

Abstract
BACKGROUND: Patients with cystic fibrosis develop decreased exercise capacity. However, the main factors responsible for this decline are still unclear. Thus, the objective of this study was to evaluate the factors influencing exercise capacity assessed with the modified shuttle test (MST) in individuals with cystic fibrosis.
METHODS: A cross-sectional study was carried out in subjects with a diagnosis of cystic fibrosis who were 6–26 y old and were regularly monitored at 2 cystic fibrosis reference centers in Brazil. Individuals who were unable to perform the tests or who exhibited hemodynamic instability and exacerbation of respiratory symptoms were excluded. Anthropometric, clinical, and genotype data were collected. In addition, lung function and exercise capacity were evaluated with the MST.
RESULTS: 73 subjects (mean age 12.2 ± 4.9 y and FEV1 76.8 ± 23.3%) were included. The mean distance achieved in the MST was 765 ± 258 m (71.6% of predicted). The distance achieved on the MST correlated significantly with age (r = 0.49, P < .001), body mass index (r = 0.41, P < .001), resting heart rate (r = −0.51, P < .001), and FEV1 (r = 0.24, P = .042). Subjects with FEV1 > 67% of predicted (P = .02) and those with resting heart rate < 100 beats/min (P = .01) had a greater exercise capacity. Resting heart rate, age, and FEV1 (%) were found as significant variables to explain the distance achieved on the MST (R2 = 0.48, standard error = 191.0 m).
CONCLUSIONS: The main determinants of exercise capacity assessed with the MST in individuals with cystic fibrosis were resting heart rate, age, and lung function.
Introduction
Cystic fibrosis is a disease caused by genetic mutations in the long arm of chromosome 7. These mutations are grouped in different classes, and the most common is F508del, which occurs in 50–70% of patients.1 The multisystemic characteristic of the disease leads to progressive loss of lung function and physical exercise intolerance.2 Exercise capacity is known to be associated with mortality in patients with cystic fibrosis and individuals with reduced oxygen consumption (peak  ), with values below 45 mL/kg/min (82% of predicted) presenting 4.9 times higher risk for a fatal outcome in an 8-y follow-up period.3
), with values below 45 mL/kg/min (82% of predicted) presenting 4.9 times higher risk for a fatal outcome in an 8-y follow-up period.3
The precise mechanisms of exercise intolerance in young patients with cystic fibrosis are still controversial and appear to be influenced by several factors, including age, sex, nutritional status, lung function, genotype, chronic colonization by Pseudomonas aeruginosa, endurance and strength of the respiratory muscles.4–8 However, recently, a multicenter study demonstrated that genotype severity was not associated with exercise capacity as assessed with the cardiopulmonary exercise test, but was associated with lower lung function and poor nutritional status.6
On the other hand, the accepted standard evaluation of peak  (ie, cardiopulmonary exercise testing) is still not available in most cystic fibrosis centers due to the need for equipment and staff with expertise to perform the gas analysis test. Therefore, the modified shuttle test (MST) has been validated for use in individuals with cystic fibrosis, and the MST is suggested as an alternative for the evaluation and monitoring of the exercise capacity, considering that the distance achieved on the test presents a strong correlation with peak
(ie, cardiopulmonary exercise testing) is still not available in most cystic fibrosis centers due to the need for equipment and staff with expertise to perform the gas analysis test. Therefore, the modified shuttle test (MST) has been validated for use in individuals with cystic fibrosis, and the MST is suggested as an alternative for the evaluation and monitoring of the exercise capacity, considering that the distance achieved on the test presents a strong correlation with peak  measured through cardiopulmonary exercise testing.9–11
measured through cardiopulmonary exercise testing.9–11
Thus, considering the importance of identifying the mechanisms associated with exercise intolerance, this study aimed to evaluate the factors that influence exercise capacity assessed with the MST in individuals with cystic fibrosis. For that, subjects were submitted to a MST, and the associations with clinical and demographic data, lung function, and nutritional status were evaluated.
QUICK LOOK
Current knowledge
The precise mechanisms of exercise intolerance in children and adolescents with cystic fibrosis are still controversial, but they appear to be influenced by several factors, including age, sex, nutritional status, lung function, genotype, chronic colonization by P. aeruginosa, and endurance and strength of respiratory muscles. Cardiopulmonary exercise testing is not available in most cystic fibrosis centers due to the need for equipment and staff with expertise to perform the test.
What this paper contributes to our knowledge
The determinants of exercise capacity assessed with the modified shuttle test in children and adolescents with cystic fibrosis were resting heart rate, age, and lung function. Measurement of resting heart rate, used in conjunction with age and FEV1, may be a complementary tool for evaluation and follow-up of patients with cystic fibrosis during out-patient visits because it is simple and easy to perform.
Methods
A cross-sectional study was carried out in subjects with cystic fibrosis (diagnosis confirmed with a genetic test),12 who were 6–26 y old and were regularly monitored at 2 reference centers (Hospital São Lucas, Pontifícia Universidade Católica do Rio Grande do Sul and Hospital Infantil João Paulo II, Pontifícia Universidade Católica de Minas Gerais – Campus Betim) for cystic fibrosis treatment. Individuals with hemodynamic instability, exacerbation of respiratory symptoms (eg, fever, increased coughing, sputum production) on the day of the test, or osteoarticular or musculoskeletal abnormalities that would potentially influence the tests were excluded.
Subjects were recruited during an out-patient visit and performed the MST on the same day. Spirometry was performed by trained staff members, which is routine for both treatment centers. In addition to the tests, anthropometric, clinical, and genetic data were collected, including the type of mutation and chronic colonization by P. aeruginosa. Chronic colonization by P. aeruginosa was defined as the persistent presence of the bacterium in the oropharynx swab or sputum culture for at least 6 months or in 3 consecutive collections.13 Mutations were classified into 3 categories: F508del homozygote, F508del heterozygote, and other mutations.
The sample size was estimated based on the relationship between the main variables demonstrated in the study by Doeleman et al.8 To identify a minimum correlation of 0.40, with a power of 90% and significance level of 5%, a minimum sample of 62 subjects was estimated. The study was approved by the Research Ethics Committee of both centers (52583416.5.0000.5336, 54142716.8.3001.5119). All legal guardians and subjects over the age of 18 y signed the informed consent term. Moreover, children and adolescents under the age of 18 y signed the assent form.
Anthropometric Data
Weight and height measurements were performed in triplicate or until 2 identical values were obtained. Weight was measured in the orthostatic position, with the minimum of clothing and without footwear, with the use of a digital scale (G-tech, Glass 1 FW, Rio de Janeiro, Brazil) previously calibrated with a precision of 100 g. Height was obtained with a portable stadiometer (AlturaExata, TBW, São Paulo, Brazil) with a precision of 1 mm, with subjects barefoot, feet parallel, ankles together, and arms extended along the body.14 Individuals were classified as malnourished and eutrophic according to World Health Organization (WHO) recommendations.15 The WHO Anthroplus program was used to calculate body mass index z-scores.16
Modified Shuttle Test
The MST was performed as described by Bradley et al.11 This test has 15 levels, and patients should walk or run, when necessary, with increasing speeds on a 10-m course delimited by 2 cones (ie, a cone at each end of the course) that must be circumvented by the individual. An audio signal is an integral part of the test, representing a level change as well as the speed increase during the test. The subjects were followed up by the physiotherapist during the first minute for adaptation to the rhythm of the audio signal. The test protocol begins with an average speed of 0.5 m/s (level 1), followed by an increment of 0.17 m/s at each subsequent level. At the end of each level, a standardized verbal encouragement was offered for the subjects to walk faster, as well as guidance to complete the total duration of the test. Before the start of the test and immediately at the end, the heart rate,  (Nonin, Minneapolis), blood pressure (BIC sphygmomanometer, Itupeva, Brazil), and the modified BORG scale score for dyspnea were measured. In addition, heart rate and
(Nonin, Minneapolis), blood pressure (BIC sphygmomanometer, Itupeva, Brazil), and the modified BORG scale score for dyspnea were measured. In addition, heart rate and  were monitored throughout the test.
were monitored throughout the test.
The test was completed when the subject reported an inability to continue due to exhaustion, lost the rhythm of the audio signal for 2 consecutive times, reached a maximum distance of 1,500 m, or presented  < 75%. The distance achieved was calculated by counting the total number of shuttles at the end of the test and expressed in meters and percent of predicted.17 The peak
< 75%. The distance achieved was calculated by counting the total number of shuttles at the end of the test and expressed in meters and percent of predicted.17 The peak  was estimated by the following equation:
was estimated by the following equation:  (mL/kg/min) = 20.301 + 0.019 × MST distance (m).10
(mL/kg/min) = 20.301 + 0.019 × MST distance (m).10
Lung Function
The assessment of lung function was performed with subjects in the orthostatic position, without the use of a nasal clip.18 All acceptability and repeatability criteria followed the recommendations of the American Thoracic Society and European Respiratory Society.19 FVC, FEV1, FEV1/FVC, and the forced expiratory flow during the middle half of the FVC maneuver (FEF25-75%) were evaluated. Data were expressed in absolute values and percentage of predicted, based on an international reference equation.20 For some of the analyses, the sample was divided into 2 groups: FEV1 < 67% predicted and FEV1 > 67%. According to Doeleman et al,8 subjects with moderate-to-severe cystic fibrosis (FEV1 < 67%) present a strong association between lung function and distance achieved on the MST.
Statistical Analysis
The distribution of the variables was assessed using the Kolmogorov-Smirnov test. As a normal distribution was found, the continuous variables were presented as mean ± SD. Categorical variables were presented in absolute and percentage frequencies. Correlations were assessed using a Pearson linear correlation test and classified as weak (r < 0.4), moderate (r ≥ 0.4 and < 0.7), and strong (r ≥ 0.7). A Student ttest for independent samples was used for comparisons of the MST distance between different lung function, nutritional status, and resting heart rate. One-way analysis of variance with least significant difference post-test was used for comparisons of lung function, nutritional status, and distance achieved on MST between the distinct genotype categories. A multiple linear regression model was used to evaluate the influence of the variables on the distance achieved on the MST. Variables presenting the highest correlation coefficient (r) with the MST distance were included in the analysis. Considering that the majority of our sample are children and adolescents, body mass index was selected to assess nutritional status instead of height and weight. Variable selection was performed using the forward stepwise method. Only the model with the highest coefficient of determination (R2) is presented.21 All analyses and data processing were performed with SPSS 18.0 (IBM, Armonk, New York), and the level of significance adopted was P < .05.
Results
A total of 73 subjects with a mean age of 12.2 ± 4.9 y were included; of the subjects, 65.8% were male and 57.5% were heterozygous for the F508del mutation. Regarding lung function, the mean percentage of predicted FEV1 was 76.8 ± 23.6 and FVC was 84 ± 20.6. The characteristics of the sample are presented in Table 1. The physiological variables evaluated at rest and at the end of the MST are shown in Table 2. The mean heart rate (beats/min) was 94 ± 15 at rest and 178 ± 17 at the end of the test. The mean level reached during the MST was 11 ± 2, and the average distance reached was 765 ± 258 m, corresponding to 71.6 ± 20.8% of the predicted distance. In addition, the estimated mean peak  was 34.8 ± 4.9 mL/kg/min.
was 34.8 ± 4.9 mL/kg/min.
Characterization of the Study Sample
Resting Characteristics and Physiological Responses to the Modified Shuttle Test
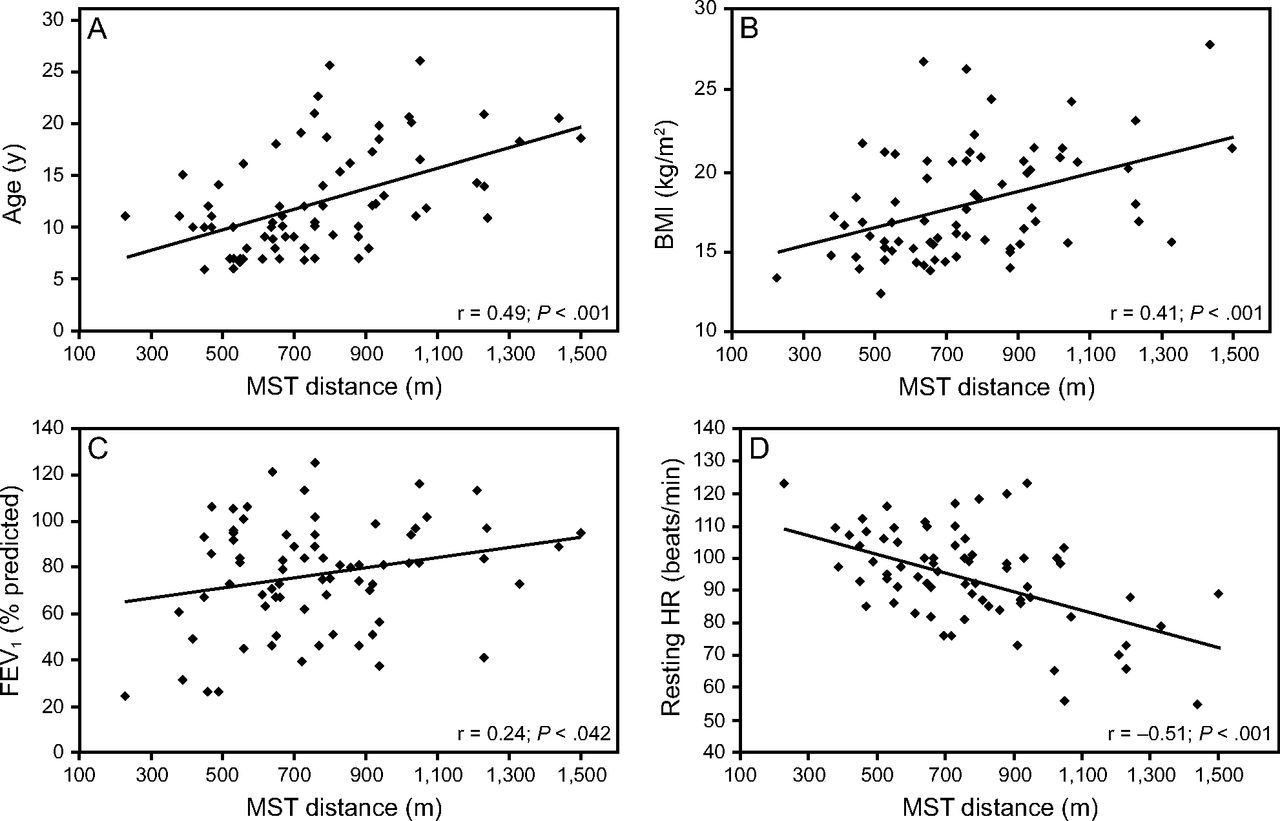
Figure 1 shows the distance achieved on the MST correlated significantly (P < .001) and moderately with age (r = 0.49), body mass index (r = 0.41), and resting heart rate (r = −0.51). In addition, we found a significant and weak correlation with percentage of predicted FEV1 (r = 0.24). Data presented in Figure 2 show the distance achieved on the MST according to FEV1, body mass index, and resting heart rate. No differences were found regarding nutritional status. On the other hand, lung function (P = .02) and resting heart rate (P = .01) significantly influenced the MST distance because subjects with FEV1 < 67% of predicted (661 ± 235 m) and those with resting heart rate > 100 beats/min (665 ± 206 m) exhibited lower exercise capacity, as evidenced by the decreased distance covered on the MST.

Correlation between the distance achieved in the modified shuttle test (MST) and (A) age, (B) body mass index (BMI), (C) FEV1, and (D) resting heart rate (HR).

Comparison of the distance achieved in the modified shuttle test (MST) between (A) eutrophic and undernourished subjects, (B) subjects with FEV1 above or below 67% predicted, and (C) subjects with resting heart rate above or below 100 beats/min. * significant differences (P < .05).
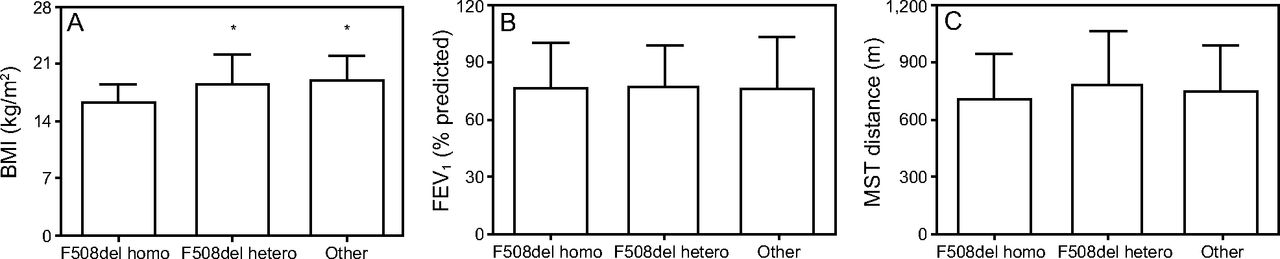
There was no influence of genotyping on the distance achieved on the MST or on lung function. However, there were significant differences for body mass index, both when the F508del homozygote was compared to the F508del heterozygote (mean difference −2.4, P = .01) and to other mutations (mean difference −2.6, P = .038). These data are presented in Figure 3.

Comparison of (A) body mass index (BMI), (B) FEV1, and (C) distance achieved in the modified shuttle test (MST) between different genotype categories. * significant differences (P < .05) when compared to the F508del homozygote group.
The results of the multiple linear regression analysis for the determinants of the distance achieved on the MST are presented in Table 3. The variables of gender, age, chronic colonization by P. aeruginosa, body mass index, FEV1 (% of predicted), FVC (% of predicted), and resting heart rate were included in the analysis. The results showed that only resting heart rate, age, and FEV1 (% predicted) were significant to explain the distance achieved on the MST, with a R2 = 0.48 and a standard error of the estimate of 191.0 m. The standardized beta coefficient for resting heart rate, age, and FEV1 were −0.328, 0.490, and 0.290, respectively.
Multiple Linear Regression Model for Predicting the Distance Achieved on the Modified Shuttle Test
Discussion
This study aimed to identify factors that may influence exercise capacity assessed by the MST in young subjects with cystic fibrosis. The results showed that resting heart rate is one of the main determining factors for the distance achieved on the MST, along with age and lung function. On the other hand, genotyping appeared to have no significant influence on exercise capacity.
Resting heart rate has been used as an important indicator of physical fitness and clinical prognosis in subjects with heart disease.22 Aerobic training performed with submaximum workloads reduces heart rate at rest and during exercise.22 In addition, a study with healthy adolescents showed that aerobic fitness is associated with resting heart rate, indicating that lower aerobic fitness is associated with higher heart rate values at rest.23 Sarganas et al24 reported an association of resting heart rate with aerobic capacity in adolescents aged 11–17 y. Our data indicate a moderate correlation between resting heart rate and distance achieved on the MST. However, resting heart rate was the main variable found to explain the distance achieved on the MST (R2 = 0.26). To our knowledge, this is the first study to report that resting heart rate is a significant determinant of exercise capacity in young individuals with cystic fibrosis, and it may be a clinical marker when used in conjunction with other variables because its evaluation is simple.
Age and FEV1 (% of predicted) were also determinants of exercise capacity according to the data of the present study. Similarly, Doeleman et al8 reported that these variables could explain 64% of the distance on the MST in adults with cystic fibrosis, although that model also included gender. In the study by Pastré et al,25 the variables found to be predictors of peak  in adult subjects with mild to moderate pulmonary disease were FEV1 (% of predicted), ventilatory equivalent for carbon dioxide production, and ventilatory reserve, accounting for 67% of exercise capacity. Our results indicate a weak correlation between the distance covered on the MST and FEV1 (% of predicted), contrary to the moderate correlation that was reported in previous work.11,26 In addition, Doeleman et al8 noted a strong correlation only when subjects with a FEV1 < 67% of predicted were analyzed. Thus, when data from the present study was categorized as FEV1 < 67% or > 67% of predicted, we noted that subjects with FEV1 < 67% of predicted achieved a significantly lower distance on the MST. It is possible that the poor correlation found in our study may be explained by the fact that the included sample was young and presenting mildly compromised pulmonary function.
in adult subjects with mild to moderate pulmonary disease were FEV1 (% of predicted), ventilatory equivalent for carbon dioxide production, and ventilatory reserve, accounting for 67% of exercise capacity. Our results indicate a weak correlation between the distance covered on the MST and FEV1 (% of predicted), contrary to the moderate correlation that was reported in previous work.11,26 In addition, Doeleman et al8 noted a strong correlation only when subjects with a FEV1 < 67% of predicted were analyzed. Thus, when data from the present study was categorized as FEV1 < 67% or > 67% of predicted, we noted that subjects with FEV1 < 67% of predicted achieved a significantly lower distance on the MST. It is possible that the poor correlation found in our study may be explained by the fact that the included sample was young and presenting mildly compromised pulmonary function.
The results of this study did not indicate an association between genotype and exercise capacity in individuals with cystic fibrosis. These data corroborate results of studies by Kaplan et al,27 Van de Weert-van Leeuwen et al,7 and the recent multi-center study by Radtke et al,6 which did not identify any influences of the type of genetic mutation on peak  . On the other hand, as expected, body mass index was worse in subjects homozygous for F508del. However, this association of genotype with body mass index was reported previously.6
. On the other hand, as expected, body mass index was worse in subjects homozygous for F508del. However, this association of genotype with body mass index was reported previously.6
One limitation of this study is the fact that the levels of daily physical activity of the subjects were not measured, which prevented us from evaluating the influence of this variable on exercise performance. However, all individuals received a recommendation for physical exercise, which is a standard guideline for all patients followed at both referral centers. It is also worth noting that the final standardized error of the estimation may be considered high, so, although results were valuable to identify the main exercise capacity determinants, values may not be used to estimate the MST distance.
Conclusions
The results of this study indicate that the determinants of exercise capacity assessed with the MST in young individuals with cystic fibrosis are the resting heart rate, age, and lung function. Measurement of resting heart rate, used in conjunction with age and FEV1, may be a complementary tool for evaluation and follow-up of patients with cystic fibrosis during out-patient visits because it is a simple and easy-to-perform method.
Footnotes
- Correspondence: Márcio Vinícius Fagundes Donadio PT PhD, Laboratory of Pediatric Physical Activity, Centro Infant, Av. Ipiranga, 6690, 2° andar, Porto Alegre, Rio Grande do Sul, CEP 90610–000, Brazil. E-mail: mdonadio{at}pucrs.br
The authors have disclosed financial support from Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (finance code 001), Conselho Nacional de Desenvolvimento Científico e Tecnológico, and Fundo de Incentivo à Pesquisa da PUC Minas (FIP 11009-S2) .
- Copyright © 2020 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}