 week studies comparing montelukast/ICS and salmeterol/ICS, also showed better symptom control in patients receiving salmeterol/ICS. When the data from the Fish study were included in the meta-analysis of serious adverse events in the 12 week studies, the overall result of the analysis did not change (RR 1.17; 95% CI 0.55 to 2.47). However, inclusion of these data in the meta-analysis of exacerbations resulted in a non-significant difference between treatment groups (RR 1.41; 95% CI 0.98 to 2.02) compared with a significant difference in favour of salmeterol observed in the meta-analysis excluding patients with severe asthma (fig 2).
DISCUSSION
This systematic review evaluated add-on therapy in patients with asthma who remained symptomatic on ICS. In all included studies, ICS dosage was sufficient considering the flat dose–response of ICS, with most of the therapeutic benefit with a total daily dose of 100–250 μg for fluticasone49 and 400 μg for budesonide50 or equivalence, respectively, which is of particular importance when investigating secondline controller therapy. Data from the studies examined in this systematic review indicate a clinical advantage of montelukast/ICS versus ICS monotherapy. In contrast, montelukast/ICS was clinically less effective than salmeterol/ICS, at least in the medium term (12 weeks). Pooled data of the active controlled 48 week trials showed that significantly more serious adverse events occurred in patients receiving salmeterol/ICS.
Montelukast as add-on therapy to ICS versus ICS monotherapy
Overall, montelukast as add-on therapy to ICS was more effective with regard to clinical outcomes than ICS monotherapy, although this finding was not reflected by an improvement in quality of life or treatment satisfaction. The ICS sparing potential of montelukast was demonstrated in a confirmative analysis in one study of good methodological quality. However, the other studies investigating this question were of poorer methodological quality, and data on clinical outcomes were scarce. Furthermore, there was variation in the design of the trials with tapered doses of ICS (different tapering protocols and baseline doses of ICS, lack of a dose optimisation period prior to randomisation), which made pooling of the data and interpretation of study results difficult. Ideally, future studies on ICS sparing effects of LTRA should use comparable study protocols and include a prolonged run-in period that optimises the ICS dose to the minimum effective dose. In addition, ICS doses should be tapered according to clinical asthma scores.
Montelukast versus long acting beta agonists (salmeterol) as add-on therapy to ICS
The efficacy of montelukast may be explained by its anti-inflammatory effect, which is the hallmark of asthma therapy.33 The importance of reducing eosinophilic inflammation was demonstrated in several studies.34–36 Despite the fact that this therapeutic principle seems to be addressed with montelukast, its impact on symptom reduction and quality of life is weaker compared with LABA, at least in the medium term.
However, much controversy currently surrounds the use of LABA.16 In our review, the increased rate of long term serious adverse events in the LABA group deserves particular attention, as not only the SMART study37 but also a recent meta-analysis38 showed an increase in asthma related deaths in patients using LABA. However, according to exploratory subgroup analyses,48 the increase in asthma related deaths is mainly in those patients who are taking LABA without ICS. Following the SMART study, the US Food and Drug Administration issued a warning about the increased risk of adverse outcomes with LABA.16
Interestingly, in the discussion section of the Cochrane review comparing LTRA and LABA as add-on therapy to ICS, the authors point to the wide confidence interval for serious adverse events, which included the possibility of an increased risk of such events in the LABA group.10 This trend became statistically significant in our subanalysis of long term trials. A negative feedback mechanism of the β adrenergic system as an adaptive response to the stimulation of receptors is suspected of being responsible for the worsening of asthma control.39
In the light of the current safety discussion,38 montelukast may be a treatment alternative in asthma that is suboptimally controlled with ICS. The disadvantage of slower symptom relief with montelukast27 28 30 may be counterbalanced by possibly better long term safety. In consequence, treatment regimens recommended in guidelines should be re-discussed, taking the risk–benefit profile of montelukast and other treatment options into account. In this regard, concerns may be raised about a potential link between leucotriene receptor antagonist use for asthma and the onset of Churg–Strauss syndrome, a rare disease with a poorly understood pathogenesis.
Long term trials are needed for a conclusive evaluation of the long term efficacy and safety of various alternative controller medications in patients with mild to moderate asthma. In those trials, possible efficacy relevant aspects such as patient age, comorbidities or ethnic group should be considered for study design and analysis. Also, patient acceptance and compliance for oral compared with inhaled preparations should be assessed in future studies as these factors may have a relevant impact on the difference between medium and long term studies.
Strengths and limitations
The value of this review is strengthened by the restriction to studies of at least 12 weeks’ duration. This selection criterion avoids bias in favour of short term effects when pooling data. At the same time, inclusion of 12 week trials allowed an assessment of the effect of study duration.
Inclusion of trials with different clinical outcome measures could be seen as a limitation of this review. At first sight, this approach led to a heterogeneous pool of studies; however, overall, the findings from this pool showed consistent trends.
The outcome measures included in our review were not necessarily defined as primary outcomes in the original studies. Secondary outcome measures may be more prone to reporting bias—that is, it is possible that only outcomes showing significant treatment differences are reported in published articles, resulting in an overestimation of treatment effects.40 However, for the active controlled studies, we were provided with unpublished study reports describing all of the results for primary and secondary outcomes in four of five studies. Thus at least the comparison of montelukast and salmeterol as add-on therapy is less likely to be prone to reporting bias.
Inclusion of both efficacy and safety outcomes turned out to be the strength of our review, as we detected comparable efficacy regarding the risk for exacerbations but significantly higher rates of serious adverse events in patients receiving LABA in the long term active controlled trials. This broad approach may be an explanation as to why this finding was not detected in previous reviews.10 12 Sin et al included trials with a follow-up period of at least 3 months but focused solely on the exacerbation rate as a clinical outcome.12 The Cochrane reviews also used a broad approach but permitted studies with a minimum duration of 28 days.5 10
Clinical trials are often conducted in highly selective patient populations considering factors such as age, ethnic groups, comorbidities, asthma characteristics, etc. This must be taken into account when making conclusions on the basis of study results. In this regard, we cannot exclude preselection of patients, as reversibility of FEV1 was used as an inclusion criterion in the studies. Although FEV1 reversibility is one of the standard diagnostic criteria of asthma,6–8 it is possible that patients who were more likely to respond to LABA may have been selected, rather than asthma patients seen in normal clinical practice. Because of this preselection, the effects of LABA may have been overestimated. It should therefore be questioned whether reversibility of FEV1 is an appropriate inclusion criterion in trials evaluating LABA, and it should also be kept in mind that significant reversibility is difficult to attain in patients on controller therapy.
Studies including more than 20% of patients with severe asthma were not considered in this review. However, defining asthma severity is problematic, as it depends on the time point of the patient’s assessment. Classification of asthma severity in studies is consequently difficult and, because of varying inclusion criteria, not comparable between studies.41 That is why we also included studies with a small proportion (<20%) of patients with asthma classified as “severe”. Two RCTs were excluded from the main analysis because of the large proportion of patients with severe asthma. Although the inclusion of patients with severe asthma in the meta-analysis of 12 week trials nullified the previous significant difference in favour of salmeterol regarding exacerbations, a systematic analysis of the effects of montelukast in patients with severe asthma would be needed to make any firm conclusion about the benefits of montelukast in this patient population.
CONCLUSION
The addition of montelukast to ICS improves control of mild to moderate asthma compared with ICS monotherapy. However, montelukast as add-on therapy to ICS is less effective than the addition of salmeterol with regard to most clinical outcomes, at least in the medium term. Because of the possibly better long term safety profile of montelukast compared with salmeterol, montelukast may be considered as an add-on treatment alternative in patients suboptimally controlled with ICS. These findings indicate that asthma treatment guidelines should be reassessed to clarify whether the current recommendations require modification.
Acknowledgments
The authors thank Elke Vervölgyi for contributing to the quality assessment of studies and Natalie McGauran for editorial support. Both contributors are employed by IQWiG.
All authors conceived the protocol of this review, BW and TK performed the literature search; SJ and AM reviewed all citations for relevance; SJ, AM, BW and UG reviewed all included trials for methods and data extraction; BW and TK corresponded with pharmaceutical companies to obtain collaboration; UG did the statistical analyses; all authors commented on the final manuscript. SJ is the guarantor.
REFERENCES
Footnotes
Funding: This work was supported by the Institute for Quality and Efficiency in Health Care (Institut für Qualität und Wirtschaftlichkeit im Gesundheitswesen, IQWiG)
Competing interests: None.