

Abstract
BACKGROUND: As the use of intravenous magnesium sulfate (MgSO4) for the treatment of refractory asthma is becoming more common, the incidence of MgSO4-related systemic hypotension is also rising. One option is to deliver MgSO4 via aerosol, but compared to most inhaled medications, which are active in the microgram dose range, the MgSO4 dose requirement is in the milligram range. This, along with inefficient aerosol delivery systems, may be the reason that some studies have found lack of efficacy with aerosol MgSO4. In preparation for a multicenter study of inhaled MgSO4 in asthmatic children 2–17 years old, we conducted an in vitro study to choose the best MgSO4 nebulizer system that would be effective over the entire age range.
METHODS: We tested the Pari LC Star jet nebulizer, Omron MicroAir vibrating-mesh nebulizer, and the Aeroneb Go vibrating-mesh nebulizer with the Idehaler valve-less holding chamber. Aerosol delivery was via face mask.
RESULTS: The Pari LC Star had an appropriate particle size distribution but a very slow aerosol output rate. The Omron MicroAir had an even slower output rate and a larger particle size distribution, which would be inappropriate for smaller children. In vitro lung deposition with the Aeroneb Go with Idehaler was 16.0 ± 0.4 mg/min in older children and approximately a fifth of that in toddlers.
CONCLUSIONS: The Aeroneb Go with Idehaler was chosen for the multicenter clinical study.
Introduction
Despite extensive research, standard stabilization therapy for pediatric acute asthma1,2 has not substantially improved outcomes.3 Since many patients do not respond to inhaled β2 agonists,4 and delayed response to corticosteroids is common, the hospitalization rate has remained stable and the related costs are increasing.5 Two recent meta-analyses found that intravenous magnesium sulfate (MgSO4) decreases asthma hospitalization in children by 30%,6,7 and MgSO4 is thus recommended in children with severe asthma resistant to initial bronchodilator therapy.6,8 However, intravenous MgSO4 is invasive and requires monitoring for adverse effects. A recent North American survey found that intravenous MgSO4 is uncommonly used, usually to prevent ICU admission rather than hospitalization, and one in 4 physicians have observed the adverse effect systemic hypotension.9
In contrast, the inhalation route is noninvasive and offers the advantage of targeted delivery to the lower airways and less potential for toxicity.10 Although 2 meta-analyses found a trend toward less hospitalization with nebulized MgSO4,6,11 others disagree.12 The key limitation is the use of inefficient aerosol delivery methods. None have used the more efficient delivery devices, such as breath-enhanced nebulizer, with which the patient inhales through a mouthpiece, or other efficiency-enhancing techniques. Unlike most aerosolized drugs, such as albuterol, which is efficacious in the microgram range, MgSO4, even when given intravenously, is only efficacious in the milligram range and hence requires many-fold higher drug delivery, and there is a physical limitation of the nebulizable volume. Increasing the MgSO4 concentration would increase the delivery rate but is limited by the acceptable aerosol tonicity of approximately 500 mOsm/L.13
With intravenous MgSO4 the greatest lung tissue exposure is in the alveoli, where the vessel wall is the thinnest and the perfusion per gram of tissue is greatest. To reach the airway smooth muscle, intravenous MgSO4 has to diffuse from the thicker-walled pulmonary arteries and arterioles or from the bronchial circulation, which is very small compared to the pulmonary circulation. In contrast, most inhaled MgSO4 would be deposited in the airways, and subsequent direct diffusion through the airway epithelium would result in a much higher magnesium level around the smooth muscle, compared to intravenous administration. Therefore, while the systemically delivered dose of nebulized MgSO4 would probably be lower than with the intravenous route and result in less risk of hypotension, the increased delivery to the airway muscles could result in a similar or greater bronchodilator effect.
The purpose of this pilot study was to investigate the expected MgSO4 pulmonary deposition of efficient modern nebulizers and to choose a nebulizer for a planned multicenter trial of nebulized MgSO4 in pediatric acute asthma in the pediatric emergency department setting. Ideally, a comparison would be made to devices used in other studies, but insufficient details regarding the equipment used made that impossible. To power the clinical study sufficiently to give confidence in the results and to keep the budget within reason, it is essential to use the same aerosol delivery system with all subjects, regardless of age. This necessitates the use of a face mask, since the younger subjects (based on emergency utilization data) are likely to be the largest group. This constraint limited the full potential of breath-enhanced nebulization, which requires a mouthpiece and both inspiratory and expiratory valves.
Methods
The study was conducted at the Hospital for Sick Children, Toronto, Ontario, Canada.
We tested 3 aerosol systems:
Aeroneb Go vibrating-mesh nebulizer (Aerogen, Galway, Ireland) with Idehaler holding chamber (La Diffusion Technique, Francaise, St Etienne, France), adapted for use with a face mask. There are no inspiratory or expiratory valves in this system, but the geometry favors aerosol retention during expiration, and then inhalation of both the retained and the generated aerosol during the subsequent inspiration. Given the necessity of using a loose-fitting face mask, preliminary tests suggested that this would be more efficient than other devices. From the investigative perspective, one disadvantage of this valveless system is that adding an expiratory valve to capture aerosol generated but not inhaled would change the fluid dynamics. This precluded a mass balance to determine the accuracy of the measurements.
MicroAir vibrating-mesh nebulizer (Omron, Kyoto, Japan), used with a face mask. We chose the MicroAir because it has a relatively high aerosol output rate.
Pari LC Star jet nebulizer (Pari, Munich, Germany), which is a high-efficiency breath-enhanced nebulizer14,15 when used in this mode, but less efficient when attached to a mouthpiece. We decided to drive this nebulizer with dry hospital oxygen, because that is what would probably be used clinically. This gave rise to the challenge of choosing a concentration that would allow effective delivery yet have an osmolarity that would not cause bronchospasm, which has been reported when the osmolarity exceeds 500 mOsm/L.13 The Pari LC Star has been extensively studied in our laboratory, and its characteristics are well known,14,15 although there was concern about its output rate in the non-breath-enhanced mode that occurs when using a face mask.
For the purpose of this study, we diluted 2 mL of MgSO4 solution (500 mg MgSO4 per mL, Sandoz, Montreal, Québec, Canada) in 7 mL of sterile water, then added 1 mL of albuterol solution (5 mg albuterol per mL, Ventolin Respiratory Solution, GlaxoSmithKline, Montreal, Canada) to give a final solution of 100 mg/mL of MgSO4 and 500 μg/mL of albuterol, with an osmolarity of 372 mOsm/L. We charged each nebulizer with 6 mL of that solution. Preliminary data from the Pari LC Star showed both a relatively low aerosol output rate and, because of evaporative loss, an increasing concentration (see below) in the nebulizer reservoir during nebulization. This resulted in higher-than-desired tonicity,16,17 so the Pari LC Star was not considered further. Neither of the vibrating-mesh nebulizers have a change in osmolarity during nebulization, because the liquid in the reservoir is not exposed to air until it is nebulized.
An inspiratory filter captured the “inhaled mass” at the device's output (Fig. 1). Since neither the MicroAir nor the Aeroneb Go/Idehaler system has valves, aerosol was drawn through the filter during inspiration and vented into the room during expiration. The inspiratory filter was at the “mouth” of a breath simulator set to a typical adult breathing pattern of 15 breaths/min, a tidal volume of 0.6 L, and a ratio of inspiratory time to total respiratory cycle time (TI/Ttot) of 0.4.15,18 On the assumption that the solution of MgSO4 would track with the solution of albuterol, we considered the “inhaled mass” the aerosol collected on and eluted from the filter and quantified via spectrophotometry.19 Assuming that the deposition of MgSO4 was proportional to the deposition of albuterol on the inspiratory filter, we calculated the rate of MgSO4 deposition. We repeated the test with values representative of a small child20: tidal volume 100 mL, respiratory rate 15 breaths/min, and TI/Ttot 0.4. Particle size distribution was measured via laser diffraction (Mastersizer X, Malvern Instruments, Worcestershire, United Kingdom) based on the Mie theory.21 The volume median diameter is the diameter where 50% of the aerosol volume is greater than this and 50% less. Particles ≤ 5 μm diameter are likely to deposit in the lungs when inhaled in older children and adults22–25 Hence, the fraction of the mass of the aerosol in this size range is known as the respirable fraction. When the amount of aerosol captured on the filter at the “mouth” over a specific time period is multiplied by the respirable fraction, the pulmonary deposition in mg/min can be estimated.15 There is evidence20,26 that in younger children the respirable fraction is more appropriately defined as ≤ 4 μm, and in infants ≤ 3 μm.
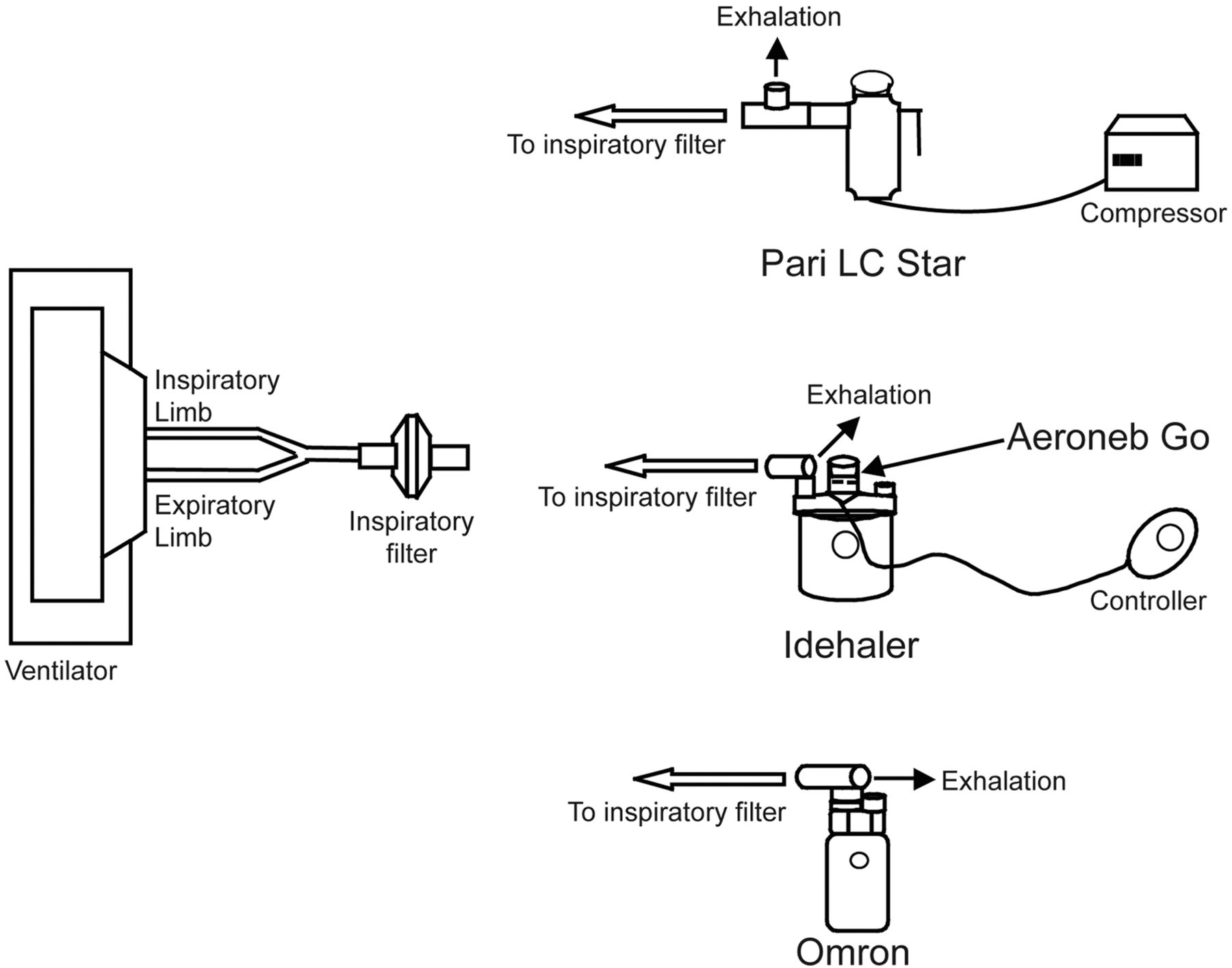
Setup for bench-testing nebulization of MgSO4-plus-albuterol solution with the Pari LC Star, Omron MicroAir, and Aeroneb Go with Idehaler holding chamber.
Results
With the 6 mL fill, the nebulization time with the Aeroneb Go/Idehaler system was 16.4 ± 0.7 min, and the mean ± SD aerosol output rate was 37.1 ± 1.5 mg/min. The MgSO4 volume median diameter was 4.4 ± 0.1 μm, and the respirable fraction was 59 ± 0% with a ≤ 5-μm cut-off, 44 ± 1% with a ≤ 4-μm cut-off, and 28 ± 2% with a ≤ 3-μm cutoff. With the adult breathing pattern the mean ± SD inhaled mass was 27.1 ± 0.6 mg/min (n = 3), which yields a predicted deposition of 16.0 ± 0.4 mg/min, based on a respirable-fraction cut-off of ≤ 5 μm for older children and adults. With an albuterol-to-MgSO4 ratio of 1:200, this would mean a pulmonary deposition of 80 μg/min. The recommended maximum intravenous infusion of albuterol in our institution is 10 μg/kg/min, so the pulmonary dose would be within that range for any child larger than 10 kg, assuming 100% delivery and absorption which, in reality, is far from the case. For an adult of 70 kg the MgSO4 deposition would be 0.23 mg/kg/min.
In a previous study20 of a measles vaccine delivered via nebulizer and face mask, algorithms were developed to look at expected deposition over a wide age range, taking into consideration that both the breathing pattern and the respirable fraction are age-dependent. Based on those algorithms, for the toddler breathing pattern the inhaled mass was 11.3 ± 0.2 mg/min with a pulmonary delivery estimate of 3.2 ± 0.1 mg/min. Therefore a child of 10 kg would have a deposition of 0.32 mg/kg/min.
For the adult breathing pattern, the other 2 devices came nowhere near that pulmonary deposition rate. The Pari LC Star delivered an estimated 9.0 ± 0.3 mg/min, and the osmolarity at the end of nebulization exceeded 500 mOsm/L, which is above the suggested safety limit.13 The particle size distribution was acceptable, with a respirable fraction of 67 ± 0%. The MicroAir delivered only 6.6 ± 0.7 mg/min to the filter at the “airway” and had a respirable fraction of only 46 ± 1%, for an estimated deposition of 3.1 ± 0.3 mg/min in adults and older children.
Discussion
The Aeroneb Go/Idehaler system demonstrated superior performance with respect to pulmonary aerosol delivery and optimal particle size while maintaining acceptable osmolarity. Although the Idehaler holding chamber is not yet licensed in North America, the Aeroneb Go is, and few problems are anticipated in getting regulatory approval for the Idehaler. The Pari LC Star has an appropriate particle size distribution but far too slow an aerosol output, and, further complicating the issue, the evaporative loss when driven by a dry hospital gas source rapidly lead to a hyperosmolar aerosol. The MicroAir had neither an appropriate output rate nor particle size distribution. Hence, the Aeroneb Go/Idehaler system best met the requirements of the planned clinical study.
Using a positive study by Ciarallo et al,27 the rate of intravenous MgSO4 administration with a dose of 40 mg/kg for a 25-kg child during a 20-min infusion would be 50 mg/min. With the Aeroneb Go/Idehaler, the MgSO4 aerosol delivery into the airway would be approximately one fifth that, or 11.2 mg/min, with the “infusion” lasting 16 min. Based on the hypothesis stated above, the high concentration of magnesium in the airway will facilitate diffusion into the interstitial tissue, which includes the airway and the airway capillary bed, from where it will be removed by the circulation. The expected result would be enhanced bronchodilation from the high interstitial concentration of magnesium, with a reduced risk of systemic hypotension because the circulating level would be lower. Since aerosol delivery is only a fraction of the systemic dose given intravenously, 2 more 16-min inhalations could be undertaken with little concern about systemic hypotension.
Limitations
The first limitation has to do with the prediction of in vivo deposition from an in vitro study where inhaled mass is captured on a filter. When the interface between the device and the subject is a mouthpiece and one way valves, an in vitro study can have inspiratory and expiratory filters so the fate of all the aerosol can be ascertained and a mass balance before and after nebulization can ensure the accuracy of the results. In this situation, as long as the breath simulator's breathing pattern is appropriate, discrepancies between what enters and stays in the body, compared to what is captured on the inspiratory filter, are due to aerosol that ends up in the patient's anatomical dead space and is exhaled onto the expiratory filter with the next exhalation. With a breath-enhanced nebulizer and a normal subject, the in vitro versus in vivo difference is small.28,29 However, the Idehaler system has no valves, and the small but significant resistance of the expiratory filter changed the fluid dynamics in the holding chamber and could not be used. Hence, the concept of mass balance before and after nebulization could not be implemented, and the accuracy of aerosol collection on the inspiratory filter could not be confirmed. Having recognized this, the low standard deviation, compared to the mean for the triplicate studies, would suggest that an error would have to be a systematic one to achieve that degree of repeatability. We recognize that the breathing patterns we used are those of normal children and may not be representative of the breathing pattern during an asthma attack, but there are no data to guide alternative choices.
Conclusions
Our data suggest that a 16-min nebulization of 6 mL of the MgSO4-plus-albuterol solution we used, with the Aeroneb Go/Idehaler setup and a face mask would maximize MgSO4 delivery to the airways in severe asthma and prevent bronchospasm due to aerosol hyperosmolarity and hypotension from systemic absorption. Therefore, we recommended this setup for the upcoming multicenter trial of inhaled MgSO4 in children with severe asthma.
Footnotes
- Correspondence: Allan L Coates MDCM, Hospital for Sick Children Research Institute, 555 University Avenue, Toronto, Ontario, Canada M5G 1X8. E-mail: allan.coates{at}sickkids.ca.
-
The authors have disclosed a relationship with Aerodrug, which is a department of La Diffusion Technique Francaise, Saint Etienne, France.
-
This research was partly supported by Paediatric Consultants Partnership grants from the Hospital for Sick Children Research Institute, Toronto, Ontario, Canada.
- Copyright © 2011 by Daedalus Enterprises Inc.





{kind=link}