Article Text

Abstract
Background: Daily recombinant human deoxyribonuclease (rhDNase) is an established but expensive treatment in cystic fibrosis (CF). An alternative lower cost therapy is hypertonic saline (HS), which has been shown to improve lung function in short term studies. This study compares the costs and consequences of daily rhDNase with alternate day rhDNase and HS in children with CF.
Methods: In an open, randomised, crossover trial, 48 children with CF were allocated consecutively to 12 weeks of once daily 2.5 mg rhDNase, alternate day 2.5 mg rhDNase, and twice daily 5 ml 7% HS. Outcomes assessed included forced expiratory volume in 1 second (FEV1) and quality of life. All healthcare resource use was prospectively recorded for each patient. Unit costs were collected and combined with resource use data to give the total health service costs per patient for each treatment strategy.
Results: Daily rhDNase resulted in a significantly greater increase in mean FEV1 than HS (8%, 95% CI 2 to 14) but there was no significant difference in FEV1 between daily and alternate day rhDNase (2%, 95% CI –4 to 9). Over a 12 week period the mean incremental costs of daily rhDNase compared with HS was £1409 (95% CI £440 to £2318), and the incremental cost of using daily rather than alternate day rhDNase was £513 (95% CI –£546 to £1510).
Conclusions: Daily rhDNase is more effective than 5 ml 7% HS twice daily delivered by jet nebuliser, but significantly increases healthcare costs. Administering rhDNase on an alternate day rather than a daily basis is as effective, with a potential for cost savings.
- cystic fibrosis
- rhDNase
- hypertonic saline
- cost
Statistics from Altmetric.com
Cystic fibrosis (CF) is the most common autosomal recessive disorder of the white population. Most of the morbidity and mortality is from pulmonary disease, which is characterised by obstruction of the airways by thick tenacious secretions that are difficult to clear.1 New treatments have improved life expectancy in CF, but have also led to increased costs. Little research has been undertaken to assess the resource use, costs, and outcomes of different treatment options for children with CF.
Clinical trials of recombinant human deoxyribonuclease (rhDNase) in CF have shown improvements in lung function.2,3 However, rhDNase is an expensive treatment, costing £7442 per patient per year,4 and not all patients benefit from it.5 The main evidence on the relative cost effectiveness of rhDNase therapy comes from a study by Oster et al6 using data from a US phase III clinical trial3 which compared the effectiveness of rhDNase with placebo in adults with CF. However, this study excluded the cost of rhDNase and only assessed health costs related to respiratory tract infection. Other studies7,8 have extrapolated these data to the UK which, given the difference in practice patterns between the US and the UK, is unlikely to produce valid results for local decision making. Furthermore, there are no detailed studies of the cost effectiveness of rhDNase in children.
Once daily 2.5 mg rhDNase, the current dose recommended in children, has been shown to be as effective as twice daily 2.5 mg rhDNase.3 There are no studies on the use of alternate day rhDNase which, if equally effective, would halve the drug cost and treatment time. Nebulised hypertonic saline (HS) is an alternative treatment for CF and appears to have beneficial effects on lung function, mucociliary clearance, and sputum expectoration in the short term which are comparable to rhDNase.9,10 The intervention costs substantially less than rhDNase but the relative total costs of care have not been assessed.
Given the high cost of rhDNase and the limited evidence on the total costs of different treatment strategies in children with CF, this study compared the costs and consequences of three mucoactive treatments—daily rhDNase, alternate day rhDNase, and HS.
METHODS
The health economic assessment was conducted in a crossover trial that has been reported in greater detail elsewhere.11 Children with CF aged 5–18 years were enrolled from Great Ormond Street Hospital and the Royal Brompton Hospital, London. Inclusion criteria were the ability to perform spirometric tests and to be either currently on rhDNase or have a forced expiratory volume in 1 second (FEV1) of less than 70% predicted. Exclusion criteria were the inability to take the trial medication, known hypersensitivity to rhDNase or HS, isolation of Burkholderia cepacia in the sputum, pregnancy, and breastfeeding. To ensure that patients were enrolled when they were clinically stable, they had to be free of a lower respiratory tract infection requiring a change in antibiotics, steroids, or bronchodilator treatment during the 14 days before randomisation.
A prospective, open, randomised, crossover trial was performed. Patients already on rhDNase or HS before the study discontinued the treatment at least 2 weeks before commencing the trial. Two weeks has been shown to be sufficient time for complete washout to occur for both HS and rhDNase.2,9 Each patient was allocated to receive, in random order, consecutive 12 week treatments of 2.5 mg rhDNase once daily, 2.5 mg rhDNase on alternate days, and 5 ml 7% HS twice daily. There was a 2 week washout period between treatments.
rhDNase and HS were administered using a Durable Sidestream nebuliser and Porta-Neb compressor (Medic-Aid, Bognor Regis, UK). HS was inhaled twice daily immediately before the patient’s regular physiotherapy. rhDNase was administered once a day or once every other day, at least 1 hour before physiotherapy. There was a 2 week washout period between treatments. The primary clinical outcome was change in FEV1, and secondary outcomes included quality of life (QOL) using the Quality of Well-Being Scale,12 and the number of pulmonary exacerbations defined using a previously outlined protocol for respiratory tract infections.3
Adherence to treatment was monitored in two ways. Patients were asked to return all unused bottles of HS and used vials of rhDNase. From this the percentage of prescribed doses that could have been taken could be calculated. In addition, each patient recorded the treatment doses taken for each trial drug in a patient diary.
Economic evaluation methodology
The methodology used for the study followed recent general guidelines for economic evaluation13 and more specific recommendations for measuring costs alongside randomised controlled trials.14 This meant that resource use and unit costs were reported separately, requiring a detailed approach to resource use estimation. Unit costs were measured at several study sites and the final cost estimates were compared between the study groups using stochastic measures of uncertainty in line with recent recommendations.15,16
Measurement of resource use
All healthcare resources used were assessed, including hospital contacts (inpatient, outpatient and ward review), radiological investigations, blood tests, drug use, and the use of community services (including community nurse, physiotherapist and general practitioner).
Patients were given a diary in which to record any contacts with health professionals and changes in medication during the study. For each hospital admission the duration of stay, reason for admission, health professionals involved, investigations, procedures and management were recorded. Further details were obtained from the patients’ hospital notes, discharge letters, and by contacting the supervising physicians.
The typical time input from different health professionals was recorded for each type of healthcare contact for children with CF. This information was collected from the two postgraduate hospitals where patients were recruited for the trial. In addition, data were collected from a district general hospital (DGH) to represent care provided by that type of hospital.
Unit costs
Unit costs from the relevant departments at the two postgraduate hospitals and from the DGH were collected at a suitable level for combining with the measures of resource use. The annual cost of employing the midpoint of each grade of health professional (including employers’ costs and overtime payments but excluding London weighting allowance13) was divided by the number of hours worked to give an average cost per hour.
The costs of blood tests and other investigations were taken from the price charged by the relevant department to another NHS provider (the direct access price). The finance departments at the three hospitals also provided information on the total costs of consumables and overheads on the ward or department where CF patients were treated for the year from April 1999 to March 2000. The total costs were divided by the annual number of occupied bed days to give the costs per occupied bed day. Capital costs were not available from the finance departments concerned. These costs were therefore estimated from a secondary source.17
For outpatient and ward reviews a similar methodology was used for collecting unit costs. Drug costs were taken from the British National Formulary,4 and community care costs were from Netten et al.18 The maximum duration of drug usage within each therapeutic category was measured for each patient during each treatment period. For each intervention the costs of the nebuliser pot and compressor were included. All costs were adjusted to 1999–2000 prices using the hospital and community health services price index.19 Total costs for each treatment period were calculated by multiplying each patient’s resource use by the unit costs.
Statistical analysis
The sample size was calculated on the basis of change in FEV1 (primary clinical outcome).11 All analyses were undertaken according to a pre-specified statistical analysis plan on an intention to treat basis adjusted for baseline measurements. The analysis focused on two separate pairwise comparisons of treatments: daily rhDNase v HS and daily v alternate day rhDNase on the basis of within-subject differences. The primary analysis was of total healthcare costs but, in order to understand why differences in cost between the interventions might exist, mean differences in resource use were reported (with 95% confidence intervals). Due to skewed cost distributions, the 95% confidence intervals around the mean total cost differences between the treatment periods were calculated using non-parametric bootstrapping techniques.15
RESULTS
Forty eight children were randomised, eight to each of the six possible treatment orders. One 14 year old girl dropped out of the study almost immediately because of what became a prolonged illness. Table 1 gives the characteristics of the remaining 47 children as observed at the baseline assessment. Eight children were unable to complete all three treatment periods, so 43 children are included in the comparison of daily and alternate day rhDNase and 40 in the comparison of daily rhDNase and HS.
Baseline characteristics of the study population (n=47)
On the basis of returned treatment packs, the estimated adherence (average proportion of medication taken) was 84% for both daily and alternate day rhDNase and 93% for HS. Similar or higher proportions were obtained from the diary information.
Effectiveness
Following 12 weeks of treatment there was a mean (SD) increase in FEV1 from baseline of 16 (25)% in patients receiving daily rhDNase, 14 (23)% for alternate day rhDNase, and 3 (21)% for HS. Comparing mean FEV1 between the treatments, there was an advantage of 8% (95% CI 2 to 14, p=0.01) for daily rhDNase over HS but none for daily compared with alternate day rhDNase (2%, 95% CI –4 to 9, p=0.55). There was variation in individual responses to the treatments. Twenty six of the 40 children responded better with daily rhDNase than with HS. There was no evidence of difference in QOL nor in the occurrence of pulmonary exacerbations between the treatments.11
Resource use, unit costs, and healthcare costs
The mean total length of hospital stay, in particular resulting from pulmonary exacerbations, was higher during the HS treatment period than during the daily rhDNase period, and with alternate day than with daily rhDNase treatment (table 2). However, these differences were not statistically significant.
Comparison of mean healthcare use between the treatments. Each value represents the mean resource use per patient over each treatment period
The drug cost per day was £0.38 for HS, £20.39 for daily rhDNase, and £10.20 for alternate day rhDNase. The mean total cost of an occupied bed day ranged from £280 to £397, of an outpatient consultation from £51 to £84, and of a ward review from £67 to £148 (table 3). The unit costs were generally higher in the two postgraduate hospitals than in the DGH, mainly because of the higher costs of overheads and capital.
Mean unit costs (£) of hospital care for each of the study centres
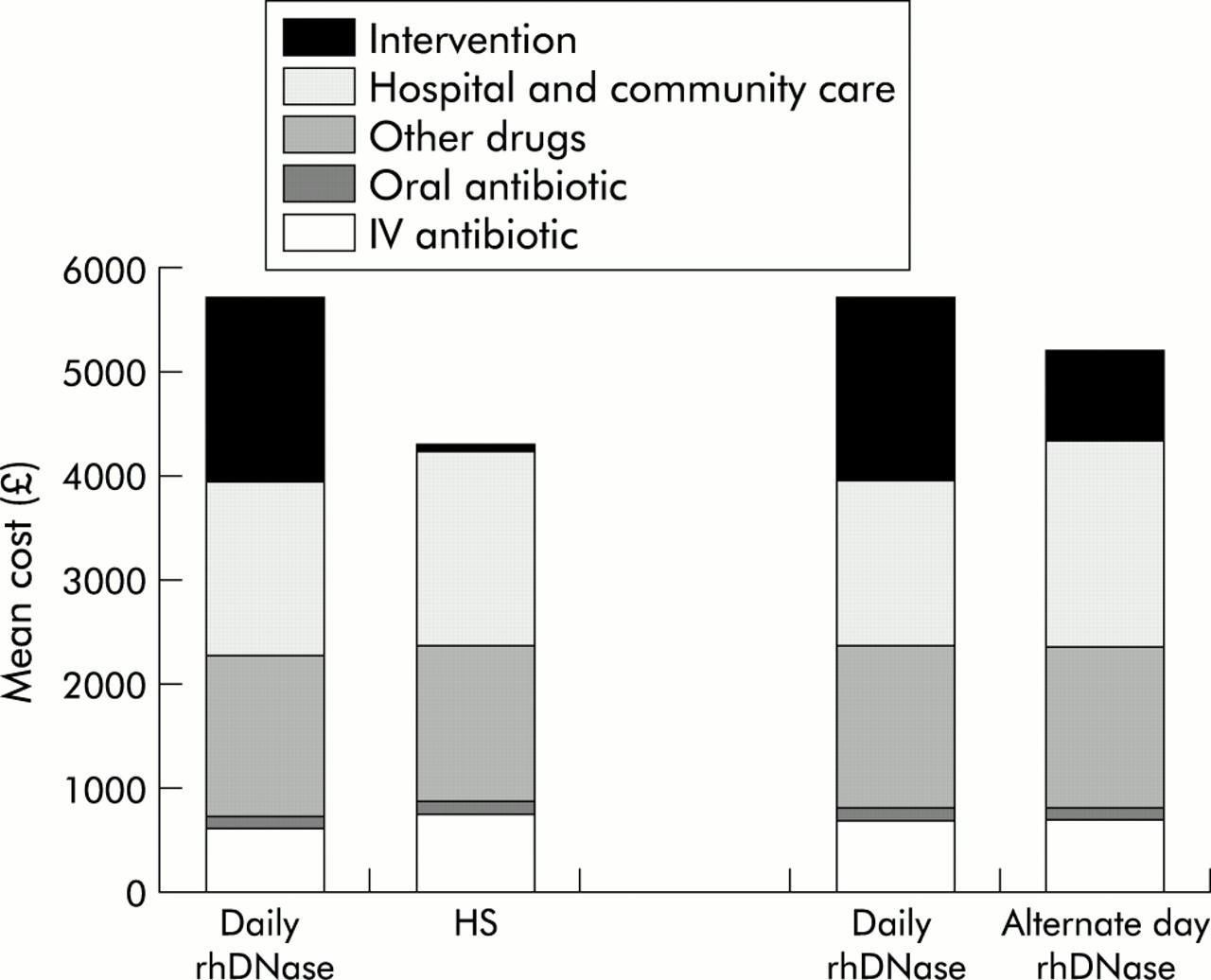
Over the 12 week treatment period the mean drug cost of daily rhDNase was £1755 compared with £37 for HS. The difference in the intervention cost was not offset by lower hospital and community care costs. Over 12 weeks the mean total health service cost for the daily rhDNase treatment period was £5694 compared with £4285 for HS, a mean difference of £1409 (95% CI £440 to £2318), table 4. In the comparison of daily and alternate day rhDNase treatment the lower hospital costs during daily rhDNase did not offset the increased intervention costs. The mean total costs during daily rhDNase were £5711 compared with £5198 during the alternate day treatment, a mean difference of £513 (95% CI –£546 to £1510), table 4. While the intervention costs were on average a higher proportion of total costs during the rhDNase periods, the costs of other resources—in particular antibiotic treatment and hospital and community care—were also important components of the total costs (fig 1).
Mean (%) costs (£) and percentages of total costs over each 12 week treatment period

{kind=link}
Mean total cost (£) of daily rhDNase compared with hypertonic saline (HS) and daily rhDNase compared with alternate day rhDNase.
Sensitivity analyses were carried out on the price of rhDNase which, in practice, may be lower than the British National Formulary price,4 and the cost per hospital day which may vary according to the setting considered. The analysis used the values from the 20th and 80th percentiles of the costs per occupied bed day from a UK national database.20 The results showed that, after reducing the rhDNase costs by 10% and 30%, the mean additional costs of rhDNase compared with HS fell to £1234 (95% CI £264 to £2204) and £884 (95% CI –£86 to £1855), and the mean additional costs of daily compared with alternate day rhDNase were £425 (95% CI –£594 to £1443) and £246 (95% CI –£771 to £1262). The results were insensitive to changes in the cost per bed day—for example, varying the cost per bed day from £187 to £120 meant that the incremental costs of daily rhDNase compared with HS ranged from £1548 (95% CI £982 to £2114) to £1521 (95% CI £845 to £2198).
DISCUSSION
This is the first UK study to examine in detail the healthcare resource use, costs, and outcomes associated with different mucoactive treatments for children with CF. The main findings were that treating patients with daily rhDNase compared with HS resulted in a mean improvement in FEV1 of 8% at a mean additional cost of £1409 over a 12 week period. Administering rhDNase on an alternate day as opposed to a daily basis was shown to be as effective, and had lower average costs of £513 over 12 weeks. If these cost differences were maintained over a year, then alternate day rhDNase may lead to annual savings of a mean of £2223 per patient.
The two previous short term clinical trials of HS have reported greater improvements in mean FEV1 than our study.9,10 Both studies administered a larger volume of HS (10 ml). Ultrasonic nebulisers, which were used in the study by Eng et al,9 delivered a larger volume over a shorter period of time, but are not recommended for rhDNase21 and are generally not used for domiciliary therapy in CF. Ballmann et al10 reported that 10 ml of HS nebulised twice a day by jet nebuliser took about 84 minutes to administer. This long inhalation time was unacceptable to the patients and the authors suggested that, if this regime was instituted as permanent therapy, there would be problems with adherence. Our trial needed to be pragmatic so a volume of 5 ml 7% HS was used which takes about 10 minutes to administer by jet nebuliser. However, the lack of benefit from HS in this study may have resulted from the low dose delivered and the resultant lack of significant change in osmolality of airway surface fluid.
The changes in FEV1 caused by rhDNase in our study were greater than those reported in the 6 month long phase III study by Fuchs et al.3 However, they were similar to changes seen in the short term phase II rhDNase trials.2,22 Fuchs et al3 have shown that patients who respond to rhDNase show an initial marked improvement in FEV1 which subsequently declines over the first few months to remain stable at a lower level.
An important aspect of our study was that, in keeping with the general guidelines on economic evaluation, it took a broad perspective to resource use measurement. This meant it was possible to assess whether the costs of rhDNase were offset by savings in hospital and community health services, or in the use of other drugs. Oster et al6 in a previous economic evaluation of rhDNase hypothesised that health service cost savings would offset one third of the cost of the drug. Furthermore, a recent US study suggested that prolonged use of rhDNase may reduce the costs of respiratory disease related care in patients with CF.23 Our study did not provide any strong evidence that daily rhDNase reduced the rate of inpatient admissions or the duration of intravenous antibiotics compared with HS. However, it suggested that the length of stay for pulmonary exacerbations (the primary reason for admission) was on average 1.95 days longer following HS than daily rhDNase, although the confidence intervals around the estimate were wide and the difference was not statistically significant.
A key determinant of the incremental costs of the rhDNase strategies was the cost of the drug itself. The unit cost of the drug was taken from the British National Formulary,4 which is recommended practice for reporting results in a generalisable way. However, if providers can negotiate a lower price for rhDNase, the incremental cost falls proportionately. By contrast, the sensitivity analysis showed that the results were reasonably robust to the particular cost per day used for a hospital provider.
Adherence to alternate day rhDNase and daily rhDNase was similar. Despite the need for twice daily administration, adherence to HS was surprisingly good. It did not appear that patients were more adherent to daily rhDNase, despite them knowing that it was a more expensive treatment. However, the impact of adherence on cost-benefit analyses remains unclear. For the rhDNase treatment periods only about 84% of the prescribed doses were actually administered. The fact that the patient did not administer all the prescribed doses may not actually reduce the cost of treatment, particularly if the doses not used are thrown away.
This study did not take a societal perspective and measure the relative costs to the patient and the family. The finding that community service use in particular was very similar between the groups suggests that taking a broader perspective would have been unlikely to change the results. Resource use directly attributable to the administration of the trial was excluded from the analysis. The only outstanding “trial effect” may be that, in the trial, patients substituted attendance at postgraduate hospital clinics for DGH clinic visits. This effect is unlikely to vary between the treatment arms, so the impact on the incremental costs of the rhDNase therapy is likely to be negligible. However, the length of follow up was only 12 weeks, so any improvements in lung function from the rhDNase therapy which led to reductions in resource use after this period were not included. Nevertheless, in the study by Oster et al6 the maximum difference in the cumulative incidence of respiratory tract infection (the main reason for hospital admission) occurred after 4 weeks of treatment.
The detailed approach to costing meant that resource use and total cost were measured for each patient, so it was possible to report mean effect sizes with 95% confidence intervals for the parameters of interest. The difference in the total cost of alternate day and daily rhDNase of £513 over 12 weeks, which may be regarded as important from a decision maker’s viewpoint, was not found to be statistically significant. For the observed difference in costs to have been statistically significant, about four times as many patients would have been required. This illustrates the general concern in economic evaluations alongside randomised controlled trials that the sample size may be too small to detect differences in economic end points reliably. This problem usually arises because the sample size is calculated, as in this study, to detect a clinically significant difference in the primary efficacy outcome measure.
By using a crossover trial it was important to ensure that there was no carry over effect. However, the power to detect treatment by period interactions in a crossover study is very limited. It is therefore recommended by several authors24,25 that the best protection against such carry over effects is to ensure that the washout period is sufficiently long. The 2 week washout period used in this trial was based on that used in previous studies.2,9
The evidence from this study needs to be supported by further research to assess the long term costs and consequences of the respective strategies, in particular to examine the relative use of hospital resources for larger groups of patients over a longer period of time. Future studies may benefit from specifying in advance what constitutes an important difference in total cost, and then using measures of variability from this study to perform sample size calculations. Nevertheless, these results give decision makers comparative information on different treatment strategies for children with CF. Given the pressure on NHS resources, it would seem important that new high cost interventions such as nebulised TOBI (Chiron, Emeryville, California, USA) are evaluated using the same framework before their widespread use is recommended in the UK.
In conclusion, our study found that daily rhDNase was more effective than HS, but increased costs by £1409 over 12 weeks. Administering rhDNase on an alternate day rather than a daily basis was as effective and had potential cost savings of £513 over a 12 week period.
Acknowledgments
The authors are grateful for the contribution of Marcus Flather, Belinda Lees, and Pauline Dooley from the Clinical Trials and Evaluations Unit, the Royal Brompton Hospital for their considerable contribution to the original study and their assistance with randomisation, database design and management. They would also like to thank the CF teams at the Royal Brompton Hospital and Great Ormond Street Hospital.
REFERENCES
Footnotes
-
This study was funded by the NHS Health Technology Assessment Programme.