

Abstract
We report a case of a 62-year-old male who presented to our intensive care unit with hypoxemia 6 hours after retinal surgery. He had a negative computed tomography (CT) pulmonary angiogram, but an emergency echocardiogram revealed the McConnell sign. He was thrombolysed and had rapid improvement in oxygenation and hemodynamics. Thrombolysis in hemodynamically unstable pulmonary embolism is not controversial, but most algorithms require confirmation of the diagnosis. Our patient had a negative CT pulmonary angiogram but was thrombolysed based on the clinical picture. Autopsy confirmed the diagnosis of multiple pulmonary emboli and unexpectedly discovered a patent foramen ovale that explained paradoxical embolism to the brain.
Introduction
Massive pulmonary embolism is associated with a mortality of up to 65% acutely.1 We present a patient who had a negative multidetector computed tomography (CT) angiogram but was nevertheless thrombolysed for acute pulmonary embolism.
Case Report
A 62-year-old white male with a history of hypertension, hyperlipidemia, and retinal detachment underwent an elective vitrectomy for tractional retinal detachment. Preoperatively his mobility was limited by poor vision, but he was ambulatory. His preoperative oxygen saturation was 97% on room air. The procedure was uneventful and he was ambulatory postoperatively. Six hours post-procedure he developed acute dyspnea with hypoxemia. He was transferred to the medical intensive care unit with an oxygen saturation of 80% while on 100% oxygen via non-rebreather mask, and was intubated and mechanically ventilated.
He had no known drug allergies. His medications included spironolactone 50 mg and atorvastatin 10 mg daily. He had retinal surgery 3 months prior. He had no history of tobacco, ethanol, or illicit drug use. On arrival in the intensive care unit, his temperature was 36.2°C, heart rate 134 beats/min, respiratory rate 25 breaths/min, and blood pressure 130/89 mm of Hg. He had an eye patch over the right eye. Auscultation found occasional crackles. Cardiac examination found tachycardia, normal heart sounds, and no murmurs. He had no abdominal distention or organomegaly. Before intubation he was neurologically intact. There was no lower-extremity edema. Electrocardiogram revealed sinus tachycardia but no right-ventricular (RV) strain.
At that point we considered differential diagnoses of acute pulmonary edema, massive pulmonary embolism (thrombotic or non-thrombotic), cardiogenic shock from acute myocardial infarction, and acute respiratory distress syndrome. A CT pulmonary angiogram showed no central intravascular filling defect, infiltrate, or pneumothorax, but the CT was limited by respiratory motion artifact. Initial blood tests were unremarkable, with a normal methemoglobin concentration. Two hours after admission to the intensive care unit his oxygenation worsened and he developed hypotension requiring vasopressors. An arterial blood sample revealed a pH 7.28, PaCO2 43 mm Hg, and PaO2 58 mm Hg while on pressure-control ventilation, FIO2 1.0, and PEEP of 15 cm H2O. He became increasingly hypoxic on those settings, and paralytics were initiated. An emergency echocardiogram showed that the left ventricle was hyperdynamic, there was severe right-atrial and RV enlargement and decreased RV function, but with sparing of the apex (the McConnell sign) (Fig. 1). Based on the high clinical probability of acute pulmonary embolism, he was given intravenous recombinant tissue plasminogen activator, despite the normal CT pulmonary angiogram.

Representative transthoracic echocardiogram showing a hypokinetic right ventricle with preservation of the apex (the McConnell sign).
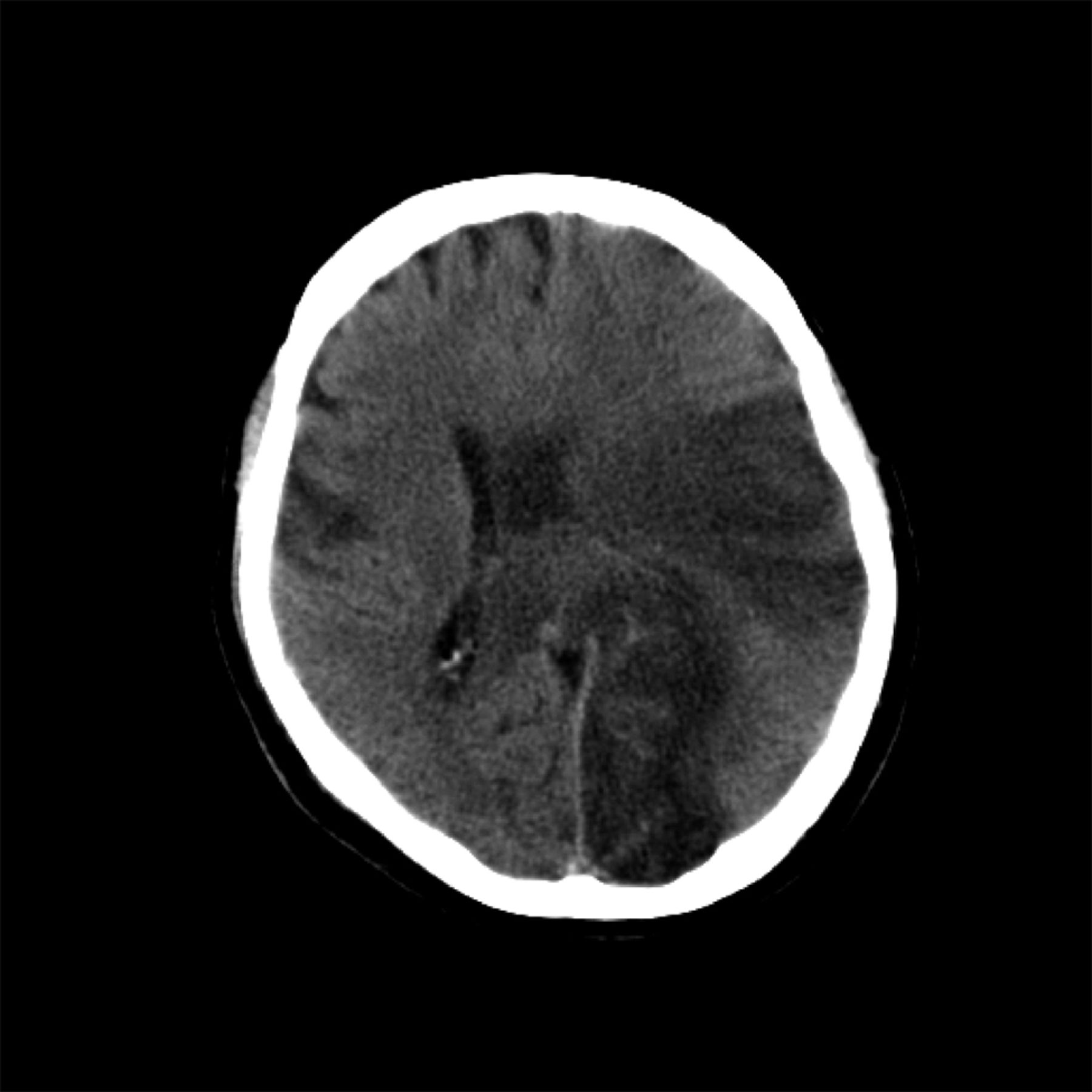
Later, upper and lower extremity venous Doppler ultrasound were negative for femoropopliteal thrombosis. The pelvic veins were not imaged by a venogram, and could well have been the source of pulmonary embolism. He was started on intravenous heparin, and contrast echocardiogram was repeated in 24 hours. The right atrium and right ventricle normalized, with no evidence of a shunt on a bubble study. Over the next 3 days he continued to improve hemodynamically. By day 5 he was off vasopressors and on FIO2 0.60 and PEEP 10 cm H2O. Once the sedation was discontinued, he was found to be unarousable, and he developed diabetes insipidus. An emergency brain CT revealed recent left middle and posterior cerebral artery infarctions, with a 15-mm midline shift (Fig. 2), confirmed by a subsequent magnetic resonance image (Fig. 3). His family decided to withdraw care. Autopsy revealed multiple sub-segmental pulmonary emboli and a patent foramen ovale.

Noncontrast computed tomogram of the brain shows hypodensities compatible with infarction in the left middle and posterior cerebral artery and right middle cerebral artery territories, with midline shift.

Magnetic resonance T2 axial flair image shows abnormal signaling in the left middle cerebral and posterior cerebral artery and right middle cerebral artery territories, with a midline shift.
Discussion
Little controversy exists in the administration of thrombolytic therapy for massive pulmonary embolism in hemodynamically unstable patients.2,3 Thrombolytic therapy decreases vascular obstruction by 12% at 2 hours, compared to heparin.4 It is established that RV dysfunction in pulmonary embolism is central to the patient's outcome acutely. Pressure overload from pulmonary embolism, resultant myocardial ischemia, poor left-ventricular filling and diminished cardiac output ultimately lead to cardiogenic shock, which, if not reversed promptly, results in death.5 Making a decision to aggressively treat acute pulmonary embolism becomes simpler if there is radiologic evidence of pulmonary embolism.
The Prospective Investigation of Pulmonary Embolism Diagnosis (PIOPED II) study, completed in 2006, reported that multidetector CT pulmonary angiogram had 83% sensitivity and 96% specificity in detecting pulmonary embolism. Notably, 40% of patients with a high clinical probability of pulmonary embolism had a negative CT pulmonary angiogram.6 PIOPED II and our case exemplify the Bayesian theorem of conditional probability, which states that the probability of disease depends on its pre-test probability and the sensitivity and specificity of the test.
Our patient had a high clinical likelihood of massive pulmonary embolism, an echocardiogram highly suggestive of pulmonary embolism (the McConnell sign), but a negative CT pulmonary angiogram. In that life-threatening scenario, recent ophthalmic surgery became a relative (not an absolute) contraindication to thrombolysis. The McConnell sign (regional variations of RV systolic wall motion abnormalities, with sparing of the apex), when prospectively tested in 85 patients, had a sensitivity of 77% and a specificity of 94% for the diagnosis of acute pulmonary embolism.7 More recently, Lodato et al reported the right- and left-ventricular end-diastolic dimension as the most accurate echocardiographic predictor of pulmonary embolism in patients referred for helical CT, but found the McConnell sign to be most specific (96%).8 This finding resolved in our patient after thrombolytic therapy. Unfortunately, our patient developed an unexpected complication of his initial diagnosis. Autopsy confirmed pulmonary embolism with paradoxical embolism to the brain via a patent foramen ovale. We postulate that the initial acute pulmonary embolism resulted in high right-side pressure, leading to paradoxical embolism and subsequent cerebral infarctions. This case emphasizes the importance of understanding the specificity and sensitivity of a test and applying it appropriately to a clinical scenario.
Footnotes
- Correspondence: Urvashi Vaid MD, Division of Pulmonary and Critical Care Medicine, Thomas Jefferson University, 834 Walnut Street, Suite 650, Philadelphia PA 19107. E-mail: urvashi.vaid{at}jeffersonhospital.org.
-
The authors have disclosed no conflicts of interest.
- Copyright © 2011 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}